



1. Background
Adolescence is one of the most critical stages of life. Puberty is the most significant change in this period, which is of special importance and mentioned as a transition in the life of adolescents. Puberty is a process through which a child changes physically into an adult with the ability to reproduce (1). There are an estimated 1.8 billion adolescents in the world, 90% of whom live in low- and middle-income countries (2). According to the 2011 census, about 12 million of the Iranian population is in the age range of 10 - 19 years old, around 50% of whom are girls (3).
From the onset of puberty, girls are exposed to a variety of physical and psychological problems, such as iron deficiency, malnutrition, urinary tract infections, sexually transmitted infections, premenstrual syndrome, miscarriage, pregnancy at a young age, etc., experienced by them for the first time (4). Therefore, it is very important to pay attention to puberty hygiene, including care and principles, which lead to maintenance and promotion of mental, physical, and emotional health (5). Such behaviors include puberty hygiene, genital hygiene, correct nutrition, taking iron pills, pain management strategies, sports, and physical activities, etc. (6).
Since the symptoms of puberty appear one after the other, lack of awareness about this period may cause confusion and numerous problems for adolescents (1, 5), leading to tension, anxiety, and psychological stress (7). Studies indicate the level of knowledge and awareness of girls concerning puberty has been reported to be low in other countries (8). Studies in Iran also show that the level of awareness of adolescent girls about puberty and proper health behaviors towards this phenomenon is much lower than expected (5, 6, 8). This can be the result of parental failure to transfer accurate information to daughters, which is due to poor awareness, low level of education, and lack of proper and close communication between parents and adolescents (9). Lack of proper education, access to wrong information, embarrassment, and inattention to genital hygiene hinder the achievement of social and mental health for the young girls, making them not feel positive about themselves and their abilities (7).
Behavioral patterns that begin during adolescence have a major impact on individuals’ health in later years. The development of beneficial health habits during childhood and early adolescence is very important because behaviors that begin in adolescence tend to continue into adulthood (1).
Integrated Behavioral Model (IBM) is one of the comprehensive and predictive models for the examination of health-promoting behaviors (10). According to IBM, determinants of individuals’ behavioral intention are their experiential and instrumental attitudes towards the behavior, their descriptive and injunctive norms, and their perceptions about the difficulty or ease of conducting the desired behavior and perceived self-efficacy (10). Based on a researcher review, no research has previously used IBM method for puberty health behaviors, the results of studies using the theory of planned behavior and other models indicate the effectiveness of these models in the promotion of health behaviors during puberty (11-14).
2. Objectives
Given the above mentioned and considering the importance of girls' health, extensive research on puberty health and efforts to improve its level is an investment toward the improvement of individual and social health. Therefore, the aim of this study was to determine the predictors of health behaviors during puberty based on IBM in girl’s secondary school students in Birjand.
3. Methods
This descriptive-analytical study was conducted on 265 first-grade girls’ secondary school students in Birjand in 2020 using multi-stags sampling. According to the mean score of students' behavior in the study of Eslamimehr et al. (15) and following formula n = Z2.S2/d2 (in which α = 0.05 and d = 0.37), sample size was determined 177 people; which according to the design effect = 1.5, 265 students were included in the study. Firstly, Birjand was divided into four regions (North, South, East, and West) based on geographical location. As in the East of Birjand, the student population density and the number of schools were lowest; one school was selected from the East. In addition, two schools were randomly selected from each other areas (North, South, and West). Then in each school, a list of eight-grade students was obtained. Then researcher randomly called mother of each student and described the aim of the study and inclusion criteria. Then, according to mother’s consent, students were invited to school and fill out the questionnaire. This process was continued until enrollment of 37 or 38 students in each school.
Sampling was done during three months from December 2020 to February 2021 after obtaining the consent of the parents and students (individuals who met the inclusion criteria). Individuals were reassured about the confidentiality of information and the anonymity of the questionnaires. Inclusion criteria were informed consent to participate in the study, menarche experience, lack of physical and mental disability, eighth-grade student (range of 13 - 14 years), and residence in Birjand. Exclusion criteria were defects in the completion of the questionnaire. The data collection tool was a researcher-made questionnaire organized in two sections. The first section included questions on demographic information (age, mother and father’s level of education, mother and father's job, birth rank, number of sisters), and the second section included 54 questions related to IBM constructs (awareness, experiential attitudes, instrumental attitudes, injunctive Norm, descriptive Norm, Control beliefs, behavioral intention, self-efficacy, and behavior). The questions related to the awareness and behavioral intention were of the yes-no type, and the 3-score Likert scale was used at a range of agree to disagree for the rest of the sections.
