1. Background
Functional constipation (FC) is a common disease in children, defined based on Rome ΙV criteria as delayed or difficult defecation for two weeks or more without any organic cause (1). About 3% of referrals to pediatricians and 25% of referrals to pediatric gastroenterologists are due to constipation (2). The prevalence of FC has been reported to be higher in South Asia and South America compared to other regions in the world (3). Among the factors predisposing vulnerable children to FC are urbanization, civil unrest, poor parenting skills, child maltreatment, and psychological distress (3). The troublesome symptoms associated with this disease, such as abdominal pain, as well as rectal and anal pain, can significantly compromise the quality of life of these patients. In addition, fecal incontinence (known as soiling or fecal leakage to underwear) can be a major concern that decreases children’s self-confidence and exposes them to social isolation and punishment by parents, leading to more psychological harm to these children (4). Overall, the chronic nature of constipation and unconstructive family performance can cause many behavioral problems, such as social isolation, low self-esteem, depression, aggression, anxiety, and, finally, decreased quality of life (5-7).
Anxiety disorders are among the most common disorders in children and adolescents, and social anxiety or social phobia is one of the most important of them (8). This disorder is a complex neuro-psychological syndrome that has been recognized as an independent diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM5) (9). Social anxiety disorder is a type of anxiety characterized by intense fear and anxiety in social situations caused by the fear of negative judgments by others. This highly debilitating type of anxiety interferes with many aspects of a person’s life. In young children, this type of anxiety may manifest itself as screaming, crying, or hugging relatives around them. On the other hand, older children and adolescents, when they face stressful social situations, experience panic-like symptoms. Individuals suffering from this disorder perceive social situations as annoying and try to avoid such situations as much as possible because they considerably hurt their professional, educational, and social functioning. In severe cases, social anxiety can considerably reduce the person's quality of life (10, 11). According to epidemiological studies, this disorder, in most cases, initially appears in childhood and adolescence, underlining the importance of this period to prevent and manage this disorder (12). The lifetime prevalence of this disorder in adolescents has been estimated between 10% and 15%, and girls have been reported to experience social anxiety disorder 1.2 to 2.1 times more than boys (10, 13).
Different studies have noted the role of psychological factors in the development and persistence of FC. Depression, anxiety, and panic have been described to be related to constipation in several studies (14-16). Social anxiety is believed to be rooted in the child’s low self-confidence, and also, chronic FC is associated with decreased self-confidence in children due to its behavioral problems. Therefore, investigating the relationship between the two disorders can open new ideas in explaining the psychological consequences of FC. However, no study investigated the relationship between social anxiety disorder and constipation in children, reporting inconsistent results on the relationship between these two. This is while if such a relationship is confirmed, patients can benefit from appropriate psychological and nursing interventions, which can have an essential role in taking care of the children (14).
2. Objectives
Altogether, we aimed to determine the prevalence of social anxiety in children with chronic FC. Our results can provide background data for planning appropriate preventive and therapeutic measures for these children.
3. Methods
In this cross-sectional study, children aged 10 to 17 years with chronic FC referred to Amirkabir Hospital in Arak, Iran, in 2022 were enrolled. This hospital is a specialized center for pediatrics. The inclusion criterion was the diagnosis of chronic FC, and the exclusion criteria were unwillingness to participate, concurrent gastrointestinal or other chronic diseases, taking any medications for constipation, the diagnosis of a psychiatric or chronic disease in parents, and raising the child in places other than the home.
After fully explaining the study’s objectives, the parents were requested to read and sign an informed consent form. The parents were also assured that their own data and their children’s would remain completely confidential to the researcher. Afterward, the necessary explanations were provided to the parents and children on how to complete the Social Anxiety Scale for Adolescents (SASA) (17), and finally, the questionnaire was completed by children under the guidance and supervision of their parents.
