




1. Background
Today, despite the progress of human societies in various fields, competition in various issues has increased mental and emotional pressures in society. So that trying hard to reach a goal increases anxiety and physical and mental pressure and causes fear in these people (1). In addition to ordinary people in the society, the competition in athletes is also seriously observed and many athletes face these problems in order to maintain superiority and achieve success, and this causes more training, injuries and nutritional disorders (2). During the past years, the participation of women in sports activities has increased from a recreational and competitive aspect. And research on three million American sportswomen showed that these women are physically and verbally healthier and more self-confident than non-athletes (1). However, despite the fact that the health of these women has been reported, it seems that these women are more susceptible to nutritional disorders, menstrual disorders and even osteoporosis due to the increased pressure of competitive training (3). When coupled with inadequate nutrition, high energy expenditure and physical activity lead to tolerance of reduced available energy conditions. The peak of these critical conditions has been defined as the triple complication of female athletes by the American University of Sports Medicine (3). In addition, researchers have shown that physical activities in female athletes are related to menstrual disorders through mechanisms such as changes in estrogen levels (4). Therefore, this risk not only in elite female athletes but also in women and girls who do amateur physical activity may cause acute physical and mental disorders and even lead to quitting sports (5). However, there is no precise mechanism to explain what leads to the fact that girls and female athletes who participate in different levels of sports are not at risk of suffering from these complications.
The prevalence of eating disorders is higher among female athletes than among non-athletes, especially among those in sports where thinness and weight loss are important to them, they believe that they will perform better if they are thin. For this purpose, they spend a lot of time in intense activity and without food (6, 7). Eating disorders are abnormal eating habits that try to keep their weight lower than normal with diet or intense sports activity (8). Although they often do not admit that they are sick, people with eating disorders have complex and serious anxieties in their eating behaviors. Their preoccupation is often about body shape and weight and poor eating habits.
In the process of losing weight, people use methods such as extreme hunger and gluttony and nausea with different drugs. They experience caloric restriction by reducing food intake and improper use of diet pills and long-term fasting (9). Therefore, nutritional disorders lead to dehydration, muscle fatigue, irregular heartbeat, kidney damage and other serious complications (9, 10). Meanwhile, insufficient consumption of calcium leads to a decrease in bone density, this situation appears when a person is in adolescence and has the greatest need for calcium to build bones. Hormonal imbalance, which mostly leads to a decrease in bone density, occurs during menstrual cycle irregularity (4, 5). Many female bodybuilders experience irregular menstrual cycles while preparing for sports competitions. This disorder in the menstrual cycle is seen more among athletes in fields such as: Marathon runners, swimming, weight lifting, ballet and cycling. According to researchers, amenorrhea is seen 20 times more than normal people among female athletes, and it is also reported that 50% of female athletes’ experience amenorrhea (5).
Although there are several hypotheses that describe the mechanism and cause of amenorrhea, most researchers agree that it occurs due to hypothalamus dysfunction and any disorder in the secretion of gonadotropins affects ovulation and the menstrual cycle. which is related to the reduction of bone mineral density in them and increases the risk of fractures in women (4). For example, in a study, it was reported that 50% of Pakistani elite athletes had eating disorders, 83.3% of these women had Disordered Eating behaviors in need of referral, and 15% of them had amenorrhea and low bone density (11). Also, in a study by Taim et al. in 2023, they showed that 32.3% of the tested athletes had dysmenorrhoea, 85.6% had menstrual disorders, and most of them had psychological disorders and mood changes during the period of monthly habits (2). On the other hand, the prevalence of these complications depends on various factors such as the level of awareness of coaches and athletes, diet, hormonal disorders, etc. (12). Considering that the effect of triad disorders on the performance of athletes has been proven, but by looking at the background of the research, it can be seen that the social and cultural level, lifestyle and knowledge of people have a special contribution to the occurrence of triad disorders in female athletes. Therefore, investigating the prevalence of triple complications at an academic level can lead to more accurate information in this field. Therefore, the aim of the present study was to investigate the prevalence of triple complications among female athletes of Isfahan University.
2. Objectives
Therefore, the aim of the present study was to investigate the prevalence of triple complications in female college athletes.