Content validity of the questionnaire [content validity ratio (CVR) and the Content Validity Index (CVI)] was verified by 10 experts in the field of health education and health promotion. For evaluating the CVR, participating experts rated each item on a 3 point Likert format (i.e., necessary, helpful but not necessary, and not necessary). Based on the numbers given in the Lawsche table, the item was considered necessary, if the CVR value was greater than 0.62 (16). The pattern described by Lynn was used for calculating the CVI. For this reason, the experts rated each item concerning its clarity [1 ("not clear") to 4 ("strongly clear")], simplicity [ranging from 1 ("not simple") to 4 ("strongly simple")], and relevance [ranging from 1 ("not relevant") to 4 ("highly relevant")]. Items that received a score of more than 0.78 were retained in the questionnaire (17).
A pilot study was conducted on 20 students who matched the study sample but did not participate in the study to evaluate the reliability of the questionnaire. The questionnaire was completed twice with an interval of one week, and its correlation was 0.602 - 0.847 in two stages. Also, the internal consistency of items was evaluated using Cronbach’s alpha. The Cronbach's alpha coefficient for the whole instrument and each of its subscales was 0.632 - 0.824.
The collected data were entered into SPSS19 and analyzed using descriptive and analytical statistics. Pearson correlation coefficient, and linear regression analysis were used and P < 0.05 was considered significant.
4. Results
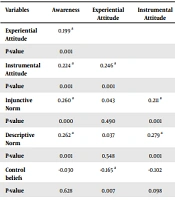
In this study, 265 girls secondary school students in Birjand were studied. The mean age of students and mothers was 13.5 ± 0.5 and 42.2 ± 5.8 years, respectively. Most mothers (50.6%) and fathers (59.6%) had guidance school to diploma education. Regarding occupations, 62.3% of fathers were self-employed, and 84.2% of women were housewives, 44.9% of the students were the first child, and 47.2% of them had a sister (Table 1). The mean score and standard deviation of all model constructs was provided in Table 2. Pearson correlation test between the constructs of the integrated behavioral model showed that all constructs except experiential attitudes and Control beliefs had a significant correlation with puberty health behaviors (P < 0.001). In this regard, the highest positive and significant correlations were between intention, self-efficacy, descriptive norm, injunctive norm, awareness, and instrumental attitudes with puberty health behaviors, respectively (Table 3).
| Variables | Frequency | Percentage |
|---|---|---|
| Educational status of Mother | ||
| Elementary and less | 96 | 36.2 |
| Middle , high school, and diploma | 134 | 50.6 |
| Above the diploma | 35 | 13.2 |
| Educational status of father | ||
| Elementary and less | 63 | 23.8 |
| Middle , high school and Diploma | 158 | 59.6 |
| Above the diploma | 44 | 16.6 |
| Mother's job | ||
| Housewife | 223 | 84.2 |
| Employee | 21 | 7.9 |
| Freelance | 21 | 7.9 |
| Father's job | ||
| Employee | 71 | 26.8 |
| Freelance | 165 | 62.3 |
| Other jobs | 29 | 10.9 |
| Birth rank | ||
| One | 119 | 44.9 |
| Two | 81 | 30.6 |
| Three and more | 65 | 24.5 |
| Number of sisters | ||
| Zero | 69 | 26 |
| One | 125 | 47.2 |
| Two and more | 71 | 26.8 |
Frequency Distribution of Demographic Information of the Subjects
| Variables | Number of Items | Response Range | Minimum | Maximum | Mean | Std. Deviation |
|---|---|---|---|---|---|---|
| Awareness | 12 | 0 - 12 | 0.00 | 12.00 | 6.76 | 2.17 |
| Experiential attitude | 5 | 5 - 15 | 6.00 | 15.00 | 12.12 | 2.18 |
| Instrumental attitude | 7 | 7 - 21 | 11.00 | 20.00 | 15.26 | 1.97 |
| Injunctive norm | 6 | 6 - 18 | 6.00 | 18.00 | 11.69 | 2.45 |
| Descriptive norm | 5 | 5 - 15 | 5.00 | 15.00 | 10.80 | 1.95 |
| Control beliefs | 6 | 6 - 18 | 6.00 | 17.00 | 11.49 | 1.93 |
