



1. Background
Population aging and global transition in age structure are usually accompanied by frailty, comorbidities, multiple long-term conditions (MLTC), increased expenditure on health, and social isolation. Polypharmacy or simultaneous use of multiple medicines is an inevitable outcome of comorbidities or chronic diseases (1).
The term polypharmacy means “multi-medication” and is often beneficial. Shifting inappropriate polypharmacy to appropriate polypharmacy requires considerations at any point of multi-medication to achieve therapeutic objectives with the least preventable adverse drug reactions (2). Several factors distinguish inappropriate polypharmacy from appropriate polypharmacy, and the number of medications prescribed to an elderly patient alone is insufficient to label the practice as inappropriate. In many cases, an elderly patient with comorbidities may require four or six medications to achieve therapeutic goals and prevent adverse events, which is considered appropriate polypharmacy. On the other hand, if the treatment fails, adverse events occur, or unplanned hospital admissions may happen due to the prescription of too many medications without proper consideration of indications, this can be labeled as inappropriate polypharmacy. Therefore, it is crucial for healthcare professionals to carefully assess patients’ needs and medication requirements individually to ensure appropriate polypharmacy and prevent adverse outcomes (3). Over the past decade, polypharmacy has become a critical health issue due to increased healthcare costs to patients and the health system, adverse drug events (ADE), unplanned and prolonged hospitalization, elderly functional decline, cognitive impairment, especially delirium and dementia, and falls (4, 5).
Some interventions considered triggers for managing polypharmacy include prescribing and risk assessment, medication review, dispensing and administration, communication and patient engagement, and medication reconciliation (2). Many countries have prioritized the polypharmacy management approach as a holistic, systematic approach that extends across social, technological, and procedural boundaries. Polypharmacy management is a medication safety challenge and a team-based, patient-centered care approach (6, 7).
In addition, innovative change management approaches have significant potential to optimize patients’ care and promote older adults’ quality of care. Orienting the formal and informal caregivers and patients toward rational and efficacious medicine use is possible by using multidisciplinary team care, innovative pharmaceutical formulations and interventions, and technology-based solutions (8).
The change management approach is developing strategies and tools to promote innovation policies that can solve pressing megatrends or grand challenges based on identifying transitional factors in a socio-technical context (7). Such a scope expansion has revolutionized the existing innovation systems towards a horizontal policy approach that clarifies the role of multi-actors, technology innovations, leadership and governance, finance, structure and infrastructures, mechanisms, regulations, and social engagement, among others, to solve complex systems’ problems in a set of interactions (9, 10).
2. Objectives
Consequently, considering the health system as a complex adaptive system, it is necessary to go beyond innovation system thinking toward socio-technical theory and socio-technical regimes thinking for tackling polypharmacy management in the elderly with comorbidities. This study aimed to analyze the technical aspect of polypharmacy management in the elderly with comorbidities through the socio-technical model for change management to help decision-makers develop prospective roadmaps of current affairs. Notably, due to the depth and breadth of the content, the results on the social dimension of polypharmacy management through this approach will be discussed in another article.
3. Methods
3.1. Study Design
This qualitative study used semi-structured individual interviews. The results are reported per the Consolidated Criteria for Reporting Qualitative Studies (COREQ) checklist (11) (see Supplementary File).
3.2. Interview Guide
Several geriatric pharmacy and health policy experts reviewed and validated the interview guide. To extract all factors in all domains of the health complex system, all factors in the World Health Organization (WHO) Health System Six Building Blocks (12) were investigated through Leavitt’s socio-technical model (13, 14) for change management. Therefore, the interview guide consisted of four parts based on the dimensions of the Leavitt model. The first part of Leavitt’s model, the “Structure” dimension, was interrelated to two blocks of the WHO framework (Leadership & Governance and Financing). This part consisted of eight questions. The second part, the “Technology” dimension, was interlinked with two blocks (Medicine & Technology and Information) and comprised six questions. In the third part, the “Actor” dimension was interconnected with the “Health workforce” of the WHO framework and comprised seven questions. The last part, “Task,” was taken equivalent to “Service delivery” and contained three questions (see Additional File 2). The face validity of the interview guide was reviewed during two preliminary individual interviews, resulting in minor changes in the order of the questions.
