



1. Background
Coronavirus disease 2019 (COVID-19), originated from China, was rapidly dispersed among other countries, worldwide, contaminating millions of people (1). Consequently, on January 31, 2020, World Health Organization (WHO) declared the virus to be a public health emergency of international concern (2). Within a short period, on February 21, 2020, some cases of COVID-19 were reported in Iran and later became one of the countries with the highest prevalence of the virus (3), so that some provinces such as Qom and Golestan reached > 50% exposure to COVID-19 (4).
According to the reports, severe acute respiratory syndrome, fever, and fatigue are the most common symptoms of the COVID-19 (5). Due to cough; one of the common symptoms of COVID-19, or respiratory droplet transmission, contact with a person carrying the virus, or with contaminated surfaces (2) causes stress and fear among the public which are considered as the secondary outcomes of this disease (6, 7). The fast transmission and fatality of COVID-19 have led to the development of new mental health problems among healthcare workers (8). Consequently, anxiety and depression are the most common psychological problems of nurses (6).
Health professionals, especially nurses as one of the largest groups of direct-care teams working in hospitals and dealing with this disease (9), may experience more anxiety and fear of getting this infectious disease and spreading the virus to their families, friends, or colleagues (6). Additionally, the high mortality rate of COVID-19 patients can lead to unpredictable and negative consequences for nurses such as death anxiety (10), which is a multidimensional construct with emotional, cognitive, and experiential attributes (11). Based on the evidence, death anxiety increases depression (10). Accordingly, the high mortality of COVID-19 patients may increase depression in nurses (12). Moudi et al. (13) reported that anxiety and depression may reduce nurses’ job performance and their motivation over time. Moreover, the care of dying patients causes grief, perceptions of failure, and increased levels of anxiety (14). In another study, Hu et al. reported that about half of the nurses participating in the study experienced mental health challenges such as burnout, fear, anxiety, and depression (15).
Given the possible negative psychosocial impact of the COVID-19 epidemic on the medical staff, and the likely increased rate of psychological problems among healthcare workers (16), it is necessary to identify factors leading to these problems among nurses in order to plan appropriate intervention programs.
2. Objectives
The study aimed at investigating the demographic factors related to depression and death anxiety among nurses caring for COVID-19 patients.
3. Methods
3.1. Study Design
This cross-sectional study was conducted among nurses at Kosar Hospital, from June to October 2020. The Kosar hospital is a 272-bed hospital, located in the east of Iran, with nearly 563 staff members. It includes a full range of general and interventional departments as well as two special wards for hospitalized COVID-19 patients. Approximately, 90 nurses work in these two wards and care for patients.
89 nurses were selected via a census method. The inclusion criteria were working in the hospital, having a Bachelor of Science or higher academic degree, at least a one-month experience of caring for COVID-19 patients, and no history of anxiety and depression. The nurses not willing to participate in this study and those who had recently lost a first-degree relative were excluded from the study
3.2. Data Collection
A demographic questioner, Beck’s depression inventory (2nd edition), and Templer Death Anxiety scale were used for collecting data.
3.2.1. Demographic Questioner
This researcher-made questionnaire yielded demographic data on age, gender, marital status, educational level, number of children, work experience, employment status, duration of caring for COVID-19 patients (in months), infection of family members with COVID-19, living alone or with family members, presence of a specific underlying disease in a nurse or their parents, spouse, or their children. The questionnaire consisted of 9 questions.
3.2.2. Beck’s Depression Inventory
Beck’s Depression inventory, second edition (BDI-II) consisted of 21 questions on a 4-point scale and three parts assessing somatic, cognitive, and affective symptoms. The questionnaire measures the severity of depression symptomatology: no depression (0 - 13), low (14 - 19), moderate (20 - 28), and severe depression (29 - 63). Higher scores on the scale indicate more severe depression (17). The reliability of this questionnaire was assessed using Cronbach’s alpha coefficient, which was reported to be 0.82.
