1. Background
Bleeding may occur anywhere along the gastrointestinal (GI) tract and, seeing the blood in the child's stools, the caregiver and child may become extremely anxious, fearing a devastating diagnosis. Lower gastrointestinal bleeding (LGIB) is a serious and sometimes threatening condition in both infants and children, which can have a range of causes (1). LGIB is described as bleeding originating from the intestine distal to the ligament of Treitz which is placed at the junction of the duodenum and jejunum. LGIB in infants and children is an ordinary problem in medical centers; however, only a limited number of studies have been conducted on its epidemiologic properties. Epidemiological data on LGIB can present useful information for developing strategies to reduce the frequency of LGIB and direct the clinical management of the patients with LGIB. On the other hand, differences have been observed in the causes of LGIB in special geographical places, and, consequently, it is necessary to determine the etiology of LGIB in each local site. The etiology of LGIB is different in children and the adults and the causes are usually simple, and require little or no treatment, for example, anal fissure and juvenile polyps, but sometimes this symptom may indicate more severe and life-threatening conditions, such as intussusception, Meckle’s diverticulum, and midgut volvulus (1-3). The differential diagnosis of the LGIB in infants and children, however, includes numerous possibilities ranging from benign disorders, which require little or no treatment at all, to serious diseases that require immediate intervention.
2. Objectives
The present study aims to determine the main causes of LGIB in the patients below 18 years old at the pediatric clinics of Fars province, South of Iran.
3. Patients and Methods
All patients less than 18 years old with LGIB who referred to Pediatric Gastroenterology Ward affiliated with Shiraz University of Medical Sciences between 2005 and 2009, were enrolled in this cross sectional study. All the patients were categorized into four age groups of less than 2, 2-6, 6-10, and 10-18 years old. Differential diagnosis was carried out for each patient and the definite causes of the LGIB were determined using clinical and para clinical examinations. Age, sex and definite diagnosis of the underlying cause of LGIB were collected and analyzed.
3.1. Statistical Analysis
All values are presented as mean ± standard deviation (SD) with 95% confidence intervals. Statistical differences between the parameters were tested using Chi-square test. The Statistical analysis of the study data was carried out using the SPSS statistical software (V. 16.0) (SPSS, Chicago, IL, USA).
4. Results
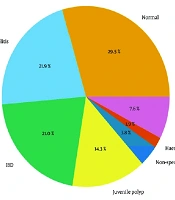
There were 309 cases with LGIB (185 males, 124 females). The demographic characteristics of these 309 patients are summarized in Table 1. There were 65 (21%) patients aged less than 2 years old, 140 (45.3%) patients aged between 2 and 6 years, 57 (18.4%) patients aged between 6 and 10 years, and 47 (15.2%) cases aged between 10 and 18 years. The most common causes of LGIB included colorectal polyps (n = 90; 29.1%), lymphoid nodular hyperplasia (n = 62; 20%), solitary rectal ulcer (n = 31; 10%), inflammatory bowel disease (n = 20; 6.5%), and anal fissure, hemorrhoids, Peutz Jegher syndrome, vascular malformations, juvenile polyposis coli, intussusceptions, Meckle’s diverticulum, and thrombocytopenia in 3.9% (n = 12) of the patients. However, the cause of hemorrhage remained undiagnosed in 94 (30.7%) patients. The etiologies of these 309 patients according to different age groups and sex are listed in Table 2. In comparison to the other groups, the prevalence of lymphoid nodular hyperplasia in the less than 2 years old group and colorectal polyps in the 2-6 years group were significantly higher than the other causes (P = 0.001). The most cases with inflammatory bowel diseases and solitary rectal ulcer were aged more than 2 years. On the other hand, no statistically significant differences were observed between males and females as well as different age groups regarding the means of the underlying causes of LGIB (P > 0.05).
Table 1.
Characteristics of the 309 PatientsWith Lower Gastrointestinal Bleeding
| Frequency | % | |
|---|---|---|
| Sex | ||
| Male | 185 | 60 |
| Female | 124 | 40 |
| Age | ||
| ≤ 2 | 65 | 21 |
| 2-6 | 140 | 45.3 |
| 6-10 | 57 | 18.4 |
| 10-18 | 47 | 15.2 |
| Etiology | ||
| Colorectal Polyp | 90 | 29.1 |
| LNHa | 62 | 20 |
| Solitary Rectal Ulcer | 31 | 10 |
| IBDa | 20 | 6.5 |
| Others | 12 | 3.9 |
| No obvious disease | 94 | 30.7 |
| Total | 309 | 100 |
aAbbreviations: LNH, Lymphoid nodular hyperplasia; IBD, Inflammatory bowel disease
Table 2.
