

Dear Editor,
A 56-year-old Indian female with skin Fitzpatrick type-V is presented with erythematous nodules and plaques on her upper extremities for the past two years. The lesions were asymptomatic and progressive. She had an occupational history of long-term exposure to sunlight. No other cutaneous areas had similar skin lesions.
The local cutaneous examination revealed hyperpigmentation and slightly erythematous, edematous, and smooth papulonodular lesions on the extensor surface of both her forearms. These lesions were coalescing into plaques, giving a mammillated appearance and some of them were seen to be arranged in irregular cord-like bands (Extension Extension to the medial and lateral sides of forearms were observed. The purpuric macules were also present. General and systemic examination were unremarkable. Routine laboratory parameters were also within normal limits.

Mammillated skin with smooth papules and nodules coalescing into plaques arranged in band-like fashion on both forearm
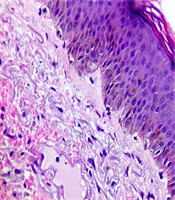
Histopathologic examination (HPE) on Hematoxylin and Eosin (H & E) staining revealed epidermal atrophy with effacement of the rete ridges. Dermis showed cleft-like spaces and bundles of degenerated elastic fibers composed of basophilic, granular materials in the dermis (Figure 2A and B). Spindle-shaped fibroblasts were seen along with mild perivascular lymphocytic infiltrates. Verhoeff Van-Gieson staining and electron microscopic studies could not be done due to the limited resources of the institution.
; B, bundles of degenerated basophilic fibrilar elastic fibres in the dermis along with some spindles fibroblasts around cleft like spaces (hematoxylin and eosin, original magnification 40×)")
A, Effacement of the rete ridges with superficial mild perivascular lymphocytic infiltrates and dermal cleft-like spaces in dermis (hematoxylin and eosin, original magnification 10×); B, bundles of degenerated basophilic fibrilar elastic fibres in the dermis along with some spindles fibroblasts around cleft like spaces (hematoxylin and eosin, original magnification 40×)
Although, elastotic changes in the skin of forearm are rarely reported, the histopathological findings were consistent with the diagnosis of solar elastosis. Therefore, we concluded with the diagnosis of solar elastotic bands of the forearm.
Solar elastosis is a pathological hallmark of photo-ageing, often seen as deposition of abnormal, amorphous granular materials within the dermis (1). Although, the exact origin of such materials is not determined, it has been attributed to both the degeneration of elastin fibers caused by chronic exposure of ultraviolet A rays and synthesis of abnormal elastin fibers by photodamaged fibroblasts (1). It leads to peculiar cutaneous changes such as hyperpigmentation, atrophy, thickening, telangiectasia, purpura, coarsening, wrinkling, and poikiloderma. It may also lead to development of some skin lesions, most commonly colloid milium, cutis rhomboidalis nuchae, Favre-Racouchot syndrome, elastotic striae, papular elastosis and anetoderma, and less commonly as acrokeratoelastoidosis of marginalis, elastosis linearis rubra nasi, upper and mid dermal elastolysis.
Of note, “Solar elastotic bands of forearm” is an extremely rare presentation of solar elastosis, which was coined and first described by Raimer et al. (1), in 1986 in his three Caucasian patients. Over the years, three more cases with similar clinical and histologic features were reported. The details of the clinical profile of previous cases have been summarized in Table 1 (2-4). In the most recent case, the role of sun exposure was denied probably based on the absence of history of long term sun exposure and involvement of only right forearm, although cutaneous signs of actinic damage such as senile purpura, atrophy, and coarsening of skin as well as histopathological changes were all in favor of solar elastosis (4).
| Serial Number of Cases | Author | Year | Age, y | Gender | Race | Site/s | History of Chronic Sun Exposure | Sign/s of Actinic Damage (Actinic Purpura, Atrophy) |
|---|---|---|---|---|---|---|---|---|
| 01 | Raimer et al. (1) | 1986 | 83 | Female | Caucasian | Flexors of both forearms | Present | Present |
| 02 | Raimer et al. (1) | 1986 | 63 | Male | Caucasian | Flexors of both forearms | Present | Present |
| 03 | Raimer et al. (1) | 1986 | 71 | Male | Caucasian | Flexors of both forearms | Present | Present |
| 04 | Stanford et al. (2) | 1995 | 43 | Female | Caucasian | Extensor of right forearm | Present | Present |
| 05 | Kiyohara et al. (3) | 2003 | 68 | Male | Japanese | Flexural surface of forearm, shoulder and chest | Present | Present |
| 06 | Haga et al. (4) | 2015 | 57 | Female | Japanese | Extensor of right forearm | Absent | Present |
| 07 | Our case | 2018 | 56 | Female | Caucasoid (Indian) | Extensors of both forearms | Present | Present |
Clinical Profiles of Previous Similar Cases Reported in English Literature
Solar elastotic bands characteristically appear on the forearm/s presenting as mostly asymptomatic, skin colored or yellowish, papules, and nodules merging to form plaques and cord-like bands (1). The classical histopathology on H & E staining shows normal or atrophic epidermis with effaced rete ridges. The dermis shows large nodular collections composed of abnormal amorphous and basophilic elastic fibrils and cleft-like spaces (4). Staining with Verhoeff-van-Gieson can be done to see the thick and serpiginous bundles of elastic fibers. A mild perivascular lymphocytic infiltrates and spindled fibroblasts are seen in opposition to the elastotic fibers. Capillary dilatation may also be observed with some hemorrhagic foci in papillary dermis.
The cutaneous amyloidosis and focal mucinoses are usually considered as differential diagnosis. The histopathologic examination with proper staining can easily rule out these entities (1). Congo red staining can be done to show the amyloid deposits, which gives apple-green birefringence under polarized light. Mucin deposition can be stained by alcian blue, mucicarmine, or PAS. The elastotic lesions are usually persisting and recalcitrant to keratolytics, and do not vanish over time even with photoprotection (3).
Solar elastotic bands of the forearm is a rare presentation of actinic elastosis, with very few cases reported in English literature. The involvement of atypical sites with characteristic histopathological features of elastosis warrant the need of HPE in all cases, irrespective of pattern of involvement.