3.3. Sampling and Data Collection
The participants were chosen by theoretical sampling. Thirty-five semi-structured interviews were conducted with several key informants selected by maximum variation purposive sampling in 2022. The participants had to be licensed pharmacists practicing geriatric care, geriatricians informed about elderly medication safety and polypharmacy management, health policy experts, or health informatics experts specialized in both fields to meet the inclusion criteria. We recruited most respondents through the snowballing technique among experts experienced in studying, working, and researching the abovementioned fields.
We emailed invitation letters attached with the interview guide to our mailing list of interviewees. A detailed information sheet and a consent form were emailed to those who responded to the initial invitation. Face-to-face, phone, and videoconference interviews were arranged based on participants’ preferences. All interviews were conducted in Iran, and telephone or videoconference interviews were conducted on the Skype or Zoom application between February and May 2022. After obtaining consent from the participants, the interviews were audio-recorded. Sampling and data collection through interviews continued until theme saturation. Based on the confidentiality and anonymity in research ethics, the sociodemographic data of each participant were collected at the end of each interview.
3.4. Data Analysis
Audio recordings were anonymized and transcribed verbatim by one of the researchers. We analyzed the interview transcripts inductively using qualitative data analysis software MAXQDA10 based on the method presented by Schwandt et al. (15). Broad themes and categories were identified for generating initial codes. In the next step, sub-themes were categorized, and the framework analysis method was used to analyze the results. The data analysis process continued with the interviews simultaneously and iteratively. The entire research team had a consensus on the results.
4. Results
4.1. Sample Characteristics
Thirty-five interviewees participated in the study. The characteristics of the study participants are detailed in Table 1. The majority of the respondents had more than 10 years of work experience.
| Characteristics | Frequency (%) |
|---|---|
| Gender | |
| Female | 20 (57.14) |
| Male | 15 (42.85) |
| Field of expertise | |
| Geriatrics | 14 (40) |
| Pharmacists/pharmaceutical specialist | 10 (28.57) |
| Health policy | 7 (20) |
| Health informatics | 4 (11.42) |
| Years of work experience | |
| 1 - 5 years | 7 (20) |
| 5 - 10 years | 9 (25.71) |
| Above 10 years | 19 (54.28) |
Sociodemographic Characteristics of Participants (N = 35)
4.2. Thematic Analysis
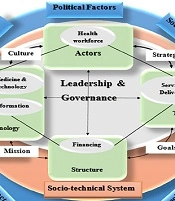
The healthcare system can fit the definition of a socio-technical system. As a complex adaptive system, interpreting the health system as a socio-technical system can promote the development of a new level of policy and practice. To ensure the elderly access to the rational use of medicines and manage polypharmacy among those with comorbidities, it is crucial to address the health system's technical and social aspects at any level (16). For this aim, our investigation was strictly based on the initial framework by Leavitt, who depicted every organization as a multivariate dynamic system with complicated interactions of four key variables: task, structure, technology, and actors (17). This model represents a holistic approach to implementing any systematic or organizational change in various fields, including social sciences and healthcare. We extended the Leavitt frame by combining it with six building blocks of WHO through a mixture of action research and retrospective analysis. As the cornerstone for models developed for studying socio-technical systems (STS), this approach promises to change the system layers by considering technological operations in parallel with social decision-making activities and community of stakeholders (18) (Figure 1)

Health system six building blocks through the lens of Leavitt’s socio-technical model
4.3. Technical Aspect Through Leavitt’s Model
4.3.1.“Structure”
Leavitt’s model’s “structure” dimension consists of two blocks of the WHO Framework (leadership and governance and financing). In this regard, two themes were extracted in leadership and governance: developing databases and optimizing homecare. The last theme emerging in the financing category was “pharmaceutical cost management.” Thirty-two (91.42%) interviewees considered “structure” the most critical transitional factor in polypharmacy management. These themes and subthemes are presented in Box 1.