Etiology of the 309 PatientsWith Lower Gastrointestinal Bleeding According to Different age Groups and sex
| Etiology | < 2 | 2-6 | 6-10 | 10-18 | Male, % | Female,% | Subtotal |
|---|---|---|---|---|---|---|---|
| Colorectal Polyps | 11 | 62 | 12 | 5 | 57, 63% | 33, 37% | 90 |
| LNHa | 28 | 22 | 5 | 7 | 37, 59% | 25, 31% | 62 |
| Solitary Rectal Ulcer | 2 | 10 | 9 | 10 | 19, 61% | 12, 39% | 31 |
| IBDa | 1 | 6 | 4 | 9 | 6, 30% | 14, 70% | 20 |
| Others | 7 | 3 | 1 | 1 | 8, 66% | 4, 34% | 12 |
| No Obvious Disease | 17 | 37 | 25 | 15 | 58, 61% | 36, 39% | 94 |
| Total | 66 | 140 | 56 | 47 | 185, 60 | 124, 40% | 309 |
aAbbreviations: LNH, Lymphoid nodular hyperplasia; IBD: Inflammatory bowel disease
5. Discussion
Lower GI bleeding is defined as bleeding originating from the intestine distal to the ligament of Treitz. Bloody diarrhea and bright red blood mixed or coating normal stool are the classic presentations of LGIB. Moreover, the LGIB accounts for approximately one-fifth of all the cases of acute GI bleeding (4). Farrell and Friedman (2005) reported the incidence of LGIB as 20.5 to 27 cases per 100,000 adults in the U.S. (5). Bai et al. (2010) investigated 160 studies which provided the data of 53951 patients with LGIB in china (6). Based on these studies, colorectal cancer, colorectal polyps, colitis, anorectal disease, and inflammatory bowel disease were the most prevalent etiologies of LGIB in the Chinese adult population. In another study in India, the main causes of LGIB (n = 64) were revealed to be colitis (n = 27; 42%) and colorectal polyps (n = 26; 41%) (7). In the present study, the most common causes of LGIB included colorectal polyps, lymphoid nodular hyperplasia, solitary rectal ulcer, and inflammatory bowel disease. Colonic diverticula, angiodysplasias, inflammatory bowel disease, and postpolypectomy bleeding have been suggested as the most frequent causes of acute LGIB in the epidemiologic studies on Western populations (8).
Different studies have reported different causes for LGIB. Nevertheless, the causes of LGIB in Eastern studies are somewhat different from the Western reports. For instance, in the systematic review performed by Bai et al. (6), colonic diverticula only accounted for 1.1% of all the 53951 Chinese LGIB patients. In the same line, it accounted for less than 1% of our study patients. Nevertheless, diverticulitis was the reported cause of GI bleeding in 17–40% of patients (9) and is an important cause of LGIB in Western populations. Inflammatory bowel diseases, including ulcerative colitis and Crohn's disease, are common causes of LGIB, usually apparent as bloody diarrhea (10). It was estimated that 6 percent of the patients with either Crohn's colitis or ulcerative colitis suffered from severe LGIB, as well (11, 12). In the current study, the prevalence of inflammatory bowel disease was 6.5 percent. Anal fissure is possibly the most general cause of rectal bleeding in infants and young children. In addition, colorectal polyps can be the cause of LGIB in preschool age and older children and inflammatory bowel disease is an important cause of LGIB which is highly prevalent among the younger children (school age children and adolescents) (13-15). Age can also provide a sign to the cause of acute LGIB; younger patients be predisposed to bleeding from hemorrhoids, vascular malformation, and solitary rectal ulcers, while older patients tend to bleed from diverticula, vascular malformations, and neoplasms (16).
In our previous study, of 256 children who were evaluated endoscopically for recurrent LGIB, 4.7% had solitary rectal ulcers (17). In the present study, solitary rectal ulcers were seen in 31 of 309 patients (10%) that may be due to better understanding and diagnosing of this entity. In adult patients, men and women are affected equally with a small predominance for women, but 75%-80% of children with SRUS are boys (18), as we see, 31 (10%) cases of solitary rectal ulcers in the current series show that 61% were boys and 39% were girls. In the present study, colorectal polyps were the most prevalent causes of LGIB among the children. Similar to our study results, in the studies conducted by Bai et al. (6) and Perisic (19) on the children with LGIB, the prevalence of colorectal polyps was higher than the other causes. Rafeey M (20) in a study on 59 children with LGIB reported polyps as a cause of LGIB in one third of patients. In another study in Iran, of 164 colonoscopies, 34.7% of LGBI were due to polyps which was the most common etiology followed by lymphoid nodular hyperplasia (22.5%) (21). Bai et al. (6) found that the proportion of colorectal polyp induced LGIB increased with the patients’ age. In our study, the prevalence of colorectal polyp in the 2-6 years old group was higher in comparison to the other groups. Lymphoid nodular hyperplasia is part of the generalized lymphoid hyperplasia associated with viral infections in infancy and childhood and immunodeficiency states as a cause of the lymphoid hyperplasia should always be excluded by estimation of serum immunoglobulin (22). Capitanio MA et al. (23) reported a rectal bleeding caused by the lymphoid hyperplasia. Lymphoid nodular hyperplasia should be considered as a differential diagnosis of LGIB in every infant who presents with LGIB under age of 2 years especially in breast fed infants. About 30.7% of colonoscopies was non-diagnostic in this study which is within the range reported in other studies; the study done by Clarke, et al (24) reported 30% normal results; another study conducted in this center revealed a prevalence rate of 23% of normal colonoscopy and Mandhans (25) reported a rate of 10.6%. Colonoscopy, even in the best centers of the world cannot find any abnormality in 10%–30% of patients with LGIB that might be attributed to several causes such as hidden positions of lesions between intestinal folds, incomplete colonoscopy since poor bowel preparation and presence of lesions are not examined segments, auto-amputation of polyps and repaired ulcer or other lesions before performing the procedure (21). Despite many reports on the identification and management of LGIB in the Western literature, relatively few reports from Asian countries have been published. Besides, there is limited information on the epidemiology of LGIB in Iran and the present study is one of the few one carried out on this topic on the Iranian patients. In spite of all the limitations, we suggest that the present study could be used by the Iranian physicians in order to gain an overall picture of LGIB in this part of Iran and guide the management of the patients with LGIB.