1. Context
Since prehistoric times, human beings have used medicinal plants to treat and find the cure for various diseases caused by bacteria, viruses, fungi, and other microbial agents (1). With the outbreak of the COVID-19 virus in Wuhan (China) and its spread to other countries that resulted in a pandemic, the lack of standard protocol for effective treatment by modern medicine experts has resulted in attention to exploring medicinal plants for possible treatment (2). Another reason for the shift of attention toward the possible use of medicinal herbs, especially in developing countries, is the expensive cost of modern antiviral and other drugs used to treat COVID-19 (3). As herbal medicines are used worldwide, with the outbreak of COVID-19, experts of traditional medicines in different parts of the world have started using medicinal herbs to treat COVID-19. Several reports have been published claiming partially or completely successful treatment of COVID-19 by using popular medicinal plants that are edible worldwide such as turmeric, coneflower, licorice, ginger, common ivy, and onion (4-6). Due to being cheap and easily available, the use of medicinal plants may have increased for the treatment of COVID-19. However, their use has led to concerns about the lack of credible scientific evidence, toxicity, and ineffectiveness. Adequate quality control, unknown herb-drug interactions, and possible adulteration are other vital concerns in this regard. COVID-19 patients suffering from chronic disorders such as cardiovascular diseases, diabetes, psychiatric problems who take several medicines are especially considered susceptible to herb-drug interactions.
While the worldwide use of herbal medicines for the treatment of COVID-19 is gaining popularity, precautionary guidelines for their use are being published in medical journals (7-9), and public awareness in this regard has increased, many pivotal questions remain:
(1) Can herbal medicines alone really prevent, treat or cure COVID-19 infection?
(2) If natural medicinal formulations have positive effects on controlling COVID-19, are these effects limited to few popular plants such as ginger, turmeric, and onion?
(3) Can herbal medicines be used simultaneously with current COVID-19 treatment protocols?
(4) How serious are the interactions between herbal medicines and the currently available drugs used to treat COVID-19?
(5) For patients suffering from chronic diseases, how are dose adjustments made for the current drugs they are taking for COVID-19 if they also use herbal medicines?
These questions and probably many other such questions remain to be answered apparently because of a lack of collaboration and communication between the experts of modern medicine and traditional medicine worldwide. While both sides have their claims of advantages over the other side, the ground reality is that based on the popularity of herbal medicine worldwide, it can be reasonably argued that their use is also common for the treatment of COVID-19, while data about their beneficial or adverse effects are not available. On the other hand, no effective modern medicine-based treatment protocol currently exists that is accepted by experts worldwide. In this review article, we present the pros and cons, safety, and precautions of using herbal medicines for the treatment of COVID-19 in an attempt to reconcile and minimize the difference of opinion between traditional and modern medicine.
2. Methods
English articles published in recent scientific literature, especially since the start of the COVID-19 pandemic at the end of 2019, about herbal medicines, traditional medicines, and natural products and their activity against viral diseases, COVID-19, and respiratory problems were searched in Medline, Scopus, and Web of Science. Gathered articles' content was investigated accurately, and applicable data were extracted. In addition, literature published as critical reviews, commentaries, and articles mentioning concerns of modern medical experts on the safety, quality, and efficacy of herbal medicines for the treatment of COVID-19 were also searched, and relevant content was used for writing this review.
3. Approaches to the Promising Use of Herbal Medicines and Phytochemicals in COVID-19
In order to respond to the questions mentioned above regarding COVID-19 infection, we present two broad approaches that are also in agreement with the published views of experts:
The first approach is screening and developing antiviral compounds from herbal medicines currently used in traditional medicine to treat COVID-19. This can also result in a novel antiviral compound as a lead molecule. Several studies have previously reported antiviral activity in natural products, several antiviral compounds have been identified, and some of them or their related derivatives have progressed to the stage of clinical trials (10-12). However, there is currently no marketed antiviral compound originating from natural products.
In vitro and in silico antiviral activities in natural products against severe acute respiratory syndrome (SARS) and middle east respiratory syndrome (MERS) have been reported in several studies (13-15). Developing a new single compound drug to treat COVID-19 from these natural antiviral products would be an expensive and time-consuming approach. Especially in developing countries with the low income of the general population, the cost of the new drug will be expected to be unaffordable.
