



1. Background
Atherosclerosis is a pathologic condition that directly affects obesity and overweight, and is associated with the thickening of the inner layer of vessels caused by fat deposits and platelets (1). The progression of atherosclerosis disrupts the blood supply to the brain and other organs (2). A major function of vascular endothelial cells is the secretion regulation of growth factors such as VEGF, which plays a key role in the process of blood supply and angiogenesis, and is negatively correlated with obesity and atherosclerosis (3). Research suggests that stimulants such as hypoxia and training can increase the stimulation of VEGF (4), and the shear stress due to blood flow is a major cause of endothelial vascular endothelial growth factor (VEGF) secretion (5). Obesity reduces the vascular endothelial function, and is associated with impaired mechanisms, including lipid metabolism and hypertension (6). A review study demonstrated correlations between the femoral arterial thickness and factors involved in atherosclerosis, including ankle-brachial index (ABI) and cholesterol (7).
Different training methods proposed in recent years to prevent and treat obesity and overweight-associated diseases include the new method of training under hypoxic conditions. Research suggests improvements in the metabolism of fats and carbohydrate in hypoxic conditions (8, 9). Resistance exercise significantly increases the metabolic and angiogenesis responses, and adding a hypoxic stimulus has been proposed for increasing metabolic and angiogenesis responses to resistance exercise (3, 10, 11). Women with breast cancer showed significant increases in the level of VEGF, fibroblast growth factor (FGF) and nitric oxide (NO) after eight weeks of resistance training (12). A significant decrease was also observed in VEGF in female older adults after eight weeks of resistance training (13). In other study, for angiogenesis factors in healthy subjects, the eight weeks of resistance training under hypoxic conditions had significantly higher level of VEGF and capillary ratio to muscle mass than the normoxic resistance training (3).
Some researchers have reported improvements in terms of the effect of resistance training on lipid profile and some have demonstrated the lack of significant changes. The correlation between training intensity and changes in lipid profile have also been demonstrated (14, 15). A study of six-week aerobic exercise under hypoxia in two groups with 14.5% and 16.5% oxygen saturations found a significant increase in high density lipoprotein (HDL) levels and a significant decrease in low density lipoprotein (LDL), triglyceride (TG) and total cholesterol (TC) compared to the normoxic resistance training group (16). The chronic effects of hypoxia and hypoxic resistance training on these factors have rarely been addressed in literature. Given the effectiveness of hypoxia in angiogenesis and lipid profile, resistance training under hypoxia conditions can increase arterial responses to resistance exercise.
2. Objectives
The present research was therefore performed to evaluate and compare the effects of eight weeks of hypoxic and normoxic resistance training and hypoxia exposure on arterial factors in overweight men.
3. Methods
3.1. Participants
Thirty overweight none-athletic males in Kermanshah voluntarily participated in the present study. The subjects had no history of cardiorespiratory diseases and had not gone to altitudes of over 2500 meters in the two months prior to the intervention. They also visited the research laboratory of the Faculty of Physical Education of Razi University in Kermanshah two days before the intervention to get familiar with the study procedure, 1RM and demographic measurements. In addition, informed written and oral consent was obtained from all the subjects, and they were informed of any potential risks associated with the experiments.
3.2. Study Design
The subjects participated in 24 sessions of training protocols and hypoxia exposure, three sessions a week. The subjects were randomly assigned to three groups, namely hypoxic resistance, normoxic resistance and hypoxia exposure, the day they visited the laboratory. The maximum repetition of resistance was determined for squat and lunge using submaximal repetitions up to fatigue as follows (14).
The levels of VEGF, LDL, HDL, TG and TC were measured one day before and two days after the eight-week intervention.
3.3. Normoxic Resistance Training
This training program initially began by performing five minutes of stretching and warm-up exercises and a 15-repeat set with about 50% of 1RM. Three sets of ten repeats were performed in the first week, four sets of ten repeats in the second week, and from the third week, five sets of ten repeats with 70% of 1RM were performed for both the squat and lunge. All the sets and exercises were separated by 90-second rest intervals (3, 17).