The SASA consists of 28 items, organized into two subscales: Apprehension and Fear of Negative Evaluation (AFNE) (15 questions) and Tension and Inhibition in Social Contact (TISC) (13 questions). This tool aims to measure adolescents’ concerns, fears, and avoidance behaviors in different situations and describes the concerns, fears, and expectations of possible negative evaluations by peers. The TISC subscale contains 13 questions that describe avoidance behaviors in social encounters, social tension, and readiness to face different social situations, such as participating in classroom discussions and communicating with familiar and unfamiliar individuals and opposite-sex counterparts. The questionnaire is scored in a 5-point Likert scale where the scores of 1, 2, 3, 4, and 5 are attributed to the responses of "very little", "little", "moderate", "much," and "very much", respectively. The items of 3, 4, 12, 17, 21, 25, 26, and 27 are scored in reverse. The total score of the questionnaire is calculated by summing up the scores of all items. A score between 28 and 56 indicates no social anxiety, and scores of 57 - 84 and > 84 reflect moderate and severe social anxiety, respectively.
The internal consistency of this questionnaire and its respective correlation coefficients obtained in test-retest in several studies have confirmed its validity. The results of confirmatory factor analysis also indicated the good fit of the two-factor structure to the data. The alpha coefficients for the subscales of AFNE, TISC, and the whole questionnaire were obtained as 0.84, 0.68, and 0.83, respectively (17, 18). Statistical analyses were performed in SPSS version 22 software. Central tendency and dispersion statistics were used to describe the data, and Chi-square test and independent sample T-test were used to compare anxiety scores between subgroups at a significance level of 5%. This project (No. 6040) received the ethical approval code of IR.ARAKMU.REC.1399.066 from the Research Ethics Committee of Arak University of Medical Sciences.
4. Results
In this study, 200 children aged 10-17 years with chronic FC were studied. The participants’ mean age (SD) was 13.43 ± 1.54 years, and boys constituted 51.5% of the participants. Regarding age groups, 59 participants were in the age group of 10 - 12 years, 81 were in the age group of 13 - 14 years, and 60 were in the age group of 15 years and older.
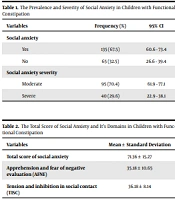
The lowest and highest social anxiety scores in these children were 35 and 127, respectively. The prevalence of social anxiety was obtained as 67.5% (95%CI: 60.6 - 73.4), of whom 70% had moderate anxiety, and 30% suffered from severe anxiety (Table 1). The mean (SD) scores of the AFNE and TISC subscales were calculated as 35.18 (10.65) and 36.18 (8.14), respectively (Table 2).
Table 1.
The Prevalence and Severity of Social Anxiety in Children with Functional Constipation
| Variables | Frequency (%) | 95% CI |
|---|---|---|
| Social anxiety | ||
| Yes | 135 (67.5) | 60.6 - 73.4 |
| No | 65 (32.5) | 26.6 - 39.4 |
| Social anxiety severity | ||
| Moderate | 95 (70.4) | 61.9 - 77.1 |
| Severe | 40 (29.6) | 22.9 - 38.1 |
Table 2.
The Total Score of Social Anxiety and It’s Domains in Children with Functional Constipation
| Variables | Mean ± Standard Deviation |
|---|---|
| Total score of social anxiety | 71.36 ± 15.27 |
| Apprehension and fear of negative evaluation (AFNE) | 35.18 ± 10.65 |
| Tension and inhibition in social contact (TISC) | 36.18 ± 8.14 |
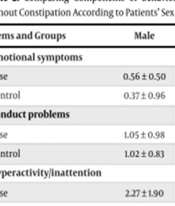
There was no significant difference in the prevalence of social anxiety between the age groups of children (P = 0.167). The prevalence of social anxiety was significantly higher in girls (74.8%) than in boys (59.8%) (P = 0.034). Also, girls showed significantly more severe social anxiety than boys (P = 0.023) (Table 3).
Table 3.