| Self-efficacy | 5 | 5 - 15 | 7.00 | 15.00 | 11.24 | 1.57 |
| Behavioral intention | 4 | 0 - 4 | 0.00 | 4.00 | 2.66 | 0.92 |
| Behavior | 4 | 4 - 12 | 4.00 | 12.00 | 9.17 | 1.53 |
Minimum, Maximum, Mean, and Standard Deviation of Integrated Behavioral Model Constructs in the Studied Students
| Variables | Awareness | Experiential Attitude | Instrumental Attitude | Injunctive Norm | Descriptive Norm | Control Beliefs | Self-efficacy | Behavioral Intention |
|---|---|---|---|---|---|---|---|---|
| Experiential attitude | 0.199 a | |||||||
| P-value | 0.001 | |||||||
| Instrumental attitude | 0.224 a | 0.246 a | ||||||
| P-value | 0.001 | 0.001 | ||||||
| Injunctive norm | 0.260 a | 0.043 | 0.211 a | |||||
| P-value | 0.000 | 0.490 | 0.001 | |||||
| Descriptive norm | 0.262 a | 0.037 | 0.279 a | 0.550 a | ||||
| P-value | 0.001 | 0.548 | 0.001 | 0.001 | ||||
| Control beliefs | -0.030 | -0.165 a | -0.102 | 0.067 | -0.005 | |||
| P-value | 0.628 | 0.007 | 0.098 | 0.275 | 0.940 | |||
| Self-efficacy | 0.286 a | 0.154 b | 0.276 a | 0.335 a | 0.324 a | -0.203 a | ||
| P-value | 0.001 | 0.012 | 0.001 | 0.001 | 0.001 | 0.001 | ||
| Behavioral intention | 0.225 a | 0.003 | 0.207 a | 0.481 a | 0.484 a | -0.016 | 0.419 a | |
| P-value | 0.001 | 0.966 | 0.001 | 0.000 | 0.001 | 0.792 | 0.001 | |
| Behavior | 0.171 a | 0.004 | 0.204 a | 0.351 a | 0.372 a | -0.031 | 0.576 a | 0.650 a |
| P-value | 0.005 | 0.942 | 0.001 | 0.001 | 0.001 | 0.615 | 0.001 | 0.001. |
Correlation Coefficients Between the Structures of the Integrated Behavioral Model in the Studied Students
All demographic variables and model constructs (awareness, experiential and instrumental attitudes, injunctive and descriptive norms, control believes and perceived self-efficacy, intention) were included in the study as independent variables, and health puberty behavior was considered as outcome. All qualitative variables were defined as dummy variables (baseline in education variable was “above the diploma”, mothers' job baseline was “freelance” and fathers' job baseline was “other jobs”). The final model was selected using the step-by-step method.
According to the results of the linear regression test, the predictors of puberty health behaviors in the studied girls were the constructs of behavioral intention, self-efficacy, and mother's job, respectively. Besides, about 54% of puberty health behaviors were predicted by these variables (Table 4). According to the results, with one-unit increase in the intention score, the behavior increased by 0.8 points on average (P = 0.001), and with one-unit increase in the self-efficacy score, the behavior increased by 0.36 points on average (P = 0.001). Also, girls whose mothers were housewives showed a 0.42 lower behavioral score than freelance (P = 0.02).
| Variables | Unstandardized Coefficients | Standardized Coefficients Beta | t | P-value | 95.0% Confidence Interval for B (Lower Bound - Upper Bound) | |
|---|---|---|---|---|---|---|
| B | Std. Error | |||||
| Behavioral intention | 0.806 | 0.077 | 0.484 | 10.446 | 0.000 | 0.648 - 0.953 |
| Self-efficacy | 0.352 | 0.045 | 0.362 | 7.844 | 0.000 | 0.267 - 0.444 |
| Housewife mothers (baseline: freelance) | -0.416 | 0.178 | -0.099 | -2.33 | 0.020 | 0.766 - 0.065 |
| P = 0.001 | F = 103.817 | R2 = 0.54 | ||||
Estimation of Linear Regression Coefficients of Intent, Self-efficacy, and Maternal Occupation Structures for Puberty Health Behaviors
5. Discussion
This study aimed to determine the predictors of puberty health behaviors based on an integrated behavioral model in girl’s secondary school students. The mean of performing puberty health behaviors in the studied students was 9.17 ± 1.53 (response range of this construct was 4 - 12). The most important predictors of puberty health behavior were behavioral intention self-efficacy, and Mother's job.