3.2.3. Death Anxiety Scale
Templer Death Anxiety scale (DAS), was designed in 1970 by Templer. It is a self-report questionnaire consisting of 15 true-false items, scored on a 15- point scale, from 0 to 15, and is classified into three levels: low (0 - 6), moderate (7 - 9), and severe (10 - 15) (10, 13, 18). The reliability and validity of the Persian version of Templer DAS are assessed using test-retest method, and their internal consistency is reported to be (total alpha) 0.91 and 0.89, respectively (19).
3.3. Ethical Considerations
The study proposal was approved by the Ethics Committee of Semnan University of Medical Sciences (code: IR.SEMUMS.REC.1399.060). All participants were informed about the voluntary nature of participation and they were assured that their information will be confidential. Moreover, they were informed that they could withdraw from this study at any time. Verbal and written informed consent was obtained from each participant and then data collection questionnaires were completed.
3.4. Statistical Analysis
Data were analyzed using SPSS Version 20 (SPSS Inc., IL, U.S.A.). Descriptive statistics consisting of mean, standard deviation, and percentage were used to describe the variables. The Pearson correlation was used to assess the correlation between death anxiety and depression. Also, inferential statistics including the Kruskal-Wallis and Mann-Whitney U test were used to investigate the relationship of death anxiety and depression to the demographic variables. A P-value of less than 0.05 was considered statistically significant.
4. Results
4.1. Patient Characteristics
Among 89 nurses participating in this study, 79.8% were female, 92.1% were undergraduates, and 84.3% were married. The mean age of the nurses was 32.80 ± 6.90 years, and 37.2% of them had no children. Also, the mean duration of working in the care wards of patients with COVID-19 was 3.10 ± 1.64 months. More details on demographic variables are presented in Table 1.
| Variables | No. (%) |
|---|---|
| Gender | |
| Male | 18 (20.2) |
| Female | 71 (79.8) |
| Educational level | |
| BSc | 82 (92.1) |
| MSc | 7 (7.9) |
| Employment status | |
| Official hiring | 33 (37.1) |
| Contract work | 10 (11.2) |
| Others | 46 (51.7) |
| Marital status | |
| Married | 75 (84.3) |
| Single | 14 (15.7) |
| Living alone or with family | |
| Alone | 11 (78.6) |
| With family | 3 (21.4) |
| Underlying disease in nurse | |
| Yes | 8 (9) |
| No | 81 (91) |
| Infection of family members with COVID-19 | |
| Yes | 7 (7.9) |
| No | 82 (92.1) |
| Underlying disease in nurse’s parents | |
| Yes | 20 (22.5) |
| No | 69 (77.5) |
| Number of children | |
| No child | 28 (37.3) |
| 1 | 23 (30.7) |
| 2 - 3 | 24 (32) |
| Underlying disease in nurse’s child | |
| Yes | 2 (4.3) |
| No | 45 (95.7) |
| Underlying disease in nurse’s spouse | |
| Yes | 2 (4.3) |
| No | 45 (95.7) |
| Age, y | |
| ≤ 31 | 39 (43.8) |
| > 31 | 50 (56.2) |
| Work experience, mo | |
| ≤ 9 | 55 (61.8) |
| > 9 | 34 (38.2) |
| Duration of work with COVID-19 patients, mo | |
| ≤ 3 | 56 (62.9) |
| > 3 | 33 (37.1) |
Demographical Characteristics of Nurses
4.2. Outcomes
The mean score of death anxiety among nurses was 7.32 ± 1.75. Additionally, the mean score of depression among them was 10.82 ± 8.50. 9% of nurses suffered from severe death anxiety and 5.6% from severe depression (Table 2).
The results of the Pearson’s correlation-coefficient showed a significant positive correlation between death anxiety and depression (r = 0.322, P = 0.05). Also, there was a significant positive correlation between death anxiety, nurses’ age, and length of working experience (P < 0.05) (Table 3).