Comparison of Social Anxiety Divided by Gender in Children with Functional Constipation
| Variables | Social Anxiety | P-Value | |
|---|---|---|---|
| Yes, Frequency (%) | No, Frequency (%) | ||
| Sex | 0.034 | ||
| Female | 77 (74.8) | 26 (25.2) | |
| Male | 58 (59.8) | 39 (40.2) | |
| Age (y) | 0.167 | ||
| 10 - 12 | 39 (66.1) | 20 (33.9) | |
| 13-14 | 50 (61.7) | 31 (38.3) | |
| 15 and older | 46 (76.7) | 14 (23.3) | |
5. Discussion
In the present study, the prevalence of social anxiety in children with chronic FC was obtained as 67.5%, of whom 30% suffered from severe social anxiety, which could affect various life aspects of these children. In one study in Iran, the prevalence of anxiety was estimated to be 48% in adults with FC (16). However, we found no similar study in children with FC to compare our results. In healthy children, however, the prevalence of social anxiety has been reported to be variable depending on the studied population, demographic features, cultural characteristics, and the tools used. In a study by Farajollahi and Esmaeili on healthy middle-school students in Kermanshah, the prevalence of social anxiety was estimated at 18.80%, of which the frequencies of moderate, severe, and very severe disorder were 12.25%, 4.90%, and 1.70%, respectively. The results of this research indicated the considerably high prevalence of social anxiety disorder among middle-school students (19). In another study by Hassanzadeh aval et al. (20) on first-grade students in Malayer, it was noted that 26% of these students suffered from at least one type of anxiety disorder, and 11.7% had social anxiety disorder. In another study in Ethiopia on 17 - 12-year-old students, the prevalence of social anxiety disorder was reported to be 63%, which is a considerably high value (21).
In the current study, the prevalence of social anxiety was 65.2% in children aged 13 - 10 years and 69.4% in those aged 17 - 14 years. Although the prevalence of social anxiety was slightly higher in older children than in youngers, this difference was not statistically significant (P = 0.548). In general, specific phobias and separation anxiety seem to be more prevalent among pre-adolescent children, while social phobias and panic disorders are more common among adolescents (22). In a study evaluating about 30,000 Iranian children aged 6 - 18 years, the odd ratio (OR) of social anxiety was higher among older teenagers than other children (OR = 1.47, 95% CI: 1.11 - 1.95) (23). Likewise, studies conducted in the USA (24), Europe (25, 26), and Africa (21) have reported a higher prevalence of social anxiety disorder among older adolescents. This observation can be related to the transitional phase in physical and psychological growth and changes in appearance and emotions during adolescence, which can be reasons for increased social anxiety (23).
In the present study, we noticed that both prevalence and severity of social anxiety disorder were significantly higher in girls compared to boys. In the study of Achiko and Shikuro, girls in all age groups showed a higher rate of social anxiety disorder than boys (21). In line with the present research, the prevalence of social anxiety disorder was reported to be higher in girls than in boys in several other studies (20, 22, 27). Overall, females are more inclined toward self-focus and rumination when dealing with stressful life events, but males tend to deal with such events mostly through distraction, which can explain the higher rates of depression and anxiety disorders among women (28). Also, the fear of "doing something in front of others" is more frequently seen in girls than in boys (21).
In addition to factors such as older age group and female gender, other studies in this field have described roles for parents’ low income, low education, and being victimized by peers and misbehaviors and sexual abuse in the development of social anxiety disorder (21). The present study can pave the way for conducting more studies to investigate other determinants of childhood social anxiety disorders. It is suggested to appropriately organize and adequately provide mental health services to promote mental health and reduce social anxiety and its consequences in these children and society. In addition, the awareness of school counselors, teachers, and parents about social anxiety should be upgraded, and finally, effective interventions should be implemented to help these children overcome social anxiety (21). In this study, the questionnaire was completed by the children, so it is possible that they did not have enough accuracy in completing the questionnaires due to not fully understanding the concept of questions. In addition, although this center is a referral center for children, it may not be representative of all children. It is also suggested to conduct larger studies, including comparison of groups to consider the impacts of cultural, environmental, and other possible influencing confounding factors in order to adjust their effect.
5.1. Conclusions
In this study, the prevalence of social anxiety in children with chronic FC was found to be considerably high. There was no significant difference between different age groups in terms of the prevalence of social anxiety; however, the prevalence and severity of this disease were significantly higher in girls than boys.