



1. Background
Coronaviruses are a large family of viruses that can cause anything from a simple cold to more severe illnesses, such as Middle East respiratory syndrome (MERS) and severe acute respiratory syndrome coronavirus (1). On January 30, 2020, the World Health Organization declared the new coronavirus, coronavirus disease 2019 (COVID-19), a Public Health Emergency of International Concern and as the sixth public health threat emergency that needs international attention (2). The prevalence of COVID-19 in Iran began in March 2019 with the identification of two positive cases in Qom, and the number of total cases reached 6 million and 128000 mortalities by November 2021 (3).
The most important clinical signs of admitted patients with COVID-19 t the hospital are fever, dry cough, respiratory problems, headache, vomiting, diarrhea, fatigue, rhinorrhea, and chest pain (4). In more severe cases, the infection can cause pneumonia, acute respiratory syndrome, kidney failure, and even death (5). The current epidemiological data show that the mortality rate of COVID-19 patients with severe symptoms is about 20 times higher than that of those with mild symptoms (6).
The patients develop dyspnea after the onset of the disease, and severe cases can quickly suffer from dysfunction of some organs. Acute respiratory dyspnea syndrome, septic shock, acute heart and kidney damage, blood clotting disorders, and even death might be the symptoms (7). The awareness of the prevalence of these symptoms is of particular importance for the initial identification and screening of patients. The standard laboratory method for the current diagnosis of the disease is a real-time polymerase chain reaction (PCR). In addition, laboratory and radiological findings are used to diagnose the disease, especially in the early stages (8). Patients admitted to the intensive care unit (ICU) usually have serious problems and various underlying diseases that can affect patient mortality (9).
2. Objectives
This study investigated the clinical features, and outcome of patients with CIVID-19 admitted to the ICU of Valiasr Hospital, Birjand University of Medical Sciences, Birjand, Iran, in 2020 (March to December).
3. Methods
3.1. Study Design and Participants
In the beginning, the code of ethics was received from the Vice-Chancellor for Research and Technology of Birjand University of Medical Sciences. All patients with COVID-19 admitted to the ICU of Valiasr Hospital (n = 157) were the statistical population. The inclusion criterion was a positive real-time PCR, and the exclusion criterion was the lack of patient’s electronic file. In this cross-sectional study, 111 of 157 patients were entered the study using convenience sampling. After designing the study checklist, the following information was collected: (1) demographic characteristics (e.g., age and gender); (2) comorbidities; (3) vital signs when admitting to the ICU [e.g., temperature, heart rate, arterial oxygen saturation with and without oxygen therapy, respiratory rate (RR), and blood pressure]; (4) clinical symptoms (e.g., fever, cough, dyspnea, sore throat, sputum, rhinorrhea, muscle pain, weakness and lethargy, chest pain, abdominal pain, headache, nausea and vomiting, hemoptysis, anosmia, seizures, anorexia, skin lesions, and conjunctivitis); (5) radiological findings [e.g., chest X-ray (CXR) and high-resolution computed tomography (HRCT)]; (6) oxygen therapy (e.g., high flow nasal cannula, simple facial mask, facial mask with reserve bag, noninvasive ventilation, and invasive mechanical ventilation (IMV)]; (7) patient outcomes (e.g., the length of hospital stay before ICU, ICU stay, and length of hospital stay after ICU); (8) two clinical scores for ICU (i.e., acute physiology and chronic health evaluation II (APACHE II) and Glasgow Coma Scale (GCS)] (10-12).
3.2. Data Analysis Method
The data were entered into SPSS software (version 22) for analysis, and then statistical tests were performed for comparing the survived and nonsurvived groups. The data were expressed as mean (standard deviation) or median (interquartile range) for continuous variables and number (%) for class variables. If continuous variables have a normal distribution according to the Kolmogorov-Smirnov test, the mean, and otherwise the median was used in the tests (13, 14). The independent t-test, chi-square test, Mann-Whitney U test, and Fisher’s exact test were used to compare the survived and nonsurvived groups at 95% confidence level where appropriate.