3.4. Hypoxia Exposure
The subjects were placed in a sitting position breathing for twenty minutes using a mask attached to a Douglass Bag (Australian, model: Model ERA II GO2 Altitude) and filled with 14% oxygen. A pulse oximeter (Nonin Medical INC.Plymouth MN USA) was used to monitor arterial blood saturation in each subject from the beginning to the end of the intervention. The minimum arterial blood saturation was found to be 75% for continuous exercise or hypoxia exposure. In case the oxygen saturation dropped below this threshold during the intervention, or the subjects suffered breathing difficulties and dizziness, they were prevented from continuing the task.
3.5. Hypoxic Resistance Training
This type of training was performed in a similar fashion as resistance training in normoxic conditions. The subjects put on the mask after warm-up in a completely similar manner to the hypoxia exposure, and performed the resistance training protocol.
3.6. Sampling
Seven ml of fasting blood samples were collected between 8 am and 10 am one day before and two days after the intervention. VEGF levels were measured using ELIZA kits (Boster Biological, sensitivity of 1 pg/Ml >, made in USA), HDL, TG and TC using Pars kits, and LDL using the Friedwold formula.
3.7. Statistical Analyses
To investigate the research hypotheses, the dependent t-test was used for normally-distributed data and Wilcoxon, Kruskal-Wallis and Mann-Whitney U tests for the data with a non-normal distribution. The data collected were analyzed in SPSS-22.
4. Results
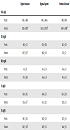
The present study participants comprised overweight male subjects with a mean body mass (weight) of 85.2 ± 6.53 kg, a mean age of 19.8 ± 1.13 years and a BMI of 27.4 ± 1.57 kg/m2. Table 1 presents the pre-test and post-test results obtained in each of the three groups, suggesting a significant increase in VEGF in all the groups, and showing a significant increase in HDL and a significant decrease in LDL, TC and TG only in the hypoxic resistance group.
| Hypoxic Resistance | Hypoxia Exposure | Normoxic Resistance | |
|---|---|---|---|
| VEGF, mg/L | |||
| Pre-test | 958.1 ± 499.1 | 1149.1 ± 609.6 | 1198 ± 907.6 |
| Post-test | 1620 ± 893.8b | 1655.5 ± 793.58b | 1438.4 ± 1008b |
| LDL, mg/dL | |||
| Pre-test | 94.8 ± 11.3 | 95.8 ± 10.9 | 96.2 ± 11.9 |
| Post-test | 89.7 ± 10.7c | 94.8 ± 9.9 | 95.1 ± 12 |
| HDL, mg/dL | |||
| Pre-test | 44 ± 3.7 | 46.1 ± 3.8 | 43.6 ± 4.1 |
| Post-test | 47.3 ± 3.88 | 46.6 ± 3.8 | 44.3 ± 4.2 |
| TC, mg/dL | |||
| Pre-test | 163.4 ± 10.3 | 164.4 ± 11.7 | 163.4 ± 10.5 |
| Post-test | 155.6 ± 10c | 163 ± 12.2 | 162.7 ± 11.1 |
| TG, mg/dL | |||
| Pre-test | 148.1 ± 10.3 | 148.2 ± 12.7 | 147.2 ± 11.5 |
| Post-test | 140.3 ± 12.8c | 147.8 ± 12.1 | 146.6 ± 11.1 |
The Pre-Test and Post-Test Results Associated with VEGF, HDL, LDL, TG and TC in All the Groupsa
The increase in the level of VEGF was found to be 75.8% (z = -2.803b, P = 0.005) in hypoxic resistance training, 51.6% (z = -2.701b, P = 0.007) in hypoxia exposure and 25.2% (z = -2.803b, P = 0.005) in normoxic resistance training. The Kruskal-Wallis test showed a significant difference (x2(2) = 6.382, P = 0.041) between the groups. The Mann-Whitney U test used for the pairwise comparison of the groups suggested no significant differences between the hypoxic resistance and hypoxia exposure groups (P = 0.631) and between the hypoxia exposure and hypoxia exposure groups (P = 0.075), while showing significant differences between the hypoxic resistance and the normoxic resistance groups (P = 0.015).
