


1. Background
Fertility and child bearing is very important part of human life and it is important from social and psychological aspects (1). on the opposite side, infertility and the inability to carry out the normal reproduction process is a bitter and painful experience in life. The background and psychological and social conditions can increase its importance and turn it into a crisis for the individual (2).
The conducted studies introduce infertility as an unfortunate experience, especially for women, because motherhood has been accepted as an essential role for women (3). Infertility is a major crisis and a cause of mental stress that can cause emotional stress and a range of negative psychological reactions, including depression, anxiety, etc. (4). So, the prevalence of depression in infertile people is higher than the whole society (5).
Infertility is considered a multifactorial problem. One of the critical factors of infertility is a lifestyle. One of the critical factors of infertility that is rarely paid attention to is a lifestyle. By choosing a lifestyle, a person performs actions and activities to maintain and improve his health and prevent diseases, such as following a proper diet, sleep and rest, exercising and controlling body weight, not smoking and alcohol consumption, and immunization against diseases. This collection forms a lifestyle. Every person with good daily life pattern can enjoy physical and mental well-being. By following a health-oriented lifestyle, he can quickly and far from the enormous costs of infertility treatments, and prevent this problem (6). On the other hand, promoting lifestyle is one factors that affects the psychological phenomenon of depression and is a useful source for reducing the stressful factors of life and improving the quality of life (7).
Another risk factor in the life of depressed people is relationships and social actions. The type of relationships and social actions is one of the critical indicators in identifying adults at risk of depression (8). In a research conducted on American adults regarding social support, social pressure and relationship quality measurement over ten years, The results showed that depression is more prevalent in people who have low social support. Also, the low quality of relationships with spouses and family independently increases the risk of depression (9). Having appropriate emotional relationships with spouses and friends, as well as the ability to communicate and interact constructively with all members of society, have been introduced as criteria for emotional and communication skills in the discussion of health and prevention of mental disorders, which further shows the importance of social health (10). In addition to mental health, social health also affects other dimensions of health. Based on the studies conducted, social health is related to reproductive ability. In this regard, Bayani et al. conducted a study comparing the social health status among fertile and infertile women and concluded that some dimensions of social health, such as social solidarity, social acceptance and social participation, show a significant difference between fertile and infertile women, and women infertile people were at a lower level of these components. From these results, it can be concluded that society considers a part of the development process of women's personality and identity dependent on playing the role of mother. Infertility and lack of motherhood experience create a negative attitude and judgment of society about infertile women and can seriously challenge women's social health level (11).
2. Objectives
Considering the importance of infertility in society and its effect on mental health, especially in infertile women, as well as the impact of social and lifestyle factors on depression and infertility, the present study was conducted to determine the frequency of depression and its relationship with the components of social health and healthy lifestyle in infertile women.
3. Methods
The current research is a descriptive, analytical, correlation study conducted with the ethics ID IR.KUMS.REC.1400.717. The number of samples was determined based on the prevalence of depression in infertile women and referring to 360 related articles. Sampling was done according to the entry criteria and the census method. In this research, the purpose was first explained to the samples, and after completing the consent form, they entered the study. First, using the Beck Depression Questionnaire, infertile women with depression were identified, and then the samples whose depression score was eight or higher were entered into the study. In the next step, they completed the demographic information form, Keyes' social health questionnaires, and the health-promoting lifestyle of Valkroplerki. The information in the questionnaires was extracted, and the correlation between the influential factors and depression was analyzed using descriptive statistics and, Kolmogorov-Smirnov tests, Pearson's correlation.
The shortened Beck Depression Questionnaire has 13 questions; the validity and reliability of the Persian version have been confirmed (12) based on a 4-point Likert scale from 0 to 3, and the minimum and maximum total points of the references are from 0 to 39.
The Valkropyrylaki enhancing lifestyle questionnaire consists of 52 questions in the format of 6 areas: nutrition, physical activity, responsibility for health, stress management, interpersonal relationships and spiritual growth. A 4-point Likert response scale (never, sometimes, often, and usually) indicates how often a person performs specific health-promoting behaviors. The health- promoting lifestyle score and the behavioral dimensions are calculated using the average answers for all 52 questions and for each area (8 to 9 items). Validity. The reliability of the Persian version of the enhancing lifestyle questionnaire has been confirmed (13).
Keyes social health standard questionnaire has five areas, including: social prosperity, social solidarity, social cohesion, social acceptance and social participation and 20 items and scale or measurement level: Likert 5 options (completely agree, agree, neither agree nor disagree, disagree, disagree entirely) each of which is given from one to five points. The total scores of the questionnaire, the full scores are added together, and higher scores indicate higher social health. The validity and reliability of the Persian version of the Keys Social Health Questionnaire have been confirmed (14).
10 members approved the researcher's form made of demographic information of the academic staff of the departments of gynecology, midwifery and psychology.
In order to analyze the data, descriptive statistics and Kolmogorov-Smirnov tests were used for the normality of the data and Pearson's correlation coefficient was used for the correlation between the research variables. P-value < 0.05 was considered stasistically significant.
4. Results
The highest frequency (61 persons) corresponds to the age of 37 years (16.9 percent), and the lowest frequency (1 person) corresponds to the age of 47 years and 49 years (0.3 percent). Nnumber of 357 people, equal to 99.2% of the women participating in the research, were homemakers and 0.8% were employees. The education level 13.9% of elementary school and, 34.2% of middle school, 23.3% of secondary school, 27.5% of diploma and 1/1 bachelor's degree. None of the women participating in the research have a history of underlying disease, none of them have a history of depression, and none take medication.