4. Results
The findings showed that out of 111 patients admitted to the ICU, 59 (53.2%) subjects died, and 52 (46.8%) cases were discharged from the ward. The mean age of all patients was 65.15 ± 15.37 years, with a minimum and maximum of 24 and 94 years, respectively. Furthermore, the mean age values of the survivors and nonsurvivors were 71 ± 11.87 and 58.4 ± 15.9 years, respectively; therefore, there was a difference between the age of the two groups (P < 0.001).
By categorizing the age of patients into five groups based on Yang et al.’ study (12), the highest frequency was related to patients over 75 years of age. Table 1 shows that the numbers of mortalities within the age ranges of over 75 and under 44 years were the highest and lowest, respectively. In the case of patients discharged from the ICU, the highest and lowest numbers were related to the ranges of under 44 and 45 - 54 years, respectively (Table 1). Therefore, there was a relationship between the age group and mortality. In other words, there was a higher mortality rate in the older age groups and a greater improvement in the younger age groups. Table 2 shows that there is no significant difference in the number of male and female patients in total (P = 0.40), survived (P = 0.57), and nonsurvived (P = 0.51).
| Variables | All Patients (n = 111) | Survivors (n = 59) | Nonsurvivors (n = 52) | P-Value |
|---|---|---|---|---|
| Age | 65.15 ± 15.37 | 71 ± 11.87 | 58.4 ± 15.9 | < 0.001 |
| Age range (y) | < 0.001 | |||
| < 44 | 14 (12.6) | 13 | 1 | |
| 45 - 54 | 14 (12.6) | 7 | 7 | |
| 55 - 64 | 20 (18.0) | 12 | 8 | |
| 65 - 74 | 28 (25.2) | 9 | 19 | |
| > 75 | 35 (31.5) | 11 | 24 |
Characteristics of Age Groups of Patients a
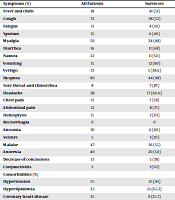
Table 3 shows that clinical symptoms, including diarrhea (P < 0.001), sore throat (P < 0.001), and hemoptysis (P < 0.001), statistically differ between the two groups. In addition, regarding the symptoms, there was a significant difference in coronary heart disease (P < 0.001), chronic obstructive lung disease (COPD) (P = 0.03), history of influenza vaccine (P < 0.001), and cerebrovascular accident (P = 0.03) between the two groups. Moreover, the frequency of RR (≥ 26 breaths/minute) in nonsurvivors was significantly higher than in survivors (P = 0.01). On the other hand, five methods of supportive oxygen therapy were considered for patients admitted to the ICU. The results showed that in the group of survivors, 52 patients needed to use supportive methods (P < 0.001). Accordingly, at the time of ICU admission, only one patient (1.7%) in the nonsurvivors used IMV; however, 54 patients (91%) of this group needed to use IMV at the time of death. Therefore, out of the total number of patients, 60 patients needed to use IMV, and 6 intubated patients were recovered and extubated (Table 3). The comparison of the two groups showed that hospitalization duration before the ICU (P = 0.15) and ICU stay duration (P = 0.43) were significantly different between the groups. The mean values of APACHE II scores among all patients at the time of ICU admission and discharge were 14.65 and 20.18, respectively. Furthermore, the GCS scores were 14.44 and 9.27 at the time of ICU admission and discharge, respectively (Table 4).