3. Methods
In this causal comparative design, in which the prevalence of triple complications in female athletes of Isfahan University was cross-sectionally investigated, first by obtaining permission from the Vice-Chancellor of Education of Isfahan University, from all the athletes of this university to participate. In the following, during a meeting, all the conditions, advantages and ethical aspects of participating in the test were explained to the subjects. Then, among these people, 141 female athletes with an age range of 19 - 25 years from different sports disciplines were selected as a statistical sample. It is worth mentioning that 27 of these participants were futsal players, 36 were handball players, 9 were track and field athletes, 24 were volleyball players, 33 were basketball players, and 12 were martial artists. It is worth noting that certain diseases, the use of effective drugs, injuries were the criteria for leaving the present study. In this study, they were given a self-assessment questionnaire to assess their height, weight, age, age of starting activity, menstrual status, fracture history, and exercise program. Regarding the menstrual status, they were asked details about the frequency, regularity or irregularity of the menstrual cycle. Regularity of the menstrual cycle. It was defined as a period that does not occur during 28 - 34 days for subjects, and immunourea was defined as people who had no irregularity in the menstrual cycle during the past year. And primary amenorrhea is the absence of menstruation at the age of 16, and secondary amenorrhea is a cycle that does not occur for three or more months after the first menstruation. Body mass index was evaluated with a scale of weight in kilograms and height squared in meters. The subjects were people who did not take birth control pills.
Questionnaire EAT-26, behaviors related to nutritional disorders with a 26-item nutritional attitude test questionnaire (EAT-26) are measured. Also, based on previous studies, Cronbach's alpha coefficient of EAT26 questionnaire was calculated as 0.74. The validity, reliability, and validity of this test have been determined on a group of athletes, and in this authentic questionnaire, it actually measures the behaviors related to unhealthy eating, attitude, and thinking in people. It has three subgroups, which are dieting, Nervous overeating is controlled by taking different drugs. Likert Scale was used to answer this questionnaire so that the frequency of scoring the answers was 0 - 3. The score is 0 = never and always = 3. It should be noted that a score equal to or higher than 20, EAT > = 20 It indicates the presence of nutritional disorder behaviors in a person. Athletes whose score is higher than 20 and have subnormal weight should be referred to a doctor and the necessary tests to check their bone density should be measured.
Shapiro-Wilk test was used to check the data distribution. Independent t-test was used to check the difference in EAT26 score between athletes and non-athletes. Also, one-way analysis of variance test was used to check the difference between different sports disciplines. Data were analyzed in SPSS26 software (P ≤ 0.05).
4. Results
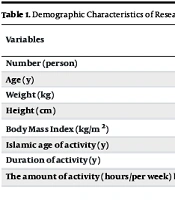
Comparison of general characteristics in athletes who have a disorder in the menstrual cycle or have a regular cycle is shown in Table 1.
| Variables | Mean (Standard Deviation) | |
|---|---|---|
| Menstruation Regular | Menstrual Cycle Irregular | |
| Number (person) | 129 (91.48) | 12 (8.51) |
| Age (y) | 67.21 (1.25725) | 50.21 (2.39317) |
| Weight (kg) | 37.58 (5.41709) | 50.54 (6.11258) |
| Height (cm) | 20.166 (4.86773) | 50.164 (4.33799) |
| Body Mass Index (kg/m2) | 26.21 (2.17382) | 09.20 (1.86049) |
| Islamic age of activity (y) | 15 (3.24037) | 75.16 (1.86474) |
| Duration of activity (y) | 93.3 (255750.) 81.2 (39066.0) | 75.3 (45227.0) |
| The amount of activity (hours/ week) bottom | 9.3 b (9.0869) | (3 00000.0) 13.5 b (4.926) |
Table 2 the score EAT-26 has been compared in two groups of athletes with regular menstruation and with irregular menstruation, as well as individual and team athletes. As can be seen, its value was different in the two groups of athletes with regular and irregular menstruation (P ≤ 0.05), but in the two groups of team and individual athletes, its value was almost the same and there was no significant difference (P ≥ 0.05).
Score EAT-26 in Two Groups of Athletes with Regular and Irregular Menstruation
Determining the general characteristics and density of bone mineral solutes in 6 groups of subjects who met the triple complications criteria examined. The results showed that there is no significant difference in the overall score and density of bone minerals in 6 groups (P ≥ 0.05) (Table 3).
