



1. Background
Although severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic has seriously affected the whole world, South Korea successfully managed to limit the SARS-CoV-2 spread via various strategies. There was no report of full lockdown during the viral spread in the country. People vigilantly responded to the viral epidemics, and based upon experience of previous Middle East respiratory syndrome coronavirus (MERS-CoV) epidemics in South Korea, medical professionals, students, and political leaders actively participated to combat coronavirus disease 2019 (COVID-19). South Koreans used latest technology and digital approaches to introduce smart trace mechanism against COVID-19 patients to tackle the situation tactically. However, there is a need to identify the level of awareness among general populations of South Korea. The current study aimed to evaluate awareness, knowledge, and epidemic prevention abilities among South Koreans between Dec 2019 and Aug 2020.
2. Methods
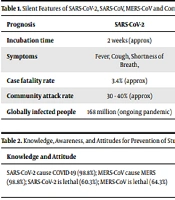
Viral pathogens are increasing worldwide, and it is anticipated that soon viruses would emerge as highly dangerous entities (1). Prevention is better than cure. Identification of epidemiological patterns of viral spread and dissemination of knowledge and awareness related to risk factors associated with viral transmission in different populations at risk could prevent the emergence of epidemics (2, 3). The SARS-CoV-2 emerged as an epidemic in Asia and became pandemic in early 2020 causing serious public health concern internationally. The MERS-CoV, member of the beta group of coronaviruses, is significantly distinct from SARS coronavirus and common cold coronavirus (4). Some salient features of SARS-CoV-2, SARS-CoV, MERS-CoV, and common cold are shown in Table 1.
The primary source of MERS infecting humans is camels, while bats are considered ultimate reservoir (5). The global number of SARS-CoV-2 positive cases on 31st May 2021was 184 million, and the number is still climbing vigorously. Also, the number of deaths due to COVID-19 was 3.98 million, and the worst affected countries were the United States of America and India (6-8). In 2012, the MERS was initially reported from Kingdom of Saudi Arabia, but later the viral infection was reported from more the 21 different countries, which depicted huge viral spread. During 2014 and 2015, the MERS epidemic in Saudi Arabia infected 688 with 282 deaths, while in South Korea, it infected 186 with 36 deaths. SARS-CoV-2 and MERS have become a major threat to the global health.
| Prognosis | SARS-CoV-2 | SARS-CoV | MERS-CoV | Common Cold |
|---|---|---|---|---|
| Incubation time | 2 weeks (approx) | 1 week (approx) | 1 week (approx) | 1 - 4 days (approx) |
| Symptoms | Fever, Cough, Shortness of Breath, | Fever, chills, muscle aches, headache | Cough Shortness of Breath | Cough, Sneezing, Runny or Stuffy Nose |
| Case fatality rate | 3.4% (approx) | 9.6 - 11% (approx) | 34.4% (approx) | 0.1% (approx) |
| Community attack rate | 30 - 40% (approx) | 10 - 60% (approx) | 4 - 13% (approx) | 10 - 20% (approx) |
| Globally infected people | 168 million (ongoing pandemic) | 8098 (in 2003) | 2500 | 1 billion (approx) |
The prevalence of viral infections is unfortunately increasing day by day due to the limited awareness among general population (9-12). Poor diagnostic abilities and inadequate knowledge about viral transmission via fomites limit accurate acquisition of prevalence rates (13, 14). Similarly, overcoming COVID-19 vaccine hesitancy and determining adequate antibody levels against SARS-CoV-2 spike protein is a challenging task (15, 16). Although the time of MERS-CoV and SARS-CoV-2 outbreak was different, based upon the experiences of emergency preparedness centers, paramedical staff, and government officials, the surge of COVID-19 in South Korea was effectively tackled within short period of time. Therefore, we asked whether the previous knowledge, awareness, and attitude of general population of South Korea about MERS-CoV contributed to emergency preparedness and development of smart information technologies against SARS-CoV-2 spread. Accordingly, the aim of the study was to assess the knowledge about SARS-CoV-2 and MERS-CoV awareness and prevention in general population of South Korea.