| Symptoms (%) | All Patients | Survivors | Nonsurvivors | P-Value |
|---|---|---|---|---|
| Fever and chills | 81 | 41 (51) | 40 (49) | 0.91 |
| Cough | 72 | 38 (52) | 34 (48) | 0.63 |
| Fatigue | 13 | 4 (30) | 9 (70) | 0.16 |
| Sputum | 15 | 6 (40) | 9 (60) | 0.43 |
| Myalgia | 50 | 24 (48) | 26 (52) | 0.77 |
| Diarrhea | 16 | 11 (68) | 5 (34) | < 0.001 |
| Nausea | 22 | 11 (50) | 11 (50) | 0.08 |
| Vomiting | 15 | 12 (80) | 3 (20) | < 0.001 |
| Vertigo | 13 | 5 (38.6) | 8 (61.5) | 0.40 |
| Dyspnea | 90 | 44 (48) | 46 (52) | 0.83 |
| Sore throat and rhinorrhea | 8 | 7 (87) | 1 (13) | < 0.001 |
| Headache | 28 | 17 (60.6) | 11 (39.4) | 0.25 |
| Chest pain | 12 | 7 (58) | 5 (42) | 0.56 |
| Abdominal pain | 12 | 8 (75) | 4 (25) | 0.24 |
| Hemoptysis | 15 | 3 (20) | 12 (80) | < 0.001 |
| Rectorrhagia | 0 | 0 | 0 | - |
| Anosmia | 10 | 6 (60) | 4 (40) | 0.57 |
| Seizure | 5 | 1 (20) | 4 (80) | 0.18 |
| Malaise | 47 | 26 (55) | 21 (45) | 0.46 |
| Anorexia | 40 | 20 (50) | 20 (50) | 1.00 |
| Decrease of conciseness | 13 | 5 (38) | 8 (62) | 0.40 |
| Conjunctivitis | 2 | 1 (50) | 1 (50) | 1.00 |
| Comorbidities (%) | ||||
| Hypertension | 55 | 25 (45) | 30 (55) | 0.50 |
| Hyperlipidemia | 23 | 15 (65.2) | 8 (34.8) | 0.14 |
| Coronary heart disease | 35 | 9 (25.7) | 26 (74.2) | 0.00 |
| Diabetes mellitus | 46 | 18 (39.1) | 28 (60.8) | 0.14 |
| COPD | 1 | 5 (26.3) | 14 (73.6) | 0.03 |
| Asthma | 3 | 2 (66.6) | 1(33.3) | 0.56 |
| Malignancy | 10 | 2 (20) | 8 (80) | 0.05 |
| Chronic kidney disease | 8 | 2 (25) | 6 (75) | 0.15 |
| Chronic liver disease | 3 | 0 | 3 (100) | - |
| Smoking | 4 | 2 (50) | 2 (50) | - |
| Drug addiction | 14 | 8 (57.1) | 6 (42.8) | 0.59 |
| Rheumatoid arthritis | 2 | 2 (100) | 0 | - |
| Malnutrition | 2 | 1 (50) | 1 (50) | 1.00 |
| Androgenic alopecia | 12 | 5 (8.3) | 7 (91.7) | 0.56 |
| Influenza vaccination history | 12 | 1 (1.9) | 1 (18.6) | 0.00 |
| Anticoagulant therapy | 3 | 2 (66) | 2 (66) | 0.56 |
| Psychological disease | 13 | 3 (23) | 3 (23) | 0.05 |
| CVA | 11 | 2 (18) | 2 (18) | 0.03 |
| Gastrointestinal disease | 15 | 7 (46) | 7 (46) | 0.79 |
| Hepatitis | 2 | 1 (50) | 1 (50) | 1.00 |
| Tuberculosis | 2 | 1 (50) | 1 (50) | 1.00 |
| Anemia | 2 | 1 (50) | 1 (50) | 1.00 |
| Thyroid dysfunction | 8 | 5 (62) | 5 (62) | 0.48 |
| Paralysis | 2 | 1 (50) | 1 (50) | 1.00 |
| HRCT | ||||
| Consolidation | 60 | 45 (44) | 33 (56) | 0.60 |
| Ground glass | 90 | 42 (47) | 48 (53) | 0.40 |
| Patchy infiltrates | 78 | 37 (48) | 41 (52) | 0.20 |
| Lymphadenopathy | 50 | 23 (46) | 27 (54) | 0.32 |
| Pleural effusion | 38 | 12 (32) | 26 (68) | 0.02 |
| Pleural thickness | 24 | 9 (37) | 15 (63) | 0.16 |
| CXR | ||||
| Unilateral infiltrates | 3 | 1 (34) | 2 (66) | 0.56 |
| Diffuse bilateral infiltrates | 88 | 41 (47) | 47 (53) | 0.52 |
| Pneumothorax | 5 | -- | 5 (100) | - |
| Increased bronchovascular markings | 26 | 8 (30) | 18 (70) | 0.05 |
| Vital Sings | ||||
| Temperature | 37.2 | 37.5 (1.3 | 37.4 (1.0) | < 0.001 |
| SPO2 without oxygen therapy | 84.5 | 86.3 (6.7) | 82.7 (8.6) | < 0.001 |
| SPO2 with oxygen therapy | 92.2 | 93.4 (5.0) | 91.3 (6.3) | < 0.001 |
| RR | 21.4 | 19.2 (3.0) | 23.7 (9.1) | < 0.001 |
| SBP | 124.0 | 124.0 (19.3) | 123.3 (20.9) | < 0.001 |
| DBP | 76.1 | 76.9 (13.7) | 75.4 (13.7) | < 0.001 |
| MAP | 92.1 | 92.8 (14.3) | 91.3 (13.5) | < 0.001 |
| HR | 91.9 | 92.6 (12.7) | 91.2 (17.0) | 0.52 |