Table 1 shows the mean and standard deviation of the components of social health social correlation, social coherence, social participation, social acceptance, and social prosperity. Skewness and kurtosis indices are between -2 and +2, which indicates the normality of the data.
| Variables | Frequency | Mean ± SD | Skewness | Kurtosis |
|---|---|---|---|---|
| Social health | 360 | 61.54 ± 8.94 | 0.56 | 0.89 |
| Social correlation | 360 | 8.73 ± 2.69 | 1.45 | 99 |
| Social coherence | 360 | 9.60 ± 3.27 | 0.65 | 0.78 |
| Social participation | 360 | 15.89 ± 4.02 | 1.23 | 1.71 |
| Social acceptance | 360 | 16.08 ± 3.75 | 0.62 | 0.69 |
| Social prosperity | 360 | 11.23 ± 2.49 | 0.45 | 0.12 |
Descriptive Statistics of the Social Health Variable
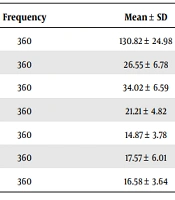
Table 2 shows the mean and standard deviation of the components of lifestyle, nutrition, exercise, responsibility, stress management, interpersonal support, and self-actualization. Skewness and kurtosis indices are between -2 and +2, which indicates the normality of the data.
| Variables | Frequency | Mean ± SD | Skewness | Kurtosis |
|---|---|---|---|---|
| Life style | 360 | 130.82 ± 24.98 | 0.45 | 0.78 |
| Nutrition | 360 | 26.55 ± 6.78 | -0.58 | -0.36 |
| Sport | 360 | 34.02 ± 6.59 | 1.12 | 0.89 |
| Responsibility | 360 | 21.21 ± 4.82 | 0.95 | 0.10 |
| Stress management | 360 | 14.87 ± 3.78 | 0.69 | 0.75 |
| Interpersonal support | 360 | 17.57 ± 6.01 | 0.36 | 0.52 |
| Self-actualization | 360 | 16.58 ± 3.64 | 1.20 | 1.55 |
Descriptive Statistics Related to the Promoting Lifestyle
Table 3 Pearson's correlation coefficient showed that depression is negatively correlated with social health (r = -0.55, P < 0.01) and lifestyle (r = -0.41, P < 0.01). Also, social health is positively correlated with lifestyle (r = 0.52, P < 0.01) (Table 3).
| Variables | Depression | Life Style | Social Health |
|---|---|---|---|
| Social health | -0.55 | 0.52 | 1 |
| Life style | -0.41 | 1 | |
| Depression | 1 |
Pearson Correlation Coefficient Between Research Variables
5. Discussion
This research aims to investigate depression and its relationship with the components of social health and a healthy lifestyle in infertile women. To achieve this goal, the present research was set up in the format of two hypotheses. The first hypothesis proposed the relationship between depression in infertile women and lifestyle components. According to the research findings, there was a significant relationship between depression variables and enhancing lifestyle (P < 0.01). Therefore, the first hypothesis of the study was confirmed. Among the components of lifestyle, exercise, responsibilit, and interpersonal support had a stronger relationship with depression, which can take more advantage of these effective components in the occurrence of depression and strengthen them in reducing the depression of infertile women The results were similar to those of Gatezadeh et al (12).
In this regard, Skandari et al. showed in a study that lifestyle directly affects depression. Because the way of life is defined as reflecting the tendencies and values of a person or group, the way of life includes a set of perceptions, values, ways of behaving, moods and tastes in everything. Health requires promoting a healthy lifestyle. The importance of lifestyle is more because it affects the quality of life and disease prevention. To maintain and promote health, correcting and improving lifestyle is necessary (13). Niki's part of promoting a health-oriented lifestyle, effectively reduces and adjust infertility problems of infertile couples (14).
Alizadeh et al. consider stress management, exercise, and smoking reduction as the most important factors affecting women's mental health (15). The only common component in Alizadeh's study and the present study was exercise, and there were differences in other components, which may be due to the difference in the research community of the two studies, because their study was conducted on all women. But in infertile women, interpersonal support and responsibility become more critical.
Also, in a study conducted by Behdani et al. under the title of the relationship between lifestyle and depression and anxiety in Sabzevar students, they concluded that there is an inverse relationship between lifestyle and depression, which means that the more favorable the lifestyle, the lower the level of depression (16). The findings were in line with and confirmed the results of the present study.
About the second hypothesis of the research, which stated the relationship between depression in infertile women and social health components, the research findings showed a significant relationship between social health and depression (r = -0.55, P < 0.01).
Based on the findings of this research, the components of acceptance and social participation showed a stronger relationship with depression in infertile women, which is in line with the results of the study by Bayani et al. that the tendency towards negative emotions such as anxiety and depression in women reduces their social cohesion and connection with their peers. Their social health is exposed to danger (11).
5.1. Conclusions
The results of this study determine the importance of mental and social health and the prediction of factors that lead to the creation and control of depression and the necessity of paying attention to the lifestyle of people to change and improve their lifestyle and identify people with depression. Therefore, it is suggested that social health and promoting lifestyle be given more attention as an important and effective indicator of infertile women's health.