The present study showed that intention was the most significant predictor of puberty health behaviors, and higher levels of students' intention to perform puberty health behaviors led to more likelihood to show such behaviors. In the study of Eslamimehr et al. also intention to perform puberty health behaviors predicted these behaviors (1). Also, results of Plotnikoff et al. showed that intention was predictor of health behaviors among a large sample of overweight and obese adolescents (Alberta, Canada), using a web-based survey (18). In the study of Tapera et al., smoking was predicted by attitudes, subjective norms, perceived behavioral control, and intention (19). The behavioral intention was introduced as the predictor of behavior in the study of Baji et al., which was conducted to investigate and identify the factors affecting students' nutritional behaviors using the modified reason action theory (20). Behavior generally follows intention, and the stronger the intention to adopt a behavior, the more success is expected to be achieved (10). According to IBM, the most important factors that lead to the promotion of intention and consequently the performance of puberty health behaviors are the constructs of attitude, subjective norm, self-efficacy, and behavioral control (10). In fact, when a person has a positive attitude about performing puberty health behaviors and feels that he has the ability to perform such behaviors and environmental factors are at his disposal and will, the intention to perform puberty health promotion behaviors is strengthened in him, and as a result, health behaviors increase. In the meantime, the role of important others in one's life such as mother, sister, friends, and peers in influencing puberty health behaviors should not be forgotten.
The next predictor of puberty health behaviors in the present study was students' self-efficacy in overcoming obstacles to puberty health behaviors. Also, the mean score of perceived self-efficacy of students indicated that most of the girls considered themselves to be efficient in puberty health behaviors. The importance of self-efficacy in puberty health can be seen in its correlation with behavior so that with the increase in self-efficacy, puberty health behaviors increased in the present study. Similarly, in the study of Karimy et al., perceived self-efficacy was a significant factor for adolescents smoking habits (21). Ziapour et al. found that increasing self-efficacy increased health behaviors (9). Also, Chan et al. reported that self-efficacy predicted healthy eating (22). Baji et al. also showed that self-efficacy had the highest correlation with students' nutritional intentions and behaviors (20). Self-efficacy is a behavioral perception that increases commitment to a work plan and plays a key role in the acceptance, maintenance, and persistence of health behaviors, representing the most important personal factor in behavioral changes (23). Perceived self-efficacy refers to a person's ability to perform the behavior successfully and achieve the expected results. This concept overshadows the individual's level of effort and level of performance. Self-efficacy is the mediator between knowledge and practice (10). People with high self-efficacy are more inclined to participate in challenging behaviors and provide a better interpretation of health behaviors, and can easily control their behaviors. On the other hand, in adolescence, a person faces new challenges. How to cope with these challenges is partly influenced by one's self-efficacy beliefs.
Also, Mother's job was a predictor of puberty health behaviors in this study, and girls who had housewife mothers showed a lower behavior score than others. However, this finding was not consistent with a study conducted by Kashefi et al. (24) on students in Bojnourd. This issue needs a more comprehensive investigation. However, by educating mothers and increasing their knowledge, we can see the improvement of their daughters' awareness and practice towards puberty health.
The most important strength of this study is its focus on puberty. Given that half of Iran's adolescent population is girls; however, the basic issues of this vulnerable group -for cultural and social reasons- have been neglected. In this article, researchers have addressed one of the most important issues of adolescents, namely puberty.
Several limitations in this study should be acknowledged. The first limitation relates to the fact that the sample of this study was composed solely of girls’ high school students of the Birjand city. So, the results of this study should be generalized with caution since they were developed based on a regional sample. In addition, collection of data in this study was based on the researcher-made questionnaire and self-report. So, the possibility of over-report or under-report by the samples should be taken into account (of course, this limitation was addressed to some extent by stating the objectives of the study and assuring students regarding confidentiality of their information).
5.1. Conclusion
According to the results of this study, the integrated behavioral model can be used as a suitable model to predict adolescent health behaviors in girl’s students. The constructs of intention, self-efficacy and maternal occupation were the most important predictors of adolescent health behaviors in the present study. Therefore, it seems necessary to pay attention to the intention to perform behaviors and self-efficacy in line with puberty health behaviors. It is also important to consider the above factors in educational and research planning.