| Toll Road | ED + A + OPO | ED + A + OPO | ED + A + OPO | ED + A + OPO | ED + A + OPO | ED + A + OPO |
|---|---|---|---|---|---|---|
| Sports Fields | Handball | Futsal | Basketball | Volleyball | Athletics | Martial Art |
| Number | 36 | 27 | 33 | 24 | 9 | 12 |
| Age | 50.21 | 67.21 | 82.21 | 22.38 | 20 | 50.21 |
| Height | 67.166 | 11.165 | 64.166 | 38.169 | 167 | 75.163 |
| Body Mass Index | 8.20 | 25.21 | 64.22 | 12.20 | 78.18 | 92.21 |
| Age of starting exercise (y) | 15.08 | 12.89 | 17.09 | 13.75 | 18 | 15.75 |
| Sports history (y) | 4 | 4 | 4 | 4 | 3 | 75/3 |
| Training per week (h) | (75 - 2) | 3 | (91 - 2) | (75 - 2) | 3 | 5/2 |
| Bone density score at thigh neck | 0.044 ± 1.063 | 1.161 ± 0.081 | 0.032 ± 1.084 | 0.041 ± 1.094 | 0.023 ± 1.032 | 1.151 ± 0.046 |
| Bone density score at lumbar 2 - 4 beads | 1.200 ± 0.073 | 166 ± 0.269 ± 1 | 1.212 ± 0.059 | 1.205 ± 0.036 | 1.122 ± 0.053 | 105.0 ± 224 ± 1 |
General Characteristics and Density of Bone Mineral Solutes of Subjects
5. Discussion
The current research showed that athletes with irregular menstrual cycle had lower weight and Body Mass Index and more training time per week compared to people with regular menstruation. However, the risk of eating disorder behaviors was not observed among any of the subjects, considering that their score was lower than 20. Triple complications in women athletes have three components of disorders related to eating, cessation of menstruation and reduction of bone density (13, 14). In this context, researchers have shown that elite female athletes, those who participate in sports such as endurance running and gymnastics, or disciplines that depend on reducing body fat percentage and weight control, experience these complications more than other athletes (5, 15). Although the activity in many sports that requires weight loss has many advantages, but in addition to these advantages, severe weight loss may cause problems for health and performance. Sudi et al. states in the research he conducted that in athletes with anorexia nervosa, calorie restriction and intense activity to maintain body weight and reduce fat percentage often lead to severe complications (16). Most studies show that triple complications are more common in athletes. It seems that the level of education and knowledge of university girls is higher than others. Therefore, the contradiction in the results of the studies can be due to the difference in the level of education and personal characteristics. In addition to the benefits of such activities, its negative effect is the cessation of menstruation, when athletes eat little food and do intense activity, hormonal changes caused by poor nutrition lead to irregularity in the menstrual cycle (17). Irregularity in the menstrual cycle is the most common disorder among female athletes, which is more common in slender athletes (13, 18). The highest rate of sports amenorrhea is among endurance runners and ballerinas, which is reported above 0.66% (12). In the current research, the prevalence of triple complications among university athletes was done and the risk of this condition was not observed in them. However, due to the pressure of training and the amount of work, menstrual cycle disorders and its interruption are important predictors that can lead to injury to athletes and ultimately decrease bone density in the long term, and the highest rate of these irregularities is reported among runners became.
One of the prominent features of people with anorexia nervosa is the occurrence of menstrual periods during sports periods. Disorders related to eating are manifested by weight loss or extreme diet along with sports performance (19). Athletes who seem to have the highest risk of menstrual cycle irregularity usually had their training before the start of their first period and followed a hard and intense training program and a low calorie diet to prevent weight gain (20). These results were consistent with the results of our study. Osteoporosis has a serious effect on women's health, amenorrhea and weight loss are two factors that are important predictors of bone loss (21). The places where the decrease in density is measured and most of the compression fractures are seen in them are in the waist, thighs and lumbar vertebrae (11). According to researchers, the highest rate of osteoporosis has been reported in people with nutritional disorders (12, 22). Poor nutrition and disorders related to eating and irregularity in the menstrual cycle have a negative effect on the health of the skeletal system, consuming enough calcium and vitamins D. Along with eating enough food, it is a guideline to prevent osteoporosis (16). According to nutritional recommendations, daily calcium intake for women aged 19 - 30 with regular menstrual cycle is 100 mg per day, while for people with low or no menstruation, it is 1500 mg per day (19). McCloud state in their research that 15 - 65 percent of women who participate in individual disciplines have shown eating disorders, while in our studies there is a significant relationship between the score of eating disorders and sports. Individuals were not observed (23). According to the results of our study and the comparison of these results with other studies, it seems that considering the level of education is one of the important pillars of investigating the prevalence of triple convulsions in girls. Also, some personality traits that are necessary for success in sports, such as perfectionism and a sense of superiority, high expectations and independence are risk factors for eating disorders. People who used these methods faced a drop in performance. Eating disorders in athletes whose mental preoccupation is related to body weight and self-dissatisfaction have lower depression and self-confidence (13, 23). Nevertheless, the present study states that the subjects did not show the complications of eating disorders, but in the comparison of the mean scores of the subgroups in dissatisfaction with their body and the desire to lose weight, runners reported the highest score compared to other sports groups. This is consistent with McCloud's research. Due to the fact that the sports history of the people under our study does not reach more than 4 years and considering the fact that they did not use diuretic drugs for nutritional control and reducing food absorption in the body, they did not have severe bone density problems.