| “Structure” in Leavitt’s Model |
|---|
| Leadership & governance (six building blocks) |
| Theme 1: Developing databases |
| Subthemes |
| - Developing electronic medical records (EMR) |
| - Expanding electronic databases for the documentation of pharmaceutical interventions, medication errors, mortality, and morbidity |
| Theme 2: Optimizing homecare |
| Subthemes |
| - Technology-enabled homecare |
Themes and Subthemes of the Structure Dimension (Leadership and Governance)
4.3.1.1. “Leadership & Governance”
1- Developing databases: Thirty-three (97.14%) experts noted that polypharmacy management is completely influenced by developing comprehensive databases based on need assessment. Designing and developing related databases aims to restructure the row data for processing and producing information, effective storage, and retrieval. In this theme, two subthemes were identified:
- Developing electronic medical records (EMR): Twenty-two (62.85%) participants believed that physicians’ higher-level evidence-based decision-making based on EMR-enabled CDSS significantly contributes to polypharmacy management. Consequently, electronic medical records have a great potential to reduce the rate of inappropriate multi-medications during comorbidities. Most of the understudied experts stated that in many cases, the physicians’ incomplete information about the older adults’ medication history due to communication deficits or patients’ forgetfulness might be solved through EMR.
“EMR is the main support system, which assists physicians to overcome limited pharmacology knowledge, limited time or missing medical and medication history of patients (…)” (P12).
- Expanding electronic databases for the documentation of pharmaceutical interventions, medication errors, mortality, and morbidity: Thirty (85.71%) experts explicated their viewpoints by emphasizing the salience of establishing solid and accurate databases. They said that the pharmaceutical interventions for the elderly differ from those in the other age groups. Storing detailed demographic data, prescribed medications, drug-drug, and drug-disease interactions, adverse drug reactions, medication errors, morbidity, and mortality by exact reason clarifies the patterns and trends and can facilitate polypharmacy management.
“We should remember that polypharmacy management is absolutely time and resource-intensive. You should focus on big data analysis to reveal trends and associations collected from various sources in central databases (…).” (P24).
2- Optimizing homecare: Thirty-three (94.28%) interviewees mentioned homecare services as a kind of flexible, supportive care to older adults to support independent living and autonomy, financial security, patient safety, and a healthy mentality. In this theme, one subtheme was indicated:
- Technology-enabled homecare: Thirty-three (94.28%) interviewees expressed their opinions in favor of optimizing technology-enabled home care. They stated that by increasing comorbidities and diversification of the elderly needs with stroke, dementia, cardiovascular diseases, spinal cord injury, etc., technical infrastructures of home care services should be prepared in a specialized manner.
The interviewees mentioned “telemonitoring” as a patient management approach at homecare to remotely monitor and evaluate the elderly by promptly gathering physical, physiological, and behavioral data by healthcare professionals at a distance, especially for promoting medication adherence and managing polypharmacy. Mobile smartphones and personal digital assistants can also promote patient engagement in internalizing self-care and self-monitoring. Regarding appropriate medication and medication adherence, elderly-friendly technology can manage and remind patients of intake.
Another innovative technology in this field is sensor technologies, which include wearable devices and motion sensors to monitor the elderly and send alarm signals to caregivers in emergencies such as falls, heart failures, or extreme temperatures. In addition, communication technologies facilitate community-based social connectedness to overcome social isolation and its adverse health outcomes.
“Home care is equivalent to respect for the elderly.
Seniors stay at their homes and receive high-quality services owing to innovative technologies. We can remotely monitor, evaluate, and promote the elderly physical and mental health (…).” (P23).
4.3.1.2. “Financing”
The “structure” dimension also consisted of another block, “financing,” including one theme and two subthemes, as presented in Box 2.
| “Structure” in Leavitt’s Model |
|---|
| Financing (Six building blocks) |
| Theme 1: Pharmaceutical cost management in elderly care |
| Subthemes |
| - Value-based insurance design |
| - Automatic medicine refill program |
Theme and Subthemes of the Structure Dimension (Financing)
1- Pharmaceutical cost management in elderly care: Twenty-eight (80%) participants explained the crucial role of pharmaceutical cost management as a holistic system approach to optimize the quality and effectiveness of elderly care with comorbidities.
- Value-based insurance design: Twenty-one (60%) experts claimed that a value-based insurance design may benefit patients with multiple chronic conditions facing polypharmacy. Furthermore, they believed this plan should be precisely designed considering differences in health status.
“We require a kind of value-based insurance but in a controlled manner. It can promote service quality and decrease costs. Furthermore, we should provide safe and cost-efficient services based on financial incentives for physicians and pharmacists and prioritize consumer choices (…).” (P16).