The second approach is the application of currently available herbal medicine formulations to treat symptoms of COVID-19 infection. Based on the physiopathology and clinical presentation of COVID-19, herbal medicines can be used for the treatment of symptoms related to different systems, including fever, cough, malaise, dyspnea, fatigue, sputum secretion, anorexia, sneeze, rhinitis, myalgia, goosebumps, sore throat, headache, diarrhea, chest pain, rhinorrhea, palpitation, dizziness, nausea or vomiting, shivering, confusion, nasal congestion, abdominal pain, and hemoptysis (16).
4. Suggested Categories of Medical Plants for Their Use in COVID-19
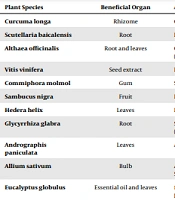
Concerning the signs and symptoms of COVID-19 disease, the following categories of herbal medicines (sections 4.1 - 4.7) are suggested to be used as a supportive treatment for the management of patients (17). It is worth mentioning that most of these medicinal plants and bioactive compounds have been reported to possess multiple activities mentioned below, either in vitro or in vivo.
4.1. Antipyretic Medicinal Plants
As fever is a common symptom of COVID-19 infected patients, antipyretic drugs are used for treatment. Medicinal herb Salix spp. bark is a source of salicin glycoside, which is metabolized by hydrolase enzymes to yield salicylic acid that inhibits cyclooxygenase 1 and 2 enzymes, leading to anti-inflammatory and anti-fever activities (18). Also, studies have confirmed similar activities of some other compounds and fractions such as black pepper (containing piperine, an alkaloid) (19), fenugreek (seeds chloroform fraction and aqueous extract of leaves) (20), mango (containing mangiferin, a phenolic compound) (21), and sweet wormwood (water fraction) (22).
The use of medicinal plants for their antipyretic activities in COVID-19 infection is justified based on the in vitro and in vivo scientific data about their antipyretic activities. However, the exact concentration of medicinal plants for their antipyretic activities remains to be determined.
4.2. Medicinal Plants with Antiviral Activity
Several plants used in traditional medicine have been reported to have antiviral activities at extract, fraction, or pure compound level (23). Particularly, few plants are reported to have antiviral activity against coronavirus species causing SARS and MERS (15). Most antiviral compounds are prevalent in dietary food items such as culinary species, vegetables, nuts, fruits, and popular medicinal plants and herbal medicines. Some examples are Apiaceae family members like parsley and celery (containing psoralen, a furanocoumarin) (24), Brassicaceae family members like broccoli, brussels sprouts, and black mustard seeds (containing sinigrin, a glucosinolate) (25), strawberries, apples, spinach, Aloe vera, carrots, mulberries and tea (containing an abundant amount of myricetin, a flavonol) (26), soybean and olive oil (containing β-sitosterol, a phytosterol) (27), citrus fruits juices (containing hesperetin, a flavanone) (28), and licorice (containing glycyrrhizin, a pentacyclic saponin) (29).
These data show the broad-spectrum antiviral activity of different plants, particularly those that are edible and common in diets worldwide. Also, some studies report the antiviral activity of plants mentioned above against previous outbreaks caused by other coronaviruses and even COVID-19. It can be concluded that the inclusion of these plants in diets can enhance general antiviral immunity and play a role in the prevention and treatment of COVID-19 infection.
4.3. Anti-inflammatory Medicinal Plants
COVID-19 is associated with cytokine storms leading to severe and generalized inflammatory reactions (30). Thus, using medicinal plants with in vivo or in vitro anti-inflammatory activity can benefit patients suffering from COVID-19 (31). Typical examples are turmeric (containing curcumin, a polyphenolic compound) (32), ginger (containing 6-gingerol, a phenolic compound) (33), rosemary (containing rosmarinic acid, a phenolic acid) (32), borage (containing gamma-linolenic acid, an omega-6 polyunsaturated fatty acid) (34), evening primrose (containing linoleic acid and gamma-linolenic acid, omega-6 polyunsaturated fatty acids) (35), dog rose (containing linoleic and linolenic acid, polyunsaturated fatty acids) (36), nettle (containing quercetin, a flavonol) (37), sage (containing a phenolic acid: rosmarinic acid and a triterpene: ursolic acid) (38), and olive (containing oleocanthal, a phenolic compound) (39). Anti-inflammatory effects of traditional medicines specifically relate to their flavonoids, terpenoids, and fixed oils content that are extensively distributed in other vegetables, nuts, beans, cereals, herbal beverages, and fruits.