Correlation Between the Death Anxiety and Depression with Quantitative Variables in Nurses
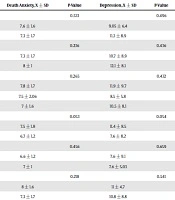
The results of the Mann-Whitney U-test showed no statistically significant relationship between the mean scores of death anxiety and depression to gender, educational level, marital status, an underlying disease in nurses or their parents, and special disease in their spouses or children (P > 0.05, Table 4). Also, the Kruskal-Wallis test results revealed no significant relationship between the mean scores of death anxiety and depression to their employment status and the number of children (P > 0.05, Table 4).
| Variables | Death Anxiety | Depression | ||
|---|---|---|---|---|
| Mean ± SD | P-Value | Mean ± SD | P-Value | |
| Gender | 0.533 | 0.496 | ||
| Male | 7.6 ± 1.6 | 9.05 ± 6.4 | ||
| Female | 7.3 ± 1.7 | 11.3 ± 8.9 | ||
| Educational level | 0.236 | 0.436 | ||
| BSc | 7.3 ± 1.7 | 10.7 ± 8.9 | ||
| MSc | 8 ± 1 | 12.1 ± 8.1 | ||
| Employment status | 0.265 | 0.432 | ||
| Official hiring | 7.8 ± 1.7 | 11.9 ± 9.7 | ||
| Contract work | 7.5 ± 2.06 | 8.5 ± 5.8 | ||
| Others | 7 ± 1.6 | 10.5 ± 8.1 | ||
| Marital status | 0.053 | 0.054 | ||
| Married | 7.5 ± 1.8 | 11.4 ± 8.5 | ||
| Single | 6.7 ± 1.2 | 7.6 ± 8.2 | ||
| Living alone or with family | 0.456 | 0.659 | ||
| Alone | 6.6 ± 1.2 | 7.6 ± 9.1 | ||
| With family | 7 ± 1 | 7.6 ± 5.03 | ||
| Specific underlying disease in nurse | 0.218 | 0.541 | ||
| Yes | 8 ± 1.6 | 11 ± 4.7 | ||
| No | 7.3 ± 1.7 | 10.8 ± 8.8 | ||
| Infection of family members with COVID-19 | 0.938 | 0.292 | ||
| Yes | 7.4 ± 1.2 | 13.8 ± 8.4 | ||
| No | 7.3 ± 1.7 | 10.5 ± 8.5 | ||
| Underlying disease in nurse’s parents | 0.938 | 0.292 | ||
| Yes | 7.4 ± 1.2 | 13.8 ± 8.4 | ||
| No | 7.3 ± 1.7 | 11.1 ± 8.2 | ||
| Number of children | 0.969 | 0.987 | ||
| No child | 7.5 ± 1.8 | 11.2 ± 8.3 | ||
| 1 | 7.4 ± 1.7 | 11.6 ± 8.9 | ||
| 2 - 3 | 7.5 ± 1.9 | 11.5 ± 8.5 | ||
| Underlying disease in nurse’s child | 0.368 | 0.051 | ||
| Yes | 8.3 ± 0.57 | 20 ± 4.3 | ||
| No | 7.4 ± 1.8 | 11.09 ± 8.4 | ||
| Underlying disease in nurse’s spouse | 0.354 | 0.937 | ||
| Yes | 8.7 ± 2.3 | 10.7 ± 6.9 | ||
| No | 7.4 ± 1.7 | 11.4 ± 8.6 | ||
Comparison of Average Score Between Death Anxiety and Depression Based on Demographical Characteristics of the Nursesa
5. Discussion
Pandemic or epidemic diseases put healthcare workers, especially nurses, in a psychological dilemma (20). The study focused on the degree of death anxiety and depression among nurses and examined the relationships between predictive factors of death anxiety and depression among Iranian nurses caring for COVID-19 patients.