| Oxygen Therapy on Admission | ||||
| High flow nasal cannula | 54 | 24 (45) | 30 (55) | 0.49 |
| Facial mask | 16 | 12 (75) | 4 (25) | 0.46 |
| Mask with reserve bag | 25 | 13 (37.2) | 22 (62.8) | 0.17 |
| NIV | 3 | 1 (33.4) | 2 (66.6) | 0.56 |
| IMV | 3 | 2 (66.6) | 1 (33.4) | 0.56 |
| Oxygen Therapy on Discharge | ||||
| High flow nasal cannula | 16 | 16 (100) | - | - |
| Facial mask | 7 | 6 (85.7) | 1 (14.3) | 0.37 |
| Mask with reserve bag | 23 | 22 (95.6) | 1(4.4) | < 0.001 |
| NIV | 5 | 2 (40) | 3 (60) | 0.65 |
| IMV | 60 | 6 (10) | 54 (90) | < 0.001 |
| Hospitalization Duration | ||||
| Hospital stay duration before ICU admission | 4.9 | 5.7 (4.0) | 3.5 (3.7) | 0.15 |
| ICU stay | 8.4 | 8.1 (9.5) | 8.1 (6.5) | 0.43 |
| Hospital stay duration after ICU | 4.9 | 4.91 (3.3) | - | - |
Symptoms, Comorbidities, Radiologic Findings, Vital Signs, Oxygen Therapy Methods, and Intensive Care Unit Duration Between Survivors and Nonsurvivors
| Variables | ICU Admission | ICU Discharge | ||
|---|---|---|---|---|
| Survivors | Nonsurvivors | Survivors | Nonsurvivors | |
| APACHE II | 12.63 (7.3) | 16.44 (5.92) | 10.46 (6.10) | 28.76 (17.7) |
| GCS | 14.46 (2.34) | 14 (1.45) | 14.38 (2.3) | 4.69 (3.17) |
Comparison of Acute Physiology and Chronic Health Evaluation II and Glasgow Coma Scale Scores on Admission and Intensive Care Unit Discharge a
5. Discussion
This study investigated various variables of patients with COVID-19 who have been hospitalized in the ICU of Valiasr Hospital since 2020. Among 111 patients, 53.2% died, and 46.8% were discharged safely. The numbers of nonsurvivors in the age groups of ≥ 75 and ≤ 44 years were the highest and lowest, respectively. Moreover, there was a higher mortality rate in the older age groups. In previous studies, old age has been reported as an important independent predictor of mortality in severe acute respiratory syndrome (SARS) and MERS (15, 16). The mean age of the present study sample was 65.15 years; nevertheless, in a study performed on 164 patients admitted to the ICU of several medical centers in Mexico, the mean age of patients was 57.3 years, which was lower than the average age of the current study patients. Additionally, 69.5% of patients in the aforementioned study were male (17).
Out of 111 patients, 46 and 54% were female and male, respectively. Furthermore, 52.9% of women and 54.2% of men died. There was no significant relationship between gender and mortality variables that is inconsistent with the findings of Jin et al.’s study, in which male subjects had a higher than three times mortality rate, compared to female cases (18). The findings of the present study showed that hypertension (49.5%), diabetes (41.4%), heart disease (31.5%), COPD (17.1%), and hyperlipidemia (20.7%) had the highest prevalence of comorbidities in COVID-19 patients. The present study results are not consistent with the findings of Alamdari et al.’s study performed on 459 COVID-19 patients admitted to Shahid Modarres Hospital in Tehran, Iran, whose diabetes was significantly associated with COVID-19 mortality (19). In addition, in a study involving 140 patients admitted to Wuhan Hospital in China, no significant difference was observed in the proportion of patients with hypertension, diabetes, and coronary heart disease between severe and nonsevere patients (20).