The number of chronic conditions and prescribed medicines can influence the utilization of any services. As comorbidities increase, the patients get more inelastic in their demand for medical utilization. Therefore, more generous health insurance plans should be developed for the elderly with comorbidities, and the cost-sharing should be more protective to increase adherence and reduce the out-of-pocket burden.
Nine (25.71%) interviewees mentioned that the utilization of generic medicines usually decreases with an increase in chronic conditions. Changing the co-payment policy leads to considerable changes in service utilization. Increasing brand-name medicine co-payments and lowering the generic drugs’ co-payments may be a solution. Besides, while discussing their professional experiences, these interviewees noted case management or personalized homes as a potential solution for managing high-cost patients with complex concomitant disorders.
“I think the patient health outcomes should play a role in the payments to the health providers and cost-sharing model should be revised (…)” (P33).
- Automatic medicine refill program: Fourteen (40%) participants were convinced that automatic refill programs facilitate medication adherence and reduce pharmaceutical costs without adding to medication oversupply. In addition, such programs may directly or indirectly reduce mortality and morbidity among the elderly with comorbidities and decrease the wastage of medicines. As a result, health systems can use the saved budgets and reallocate them to improve the health outcomes of this age group.
“To manage costs in cases with polypharmacy to pay less for multi-medications and promote adherence, the automatic medicine refill program may be a solution (…)” (P8).
4.3.2. “Technology”
4.3.2.1. “Medicine & Technology”
The second dimension is “technology,” consisting of two blocks of the WHO Framework (medicine, technology, and information). The themes and subthemes are presented in Box 3.
| “Technology” in Leavitt’s Model |
|---|
| Medicine & technology (Six building blocks) |
| Theme 1: Development of medicine formulations |
| Subthemes |
| - Poly pills |
| - Precision medicine |
| Theme 2: Innovative technologies |
| Subthemes |
| Person-cantered technology-enabled care |
| Clinical decision support system |
| Additive manufacturing |
Theme and Subthemes of Technology Dimension (Medicine & Technology)
1- Development of medicine formulations: Twenty-seven (77.14%) interviewees discussed the impact of innovative medicine formulations on polypharmacy management by considering technological invention quality, especially in the area of effectiveness. Innovations in this field are of high medical and social importance due to their direct impact on patient’s health and decreasing side effects of the previously invented medicine formulations.
“New formulations balance the benefit to harm and reduce the drug-drug interventions by integrating formulation. Certain effectiveness is key in repurposing the existing medicine molecules, inventing new formulations or even producing target-based ones (…).” (P7).
- Polypills: Sixteen (45.71%) participants introduced the polypill or combo pill as an innovative solution for polypharmacy management and adherence promotion among the elderly.
One of the most crucial factors intensifying the adverse drug reactions and paradoxical effects is missed doses and lack of compliance. This matter increases healthcare costs by increasing morbidity, hospitalization, and even mortality and decreases the quality of life even for those who do not experience severe side effects.
It is established that the polypill approach and moving from multiple medications to one dose can improve adherence to prescribed medications and control potential side effects and risk factors simultaneously. However, some experts expressed their concern about the possibility of a polypill’s low efficacy and effectiveness due to the potential side effects of the components. This may lead to the complete loss of the polypill benefits.
Consequently, most participants confirmed the impact of polypharmacy on decreasing the dose frequency and lowering health system costs.
“Polypill is helpful because the elderly don’t get confused by multi-medication and if possible, they can take one pill instead of two, or three (…)” (P18).
- Precision medicine: Nineteen (54.28%) participants emphasized the importance of reconsidering pharmaceutical treatment with a new approach where exclusive and individualized pharmacotherapy is planned for every unique person. Polypharmacy often happens due to neglecting patient characteristics such as gender, age, comorbidities, history of drug intolerance or sensitivities, or other clinical and individual traits. The solution may be adopting a new insight toward the pharmaceutical manufacturing methods by considering individual body responses to medicines’ pharmacokinetic and pharmacodynamics properties.
The interviewees confirmed the potential of precision medicine as a subsequent solution in polypharmacy management by predicting the efficacy and effectiveness of medicine and even interactions or side effects on individuals.
“Approaching precision is the goal of many companies, simulating medicine’s effects and health outcomes in each person’s body in a personalized manner. An escape way from polypharmacy challenges (…)” (P35).