Inflammation plays a pivotal role in the pathogenesis of COVID-19, causing cytokine storms and increasing mortality by the widespread occurrence of the inflammatory process. Consumption of medicinal plants with anti-inflammatory compounds with novel structures can help treat COVID-19 patients or at least decrease the number of severe cases.
4.4. Immuno-stimulating Medicinal Plants
COVID-19 infection is more common and severe in immunocompromised patients (40, 41). Thus, using medicinal plants with immuno-stimulating activities, such as coneflower (containing polysaccharides, alkamides; dodeca-2E,4E,8Z,10Z-tetraenoic acid isobutyl amide, and phenolics; cichoric acid) (42) that is a famous plant with reported immunostimulating and immunomodulating activity, can benefit such patients. Some of the marketed products of coneflower, such as Nature's Way Echinacea, Now Foods Echinacea, and Nature Made Echinacea, are commercially available. Other plants include Mongolian milkvetch (Astragalus membranaceus) (containing astragaloside IV, a triterpene saponin) (43), ginger (containing zingerone, a phenolic compound) (44), green tea (containing epigallocatechin-3-gallate, a polyphenolic compound) (45), Aloe vera (containing acemannan, a polysaccharide) (46), and ginseng (containing ginsenoside Rb1, a triterpene saponin) (47). However, the use of immunostimulant medicinal plants is contraindicated in patients suffering from autoimmune diseases or those taking immunosuppressive drugs.
In summary, plants with immuno-stimulating activities can increase the human body's resistance to pathogens and contribute to the prevention of infectious diseases. In addition, herbal products can also be used during COVID-19 to enhance immunity. However, their limitation for use in immunocompromised patients should be considered.
4.5. Antioxidant Medicinal Plants
COVID-19 infection is associated with extensive tissue damage requiring repair and recovery back to a normal functional state. Medicinal plants containing antioxidant compounds, such as flavonoids (eg, quercetin, kaempferol, apigenin, myricetin, luteolin, isorhamnetin, luteolin, chrysoeriol, hyperin, isoquercetin, rutin, hesperidin, naringenin, taxifolin, nobiletin, and hyperoside), anthocyanins (eg, cyaniding, malvidin, peonidin, delphinidin, pelargonidin, petunidin, and idaein), carotenes (eg, α-carotene, β-carotene, γ-carotene, and lycopene), and xanthophylls (eg, auroxanthin, antheraxanthin, neoxanthin, lutein, violaxanthin, zeaxanthin, and β-cryptoxanthin), can help in this process (48, 49). Commonly used edible plants like spinach, celery, parsley, apple, orange, red cabbage, blackberry, barberry, carrot, tomato, mango, and pumpkin have high antioxidant content. In addition to the above-mentioned antioxidant phytochemicals that give a specific color to plant parts, the antioxidant activity of chlorophylls as the most widespread natural pigment cannot be ignored (49). In every plant organ, a class of phytochemicals predominates others in making the plant a colorful appearance in which the main coloring agents are chlorophylls (green), flavonoids (yellow), anthocyanins (red to blue), and tetraterpenoids including carotenes and xanthophylls (yellow to red) with either conjugated double bonds or phenolic hydroxyls responsible for their free radical scavenging activity. Thus, all vegetables and fruits used in different world regions have some antioxidant activity.
According to the antioxidant potential of various phytochemicals and their widespread presence in medicinal plants, they can be used as supportive therapy to treat COVID-19. Free radical production plays a prominent role in the tissue damage caused by infectious diseases, especially when accompanied by inflammation. Thus, the antioxidant activity of medicinal plants can minimize tissue damage and promote faster recovery.