Previous studies evaluating the mortality rates of MERS, SARS, and most recently COVID-19 have shown no signs of immunodeficiency as a risk factor for death. Furthermore, there is no history of higher mortalities related to chemotherapy, transplantation, or other disorders that require immunosuppression at any age (21, 22), which is similar to the present study findings. Moreover, a history of influenza vaccination had no significant effect on mortality (23) that is consistent with the results of the present study.
The most commonly reported clinical symptoms were dyspnea (81.1%), fever and chills (73%), cough (64.9%), muscle pain (45%), weakness and lethargy (42.3%), anorexia (36%), and headache (25.2%). Yang et al. observed that dyspnea was more common in ICU patients, similar to the current study results (12). Contrary to the findings of the present study, muscle pain was not common in patients with COVID-19 and was reported in only two clinical trials. Muscle pain was observed in 11% of the 99 COVID-19 patients admitted to Wuhan Jinyintan Hospital in China (11) and 14% of the 28 confirmed COVID-19 cases in South Korea (23). Zhang et al. showed that dyspnea (29%) is the least common symptom in COVID-19 patients (22). Based on the results of the current study, it was concluded that the patients did not refer to the hospital in the early stages of the disease, compared to the Chinese patients.
Among the radiological findings, only bronchoalveolar markings in CXR and pleural effusion in HRCT were significant between the two groups of survivors and nonsurvivors, which is inconsistent with the results of a study by Zhou et al. They observed that consolidation and ground-glass opacity were significantly different between the two groups (11).
The mean values of APACHE scores among survivors at the time of ICU admission and discharge were 12.6 and 10.46, respectively. Moreover, the mean values of APACHE scores in nonsurvivors at the time of ICU admission and discharge were 16.44 and 28.7, respectively. Additionally, the GCS scores at the time of admission and discharge were 14.4 and 14.3 in survivors and 14 and 4 in nonsurvivors. Yang et al. showed an APACHE II score of 17 in nonsurvivors similar to that of the present study (12). Contrary to the findings of the current study, Halim et al. demonstrated an APACHE II score of 22 for nonsurvivors (24). The APACHE II score was significantly increased in the group of patients who died. In a study conducted by Rahimzadeh et al. in Tehran (1986), it was shown that the mortality rate highly met the standards in the APACHE II scores less than or equal to 15; however, in scores above 16, the mortality rate was significantly higher than expected (25). Studies by Hosseini and Ramezani conducted in Bojnourd, Iran, (1991) and Zimmerman et al. (2013) showed that APACHE II is a suitable criterion for predicting mortality. Patients who are more severe and have a higher APACHE II score need longer hospitalization (26, 27).
Except for heart rate, there was a significant difference in vital signs between the two groups of patients; nevertheless, Zhang et al. showed the heart rates of the two groups were different, although their findings of other vital signs are similar to those of the present study (22). In the current study, in the group of survivors, 52 patients needed to use supportive oxygen therapy methods (P < 0.001), which is almost similar to those of Yang et al.’s (94%) and Li et al.’s (100%) studies (12, 28). Naved et al. in Pakistan in 2011 and Bahtouee et al. in 2012 showed a relationship between the duration of hospital stay and mortality (29, 30). Nonetheless, the present study obtained no significant data regarding ICU stay in two groups, contrary to the results of Halim et al.’s study reporting 11 days in the nonsurvived group (24).
5.1. Conclusions
The most common clinical symptoms of COVID-19 were dyspnea, fever and chills, cough, muscle pain, weakness and lethargy, anorexia, and headache in patients at the time of admission. Some variables might increase the risk of poor clinical outcomes, such as older age, comorbidities, bronchoalveolar markings, pleural effusion on HRCT, higher RR ≥ 26 breaths/minute, and APACHE II score ≥ 16. The aforementioned risk factors can help detect ill patients with a poor prognosis at the beginning of ICU admission.