A cross-sectional survey was conducted in multiple cities of South Korea, including Jeonju, Suwon, and Seoul, with a sample size of 1500 from December 2019 to August 2020. Also, 71.4% of the participants were female, 57.1% had a university degree, 21.4% either enrolled or completed their postgraduate studies, and 21.5% were high school graduates. Majority of the participants (40%) were > 40 years of age, 32% were between 20 - 40 years of age, while 28% were below 20 years of age. Moreover, 98.8% of the participants were aware of COVID-19 causing virus SARS-CoV-2, while 64.3% of participants were aware of MERS and associated deaths. According to our results, 99.5% of participants responded that SARS-CoV-2 can be prevented by maintaining safe distance of about two meters, while 78.6% of participants knew that MERS-CoV can be transmitted by air. In addition, 99.5% of participants were aware that SARS-CoV-2 can be transmitted through close contact and droplets, while 21.4% of participants thought that MERS-CoV can be transmitted by close contact. Furthermore, 85% and 13.6% of participants considered that SARS-CoV-2 and MERS-CoV are preventable using vaccines, respectively (Table 2). It should also be mentioned that 97% of the participants used masks for prevention of airborne diseases.
| Knowledge and Attitude | Mode of Transmission SARS-CoV-2/MERS-CoV | Preventable by Vaccine |
|---|---|---|
| SARS-CoV-2 cause COVID-19 (98.8%); MERS-CoV cause MERS (98.8%); SARS-CoV-2 is lethal (60.3%); MERS-CoV is lethal (64.3%) | Airborne (78.6%); Droplets (99.5%); Close contact (99.5%/21.4%); Human to human (71.4%); Human to animals (14.3%); Feces (7.1%) | SARS-CoV-2 (85%); MERS-CoV (13.6%) |
3. Results
In this study, 65.3% of the participants reused the same mask for several days, 99% responded that strictly using masks can prevent SARS-CoV-2 spread, and 31.84% were aware of the fact that the MERS-CoV spread can be prevented by using mask in crowded areas and by maintaining good personal hygiene through washing hands frequently. Moreover, 81% of the participants believed that bats are the source of SARS-CoV-2 while 71.4% responded that the source of MERS-CoV spread was camels (Table 3). Also, 93% and 71.4% of participants thought that SARS-CoV-2 and MERS-CoV can be transmitted through human-to-human route, respectively. In addition, 14.3% of participants considered that SARS-CoV-2 and MERS-CoV can be transmitted from humans to animals, and 7.1% considered that SARS-CoV-2 or MERS-CoV can be transmitted by feces (Table 2). Data analysis revealed that 21.4% of the participants were highly satisfied with the support provided by Korean government to combat SARS-CoV-2 and MERS outbreak (Table 3), 28.6% were satisfied up to some extent, while 35.7% were not satisfied with the efforts made by government.
| Utilization of SOPs | Source of Virus | Efforts by Government |
|---|---|---|
| Usage of Masks (97%); Re-usage of Masks (65.3%); Masks usage is critical for SARS-CoV-2 (99%); Masks usage is critical for; MERS-CoV (31.84%) | Bats source of SARS-CoV-2 (81%); Camels source of MERS-CoV (71.4%) | Highly satisfied (21.4%); Satisfied to some extent (28.6%); Not satisfied (35.7%) |
4. Conclusions
Efforts are still needed to improve knowledge and awareness level about prevention of viral diseases among general population in South Korea. Policy makers should not only provide wider opportunities for the dissemination of knowledge and awareness about viral transmission, but also focus on epidemiological patterns of emerging epidemics in world. In educational institutes and offices, disseminating online awareness programs and conducting online seminars related to biosafety and virus control could be a better strategy to prevent future viral epidemics.