The findings of the present study showed no statistically significant differences in the mean scores of death anxiety and depression with gender. However, some studies have revealed that gender may affect psychological health status (21). Moreover, gender-related attributes may increase the impact of the COVID-19 pandemic on women (22). Some researchers have observed the significant effect of depression on female nurses caring for COVID-19 patients (23, 24).
Our findings do not support the relationship between death anxiety and depression to the underlying diseases in nurses. This result contradicts the results of the studies (23) showing a significant correlation between depression and chronic diseases in nurses caring for COVID-19 patients (23). These contradictory results may be attributed to the small number of nurses with chronic disease (9%) in our study.
The findings also revealed that in most nurses, death anxiety was at a moderate level. However, no studies reported the prevalence of death anxiety in nurses caring for COVID-19 patients. Galehdar et al. (25) showed that nurses experienced anxiety due to COVID-19 patients’ death. Peters et al. (26) reported that most caregivers experienced high levels of anxiety following the death of their patients. Death anxiety can lead nurses to develop negative attitudes towards caring for the patients which may lead them to apply defense mechanisms by distancing themselves from perceived death or practicing death avoidance behaviors (27). Pehlivan et al. (27) suggested that probable psychological interventions are provided for nurses to overcome death anxiety.
Our study revealed that death anxiety was higher among older nurses than the other groups. The result was in line with the results of the study conducted by Li et al. (9), who reported that older nurses caring for COVID-19 patients had higher levels of anxiety in some hospitals in Wuhan, China. Another study (28) reached the same conclusion, revealing that death anxiety increases with age. In contrast to these findings, Peters et al. (26) reported that younger nurses consistently showed more death anxiety.
We also found that nurses having longer work experience had higher levels of death anxiety. Black (29) reported that older caregivers, with more experience of working with elderly patients, showed higher levels of death anxiety and death avoidance attitudes than younger caregivers. However, some studies have reported contradictory results. For instance, Halliday and Boughton (30) reported that palliative care nurses with more experiences of caring for dying patients showed a lower level of death anxiety, and Lange et al. (31) found that more work experience leads nurses to develop more positive attitudes towards death and better care for dying patients.
According to our results, about 47% of the nurses experienced some levels of depression, which was higher than the previously reported results. For instance, a meta-analysis by Pappa et al. (32) showed a 22.8% prevalence of depression among healthcare workers caring for COVID-19 patients. The percentage discrepancy may be due to the differences in research communities.
In this study, there were significant positive relationships between death anxiety and depression. This finding is in line with the results of a review article conducted by Vanjare and Chandra (20) who demonstrated that the death of COVID-19 patients can induce depression among healthcare workers. Sharifi Saki et al. (10) also identified that death anxiety increases depression in women suffering from breast cancer. Other researchers as well have shown a relationship between death anxiety and depression in patients, nurses, and caregivers (33, 34).
It has been reported that the psychological wellbeing of nurses plays a significant role in nursing care and prevention of the spread of disease in patients during pandemics such as COVID-19 (35). Accordingly, special attention to nurses and psychological support is felt strongly for promoting the care provided to patients (36).
As a strong point, this was the first study that investigated demographic factors associated with depression and death anxiety in nurses caring for COVID-19 patients, however, there were several limitations to this study. One limitation of the present study was the lack of similar research to compare our results with. Furthermore, the small sample size of nurses with the majority of female nurses (79.8%) rather than male nurses restricted the generalization of the results beyond this specific sample. Thus, more studies should be conducted in different settings with a larger sample size and an equal representation of gender to facilitate the generalization of findings.
5.1. Conclusions
The finding of the present study revealed that nurses caring for COVID-19 patients are at high risk of death anxiety and depression. Thus, there is a need to identify these problems, so that they could be prevented or reduced using possible solutions and effective interventions such as online psychological counseling services and multidisciplinary mental health teams to support and facilitate appropriate coping mechanisms for frontline nurses caring for COVID-19 patients.