2- Innovative technologies: Eighteen (51.42%) interviewees considered pharmaceutical advancements and emerging innovative technologies as impressive facilitators for polypharmacy management by ensuring the safety and efficacy of pharmacotherapy in all phases of multi-medication, from manufacturing to preparation, distribution, and consumption. In this regard, three subthemes were identified and discussed.
- Person-centered technology-enabled care: Twelve (34.28%) participants agreed on the necessity of a global person-centered reorganization of the healthcare system, especially service delivery, to empower patients to monitor and manage their health status by benefiting from recent technologies. Some participants emphasized the electronic health (e-health) tools, person-centered technology-enabled care, and other technological infrastructures as a backbone for revolutionizing the care process of individuals with comorbidities and managing inappropriate polypharmacy.
In polypharmacy management, change management and service transformation are parallel with cultivating a person-centered, proactive healthcare system.
Person-centered technology-enabled care incorporates technological innovations and individuals’ values, priorities, and choices. Promoting patient engagement based on assistive technologies enhances the possibility of achieving expected treatment goals and health outcomes by increasing the effectiveness of patients’ and healthcare providers’ communication.
“I emphasize patient and family engagement. The person-centered TEC is a good alternative for empowering them using E-health tools, telemedicine, and tele-coaching. The elderly should be able to monitor their health status and control their wellbeing (…).” (P4).
- Clinical decision support system: Seventeen (34.28%) interviewees affirmed the salience of the clinical decision support systems (CDSS) in the physician’s clinical performance, especially regarding prescription behavior and reducing pharmaceutical errors. They believed that, in many cases, inappropriate polypharmacy and adverse drug reactions are due to prescription errors or inadequate information about patients’ pharmaceutical histories. The participants also confirmed the importance of having a user-friendly CDSS consisting of electronic health records, pharmaceutical information, guides, and alerts.
“In many cases, especially complex comorbidities, prescribing can be error-prone. Therefore, a very accurate and precise CDSS is required to optimize medication review and effectively assess the patient’s status. (…).” (P10).
Accordingly, the participants agreed on the positive impact of CDSS on increasing the efficacy of multi-medication and decreasing costs, mortality, morbidity, and prolonged hospitalization among the elderly with comorbidities.
“Traditional CDSS isn’t effective in this technology-driven era. The old systems just present guidelines that are proper for one single disorder or provide medical and pharmaceutical knowledge (…)” (P26).
The participants mentioned the importance of benefiting from innovative methods and developing new versions of CDSS for more comprehensive, easier, and faster data transfer between physicians and pharmacists. For facilitating this two-way discussion, they emphasized connecting previous approaches to new systems based on machine learning for medication review and control.
- Additive manufacturing: One of the participants claimed that “additive manufacturing” or “3D printing” based on rapid prototyping might be an outstanding, inexpensive, and innovative solution for producing personalized dosages for the elderly with long-term comorbidities. They believed this approach could maximize the medicine’s efficacy and minimize adverse drug reactions. As a strategy for polypharmacy management, “additive manufacturing” can even facilitate the combination of medicines, but quality control should be implemented precisely.
“Additive manufacturing is a revolution for polypharmacy management... with the help of this technology, medicine delivery system transformation is possible by taking into account variable demographic characteristics such as race, age, sex, pharmacokinetics, and pharmacodynamics differences (…).” (P22).
4.3.2.2. “Information”
The last block of the WHO framework discussed in this study is “information,” which is still related to the technology dimension. It includes one theme and one subtheme, as presented in Box 4.
| “Technology” in Leavitt’s Model |
|---|
| Information (Six building blocks) |
| Theme 1: Technology-based self-care |
| Subtheme |
| - Health literacy and e-health literacy |
Theme and Subtheme of the Technology Dimension (Information)
1- Technology-based self-care: Twenty-three (65.71%) interviewees emphasized technology-based therapeutic self-care as one of the key elements for overcoming polypharmacy challenges. It is about empowering the elderly with long-term chronic disorders to play a proactive role in taking the prescribed medications, avoiding interactions, and managing symptoms based on their health literacy, digital literacy, and e-health literacy.
“Providing self-care knowledge modifies their attitudes, encourages self-care behavior, and brings sustainability. Critically, the elderly should promote digital literacy to benefit from recent technologies, especially e-health tools (…).” (P20).