4.6. Medicinal Plants Used in Treating Respiratory Infections, Cough, and Flu
As respiratory infections are common worldwide, several medicinal plants in different traditional systems have been used for treatment. These herbal medicinal products include decongestants (eucalyptus oil, peppermint oil, and camphor) (50), bronchodilators (cocoa, coffee, tea, onion) (51, 52), demulcents and emollients (mallow, marshmallow, licorice, elder, pelargoniums) (29, 50), expectorants and mucolytics (thyme, common ivy, licorice, sage, senega, ipecac, poplar buds) (29, 50, 53, 54), anti-allergics (toothpick plant, chicory) (50, 55) and antitussives (licorice, black cumin, flax, common wormwood, cumin) (53, 54, 56).
Although COVID-19 infection involves different body systems, it is usually considered a respiratory disease and causes respiratory symptoms. The above-mentioned plants and their products can help reduce COVID-19 associated respiratory symptoms and facilitate the convalescence of patients.
4.7. Adaptogenic Medicinal Plants
Adaptogenic medicinal plants protect against stress and increase adaptability, resilience, and survival via enhancing non-specific resistance. These plants act by modulating innate and adaptive immunity, enhancing anti-inflammatory activity, neutralizing oxidative stress and repairing related damage, enhancing antiviral effects, and improving quality of life during convalescence (57). Commonly used adaptogenic plants include ginseng (containing ginsenoside Rb1, a triterpene saponin), licorice (containing glycyrrhizin, a pentacyclic saponin, liquiritin, and isoliquiritin flavonoid compounds), and ashwagandha (containing withaferin A, a steroidal lactone triterpene) (58) that can be considered in the treatment of COVID-19 infection.
Adaptogenic plants with various biological effects can increase body resistance against the COVID-19 virus, decrease the infection period, and increase the patient recovery rate. Generally, adaptogenic plants can help overcome the COVID-19 induced damage and promote recovery.
5. Concerns for the Use of Herbal Medicines in COVID-19
What is mentioned above illustrates the possible effects of natural compounds and herbal products on the treatment of COVID-19 infection. However, there are inherent issues related to the composition, preparation, and use of herbal medicines. In addition, the use of medicinal plants can lead to problems and adverse effects, mainly when used in patients with specific medical conditions (vide infra).
5.1. Quality
Several factors affect the concentration of bioactive compounds in medicinal plants, such as geographical conditions of the soil where the plant is harvested, plant species and plant parts used in treatment, harvesting time, storage condition, and processes that are routinely employed for preparation. Standardization and quality control are much more difficult and technically more time-consuming in herbal medicines than in single compound drugs. In this regard, the contamination of herbal products by heavy metals and microbes is a common problem. Medicinal plants used for sexual performance enhancement, bodybuilding, and weight loss have the highest adulteration rate (59). Considering the fear and stress caused by the COVID-19 pandemic leading to rapid demand for herbal products in a short duration of time, the quality control of herbal medicines may be further compromised.
5.2. Efficacy
Although many papers have reported positive effects of herbal medicines, due to the difficulties in quality control as mentioned above and the lack of comparison of their therapeutic effects with modern medicines, their actual efficacy remains unknown in most cases. This is true for most herbal medicines currently available on the market.
5.3. Safety
5.3.1. Adverse Effects
Contrary to popular belief, most herbal medicines have adverse effects that are also reported (60). Common examples include Ephedra preparations that cause hypertension, myocardial infarction and arrhythmia, seizure, stroke, hepatotoxicity, neurotoxicity, and transient blindness (61, 62). Another example is the risk of hepatotoxicity by pyrrolizidine alkaloids containing plants of Boraginaceae like Borago officinalis (63). Medicinal plants with mild side effects include garlic (insomnia, vomiting, heartburn, dizziness, diarrhea, tachycardia, nausea, bloating, flushing, headache, mild orthostatic hypotension, sweating, offensive body odor, and flatulence) (64), echinacea (rash, abdominal pain, angioedema, dyspnea, nausea, pruritus, rash, erythema, and urticaria) (65), St. John's wort (nausea, rash, fatigue, restlessness, and photosensitivity) (66), ginger (mild to moderate gastrointestinal side effects and sleepiness) (67), ginseng (headaches, alterations in blood pressure, diarrhea, skin irritations, and vaginal bleeding) (68), and Aloe spp. (skin irritation, hives, cramping, and diarrhea) (69). Thus, patients with COVID-19 may exacerbate their symptoms while taking some of the medicinal plants.
