
1. Introduction
Hypertriglyceridemia (HTG) and diabetic ketoacidosis (DKA) are complications of uncontrolled diabetes that may result in significant mortality or morbidity (1). Hypertriglyceridemia can be associated with primary/ genetic causes or secondary causes/ lack of insulin (2). In mechanism HTG, insulin deficiency activates lipolysis in adipose tissue and increases the release of free fatty acids (FFA) and amino acids from adipose tissue and muscle; increasing FFA uptake by the liver leads to increases in very low-density lipoprotein (VLDL) in the liver and decreases the clearance of VLDL from plasma. Thus, these factors lead to hypertriglyceridemia (3). Studies reported severe hypertriglyceridemia in about 8% of adults with DKA (4), but limited data have been found in children. We report a case of hypertriglyceridemia in a child 12 years old with diabetic ketoacidosis.
2. Case Presentation
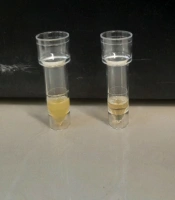
The 12-year-old boy patient was diagnosed with VACTERL syndrome due to accompanying anomalies (tracheoesophageal fistula, esophageal atresia, vertebral defects, renal and limb anomalies). He was referred to our center with polydipsia, polyuria, weakness, and lethargy. On admission, initial laboratory data were as follows; serum glucose 300 mg/dL, hemoglobin 9.6 g/dL, HbA1c 10.7%. cholesterol 980 mg/dL, TG13,520 mg/dL, low-density lipoprotein cholesterol (LDL-C) 396 mg/dL, sodium 142 mEq/Potassium 3.3 mEq/L and chloride 85 mEq/L. In arterial blood gas (ABG) analysis, PH was 7.21, Hco3 was 7.2 mmol/L, and anion gap was 27.2 mmol/L. In the liver function test, SGOT (AST) was 26 IU/L, SGPT (ALT) was 85 IU/L, AIK was 290 IU/L, Lipase 53, and Amylase 61. The serum sample was turbid and milky, indicating a lipemic state (Figure 1).

Photo of blood sample of the hyperlipidemic patient obtained by centrifugation in admission vs. blood sample after 3 days treatment
The patient was diagnosed with DKA, severe hypertriglyceridemia, and acute pancreatitis. Conservative treatment started, and the patient received insulin infusion at a dose of 0.1 units/kg per hour and FFP with a volume of 10 cc/kg for 3 days. After treatment, serum glucose and lipid profiles were analyzed. The results showed that serum glucose was 210 mg/dL, triglyceride was 4620 mg/dL, cholesterol was 950 mg/dL, and LDL was 377 mg/dL. HDL was 70 mg/dL (Figure 1) in the liver function test, SGOT (AST) was 26 IU/L, SGPT (ALT) was 85 IU/L), AIK was 290 IU/L, lipase was 53 U/L, and amylase was 61 U/L (blood sample in admission vs. blood sample after 3 days of treatment). After controlling blood sugar and triglycerides, the patient was placed on a fat-restricted diet, gemfibrozil, and medium-chain triglyceride (MCT) oil. One week after discharge, analyses revealed serum glucose 199 mg/dL, total cholesterol 210 mg/dL, triglycerides 238 mg/dL, LDL-C 115 mg/dL, HDL-C 59 mg/dL (Figure 2). In the liver function test, SGOT (AST) was 13 IU/L, SGPT (ALT) was 38 IU/L, AIK was 260 IU/L, Lipase 50 U/L, and amylase 68 U/L.

Photo of hyperlipidemic serum obtained by centrifugation in patient’s blood sample in admission vs. 1 week after discharge
3. Discussion
Hypertriglyceridemia is a rare complication during DKA which may increase the risk of acute pancreatitis (5). In our study, hypertriglyceridemia was caused by her HbA1c of 10.7%, indicating insulin deficiency for months. This disturbance is rarely diagnosed in children with DKA compared to adults (6, 7).
A review of studies of children with DKA and hypertriglyceridemia reported that a triglyceride level of more than 10 g/L is associated with a 5% risk of developing acute pancreatitis and an increase of more than 20 g/L with a 10 - 20% risk (5). In this case, we also suspected acute pancreatitis and evaluated pancreatic enzymes, which showed normal serum amylase and lipase, so we ruled out acute pancreatitis in this patient. In our case, management HTG includes insulin infusion (by stimulating lipoprotein lipase activity) and FFP. FFP as fluid replacement successfully reduced lipid levels without complications and the symptoms of patients in the acute phase of the disease (8). This is because FFP may provide circulating TG hydrolysis by reducing inflammatory cytokines and replacing the deficiency of lipoprotein lipase or apolipoprotein (9). Finally, in this case, we recommend having close monitoring throughout the time the patient receives the infusion of insulin and FFP. Our study has some limitations that include the false positive results of the laboratory, not paying attention to the patient’s NPO and limited facilities in our hospital.
3.1. Conclusions
Insulin and FFP injection is a safe, effective therapy for DKA hypertriglyceridemia, rapidly lowering dangerously high triglyceride levels and preventing untoward complications.