- Health literacy and e-health literacy: Thirteen (37.14%) participants claimed that electronic health literacy, digital literacy, and health literacy are principal determinants of helping the elderly with comorbidities to search, assess, and use available information to answer their pharmaceutical questions and follow medication orders.
“Technology-based therapeutic self-care focuses on self-monitoring (physiologic and psychologic parameters) and seeking care or consultation as needed. The success will be guaranteed by patients’ acceptable level of health literacy and digital literacy (…).” (P33).
The participants believed that health and e-health literacy could facilitate older adults’ well-informed decision-making.
“Health and e-health literacy are important in promoting the elderly’s health. Educational workshops should be conducted, and their knowledge level should be measured periodically. For instance, the e-Health Literacy Scale is a good indicator for evaluation. (…)” (P19).
The participants believed inappropriate polypharmacy could be associated with patient-related factors, such as poor health, e-health literacy, and weak patient-physician communications. Unfortunately, most elderly patients with comorbidities on multidrug regimens cannot comprehend all the care plan details or pharmaceutical instructions. Furthermore, if they face a problem, they cannot search and find more information on the Internet.
Furthermore, e-health literacy is a suitable alternative for the elderly to monitor their health status and adhere to instructions. Moreover, many elderlies face challenges, such as vision or hearing impairment, mobility limitation, memory deficiency, and cognitive deficits. In this case, the level of health literacy or e-health literacy may facilitate choosing an adaptive communication style to overcome these challenges and increase the chance of a complete understanding of medical recommendations.
Ten (28.57%) experts discussed the impact of sociodemographic and contextual factors on health and e-health literacy. Disparities in e-health literacy may be rooted in older adults’ education, income, and other characteristics. Still, we should provide equal opportunities for the elderly in various socioeconomic classes to promote their knowledge.
“As a health system, equitable services should be provided for vulnerable and deprived groups who don’t know about self-care or seeking help… Suppose we face a group of the elderly with low health and e-health literacy. In that case, we are responsible for facilitating their access to the necessary care without any difficulty, without putting them under pressure for learning new skills (…).” (P16).
One of the participants mentioned the Internet as the most available, affordable, and prominent platform for accessing health and pharmaceutical information, especially during crises or pandemics.
“During the COVID-19 pandemic, the Internet made it possible to inform people about all aspects of prevention, care, and treatment globally, available at any time and with low cost … Therefore, the Internet is a good means of informing the elderly about adherence, or drug reactions (…).” (P16).
One expert prioritized developing and introducing reliable information resources to the elderly. The critical point was to categorize the information sources to empower the elderly to utilize high-quality and trustable information.
“Internet is like a double-edged sword. If we do not introduce the right sites and sources of information to the elderly, we cannot guarantee the result, safety, and effectively (…)” (P16).
Higher e-health and health literacy generally lead to higher medication adherence and a healthy lifestyle. However, we should also provide enough accurate information and high-quality care for those with low e-health literacy.
5. Discussion
Due to the polypharmacy economic burden and its undesirable impacts on older adults’ health status, prolonged hospitalization, morbidity, mortality, and its’ intensifying effect on geriatric syndrome, including falls, frailty, memory deficiencies, etc., polypharmacy management is becoming increasingly a major health priority (19).
According to the results of our study, developing databases is another aspect of the technical view of polypharmacy management. Our study participants emphasized developing EMRs and expanding electronic databases to document pharmaceutical interventions, medication errors, morbidity, and mortality. In fact, due to poor communication, patients’ forgetfulness, and healthcare providers’ fatigue, anxiety, or frustration, the history-taking process may be inaccurate and incomplete. Therefore, electronic records provide detailed information about patients’ history and their medical and pharmaceutical interventions. In addition, establishing large databases facilitates megatrends and big data analysis. Wilfling et al. recommended the application of e-health technologies, especially big data analysis techniques, as a major solution to clarify trends, megatrends, and significant relationships among variables in large datasets. Big clinical data is typically built on a diverse range of sources. It is presumed that traditional statistical applications do not have the technical capability to analyze big data and reveal patterns. The authors also suggested that interdisciplinary collaboration between statisticians, information research scientists, and healthcare professionals should be promoted to interpret big data and extract solutions for polypharmacy management (20). Also, Kadra et al. demonstrated the impact of database and big data development on polypharmacy management and patient outcomes. They extracted APP data, which can facilitate the identification of polypharmacy, its trends, and predictors among the elderly with comorbidities and the prescription style that leads to inappropriate polypharmacy using electronic mental health records (21).