5.3.2. Herb-Drug Interaction
Pharmacodynamic and pharmacokinetic herbal drug interactions are common, especially in patients suffering from chronic diseases such as diabetes, hypertension, and psychiatric and neurologic disorders (70). Additionally, drugs with a narrower therapeutic index, such as anticonvulsants, anticoagulants and antiplatelets, antiarrhythmics, immunosuppressives, neuroleptics, and antidiabetics, and some antibiotics, such as vancomycin, have a higher probability of herb-drug interaction and life-threatening consequences. Common examples of herb-drug interactions include St John’s wort used as an antidepressant that has significant interactions with antiviral drugs, oral contraceptives, immunosuppressive and anti-cancer medicines leading to their reduced clinical effectiveness (71). Ginseng, used as adaptogenic, interacts with anticoagulants such as warfarin and potentiates hypoglycemic effects of antidiabetic drugs (72). Another example of herb-drug interaction is ginger that is used to treat COVID-19. It enhances the effect of anticoagulants, leading to bleeding and hypoglycemic attacks in diabetic patients taking sulfonylureas (62, 73).
5.3.3. Concerns for Particular Groups of Patients
In addition to the restricted number of clinical studies performed on herbal medicines in patients, most of such studies have been carried out on regular adult volunteers with common health conditions and patients suffering from specific conditions have been largely excluded because of ethical and scientific considerations. This has led to the lack of authentic data in specific groups, including infants and children who have not achieved maturation of physiological and metabolic pathways (74). Pregnant women are another group where the nonselective use of herbal medicines can endanger the mother and unborn baby's health by embryotoxicity, teratogenicity, and abortion (75). Furthermore, breastfeeding women's use of herbal medicines, such as, tea and other caffeine-rich materials, can affect milk production or transfer some phytochemicals to newborns (76). Additionally, elderly patients who usually use more medicines and have age-related pharmacokinetic and pharmacodynamic changes are at higher risk of adverse effects of herbal medicines, herb-drug interactions, and related consequences (77, 78). Patients undergoing a surgical operation within two weeks are another group who require more precaution (79) since herbal medicines can alter the coagulation system (ginger) (62), cardiovascular stability (Ephedra spp.) (61, 62), blood sugar control (ginger) (73), anesthesia (valerian) (80) and drug metabolism (St John’s wort) (73). All these groups of patients require special precautions compared to regular patients.
6. Randomized Clinical Trials
Several medicinal plants have undergone clinical trials for their various biological effects. These include onion, garlic, ginger, turmeric, licorice, and ginseng preparations. However, no randomized clinical trials have been reported for their effectiveness in COVID-19 treatment. Comprehensive guidelines for clinical trials on herbal medicine have long been published and are available (81). Recently, clinical trial protocols have been reported for curcumin and herbal extracts of Shunthi (Zingiber officinale, ginger), Vidanga (Embelia ribes), Yashtimadhu (Glycyrrhiza glabra, licorice), Haritaki (Terminalia chebula), Guduchi (Tinospora cordifolia), Shatavari (Asparagus racemosus), Amalaki (Emblica officinalis), and Pippali (Piper longum) (82, 83), and results are being awaited for their efficacy and safety.
7. Conclusions
Medicinal plants used in traditional medicine have a promising role in treating COVID-19. Several antiviral compounds with novel structures are found in these plants that can be considered for further research to develop new medicinal products or new lead compounds. In addition, several categories of herbal medicines can be used for reducing inflammation and tissue damage and managing associated signs and symptoms of COVID-19 patients. Herbs, including commonly used edible plants such as licorice, onion, peppermint, marshmallow, carrot, spinach, apple, orange, cabbage, barberry, tomato, and parsley, can increase the general resistance of the human body against infection and promote immunity to overcome the COVID-19 associated pathogenic process. Thus, the rational use of herbal medicines can help prevent COVID-19, decrease its severity and duration, promote tissue repair, and enhance general recovery when used alongside modern medicines. However, several areas, including the quality, safety, and efficacy of herbal medicines, their interaction with drugs, and their use in particular groups of patients, require attention. We suggest randomized clinical trials on herbal medicines before their safe and effective use in the treatment of COVID-19.