A significant increase of 7.4% (t9 = -4.9, P = 0.001) was observed in the level of HDL in the hypoxic resistance training group, although no significant changes were observed in the hypoxia exposure (t9 = -1.2, P = 0.256) and the normoxic resistance training group (t9 = -1.3, P = 0.222). A significant decrease of -5.3% (t9 = 3.1, P = 0.012) was observed in the level of LDL in the hypoxic resistance training group, although no significant changes were observed in the hypoxia exposure (t9 = 0.889, P = 0.397) and the normoxic resistance group (t9 = 1. 62, P = 0.139). A significant decrease of -5.2% (t9 = 3.1, P = 0.11) was observed in the level of TG in the hypoxic resistance training group, although no significant changes were observed in the hypoxia exposure (t9 = 0.324, P = 0.753) and the normoxic resistance group (t9 = 0.589, P = 0.570). A significant decrease of -4.6% (t9 = 4.1, P = 0.002) was observed in the level of TC in the hypoxic resistance training group, although no significant changes were observed in the hypoxia exposure (t9 = 1.3, P = 0.220) and the normoxic resistance group (t9 = 0.327, P = 0.751).
5. Discussion
The present study was conducted to investigate the effects of eight weeks of hypoxic and normoxic resistance exercises and hypoxia exposure on arterial factors in overweight men. After eight weeks, the level of VEGF increased in all the three groups, and significant differences were observed between the groups in terms of changes in the level of VEGF. The present findings suggested an increase in the level of VEGF following normoxic and hypoxic resistance trainings, which is consistent with literature (3, 12, 18). Kon et al. reported significant changes in the level of VEGF in hypoxic resistance training compared to in normoxic resistance training. They used an increasing intensity of exercise during the sessions, whereas the present study used a constant exercise intensity. The present study found the hypoxic resistance training group to be significantly different from the normoxic resistance training group, although it was found not to be significantly different from the hypoxia exposure group. Hypoxia can be concluded to affect the arterial function in overweight individuals (3). In contrast to the present study, no significant changes were observed in the level of VEGF in certain studies (13, 19, 20). Exercise duration and intensity have been proposed as the factors affecting the results (20). Research suggests that resistance training stimulates the secretion of cytokines (21), as a reason for increasing VEGF following resistance training. Moreover, exercise-induced ischemic induces a local hypoxia in muscles (18). Shear stress, cytokine secretion and local hypoxia can therefore significantly contribute to stimulating VEGF after resistance training. Hypoxia is a major factor contributing to angiogenesis stimulation (4). Systemic hypoxia such as angiogenesis can be considered an internal stimulus for endurance adaptation (22). A major function of hypoxia is to stimulate hypoxia-inducible factor-1 (HIF-1), which is responsible for transcribing different hypoxia-compatible genes, including angiogensis and glycolysis. Stimulating the expression of VEGF and erythropoietin (EPO) is an important regulatory effect of HIF-1 (23). Evidence suggests increased cytokines in hypoxia conditions, which can stimulate the expression of VEGF, as in the case of resistance training (24).
The present study showed a significant increase in HDL and significant reductions in LDL, TG and TC in the hypoxic resistance group, although it did not suggest any changes in lipid profile in the hypoxia exposure and normoxic resistance training groups. Both significant improvements and no changes in lipid profile have been reported in literature (14, 15). Evidence shows that the intensity, duration and volume of exercise affect the changes in lipid profile. Moreover, a minimum duration of eight weeks has been proposed for exercise to affect lipid profile, whereas the majority of researchers using protocols based on below eight weeks of training did not report significant changes (15). Compared to previous studies on resistance training protocols, the present research focused only on two types of training, i.e. lunge and squat. The low volume of exercise can explain the lack of changes in lipid profile obtained in the normoxic resistance exercise group. Investigating the effect of hypoxia exposure on lipid profile in patients with coronary heart disease showed that intermittent hypoxia significantly improves lipid profile after 22 sessions (3 hours per day) (25), which is inconsistent with the present study that reported no significant changes, as the subjects were exposed to hypoxia for only 20 minutes each session. Evidence suggests the critical role of HIF-1 in regulating the metabolism of carbohydrates and fats. In addition, using fat as a substrate required for metabolism has been observed in hypoxia conditions (26).
5.1. Conclusions
Normoxic and hypoxic resistance training and hypoxia exposure generally increased the level of VEGF. Hypoxic resistance training also significantly increased lipid profile. Hypoxia can therefore be proposed as a more prominent factor in terms of improving the arterial function. Exercises under hypoxia conditions and their effects on the arterial function have rarely been addressed in literature. Numerous discrepancies observed in the obtained results can be explained by the differences in the intensity and duration of trainings or the type of exercise. Overweight subjects at risk for cardiovascular diseases can generally prevent the disease by employing appropriate training protocols. Optimal training programs are therefore recommended to be provided for these individuals.