In line with our study's results, Flaherty et al. (22) also indicated that optimizing home care is an influential factor for polypharmacy management. Since hospitalization is significantly related to multi-medication and inappropriate polypharmacy, if the health system provides the most technology-enabled specialized home services and decreases the hospitalization duration, the polypharmacy challenges can be managed more easily. In contrast, a study by Giovannini et al. indicated that homecare might increase the prevalence of comorbidities and multi-medication and add to the complexity of patients’ conditions (23). In another study by Sun et al., this issue was discussed from a different perspective. The authors argued that we should provide specialized homecare services by professional caregivers. Furthermore, their results revealed that educating homecare nurses about effective multi-medication, safe prescribing, and the deprescribing process can be critical for polypharmacy management in parallel with developing technology-enabled home care (24).
According to the results of this study, another contributor to addressing polypharmacy management is pharmaceutical cost management through value-based insurance design and automatic medicine refill programs. It is crystal clear that pharmaceutical cost management and considering the financial aspect of prescribing for the elderly with comorbidities is a significant concern for managing polypharmacy. The price of prescription medicine should not be set per market tolerance. A value-based approach is a tool for tying the price of a medicine to the value it provides to patients in terms of efficacy. This pricing approach categorizes the medicines based on their impact on the patient’s quality of life. A study by Fendrick et al. (25) demonstrated that paying the same out-of-pocket for different health services without paying attention to their exact clinical benefit and indication can increase the probability of inappropriate polypharmacy, adverse drug reactions, and overuse of services without certain clinical benefits. However, a value-based approach is an efficient solution for overcoming these challenges (26, 27). In many cases, automatic medicine refill programs are part of the value-based insurance design, and the price of medicines decreases with the subsequent refill. Ma et al. revealed that automatic medicine refill programs enhance older adults’ adherence and polypharmacy management and also assist pharmaceutical cost management by reducing medication wastage (28).
Regarding the development of medicine formulations, innovative technologies, and technology-based self-care, the results of our study demonstrated that the recent innovative technologies are beneficial in involving seniors in managing their health status. Otherwise, health literacy, digital literacy, and consistent provision of education programs facilitate changes in elderly health knowledge, attitudes, and behaviors. Therefore, it can help control inappropriate polypharmacy (29).
Molokhia and Majeed recapitulated the future solutions for managing polypharmacy and transforming current trends. They claimed that the rapid development of new pharmaceutical formulations and technologies and innovative technology-based infrastructures such as electronic patient records could facilitate monitoring older adult patients (8). All processes, including prescribing, deprescribing, history-taking, and medication review, can be executed with greater precision. Additionally, developing e-health tools, such as smartphone applications, has promoted patient education, patient-physician communication, and technology-based self-care. Furthermore, while artificial intelligence and CDSS can optimize prescribing behavior and minimize errors by screening and monitoring drug-drug and drug-disease interactions, engaging the community, as a whole or each individual, to play a proactive role in maintaining the correct and accurate attitude and behavior towards managing medication consumption in line with therapeutic objectives is a cornerstone for effective polypharmacy management (30, 31).
Planning a future roadmap for polypharmacy change management depends on preparing the elderly with comorbidities, their caregivers, and healthcare providers. There is an emergent need to cope with the massive flow of information and communications resulting from technology systems and services. This transformation should facilitate the older adults’ movement toward safe medication based on access to accurate screened information. Consequently, approaching an e-health-driven socio-technical care system may have prominent salience on issues such as polypharmacy management.
5.1. Conclusions
A comprehensive technical polypharmacy change management approach should be planned and designed based on a holistic, person-centered, systematic approach, benefiting from the most innovative and recent enabling technologies. Adopting a systems-thinking approach and developing solutions based on top-down and bottom-up leadership and multidisciplinary collaborations can also be valuable.
Stimulating change management strategies for polypharmacy management in the elderly with comorbidities can improve medication safety and health outcomes and reduce costs.
In conclusion, designing and leading a holistic framework substantially depends on identifying socio-technical transitional factors. Furthermore, sustainable change can result from benchmarking, implementing, and evaluating solutions in different contexts. In addition, it is essential to prepare well-developed infrastructures and adopt innovative, user-friendly technologies.
