


1. Background
The COVID-19 pandemic has had a profound effect on individuals’ mental health worldwide as it has increased the prevalence of anxiety and depression (1). The prevalence of mental disorders and sleep problems is several times higher during the COVID-19 pandemic compared to the previously reported statistics (2). Numerous cross-sectional studies worldwide have confirmed the negative impact of COVID-19 on individuals’ mental health. However, few studies have examined the risk factors for the pandemic and their impacts on mental health (3).
Since the trend and prognosis of this disease are unknown in different individuals, and there is not enough information about the nature of the disease, similar to other life-threatening diseases decreasing life expectancy, it may have significant psychological side-effects such as fear of death, anxiety, depression, and stress on the infected individuals and influence the course of recovery (4). According to Lai et al. (5), depression, anxiety, insomnia, and distress are psychological issues involved in the COVID-19 disease. Qiu et al. (6) found out that mental health problems such as panic, anxiety, depression, fear, denial, and despair are the most fundamental traumatic psychological reactions in most affected individuals and those exposed to the disease outbreak. In general, a disease epidemic can significantly lead to increased worry and anxiety and even severe mental illnesses in individuals (7). Although researchers have spared their efforts to compete for the production of the COVID-19 vaccine, since this does not work fast enough to control the epidemic, mass communication restrictions (extensive restrictions) and infection prevention strategies (e.g., travel restrictions, quarantine, and self-quarantine) have been adopted to prevent the spread of the virus (8).
In general, the spread of infectious diseases can lead to increased anxiety, and this anxiety, in turn, has unpleasant effects on individuals’ mental states (9). Anxiety is one of the most common mental disorders, leading to a widespread, unpleasant, and ambiguous feeling of fear and stress of unknown origin and physiological arousal (10). The COVID-19-induced anxiety stems from infection by the coronavirus, mainly because it is unknown and creates cognitive ambiguity (11). Due to the novelty of the COVID-19 disease, little research has addressed the disease anxiety and its treatment options. Previous research on treatments using psychotherapeutic approaches have indicated that they were more effective in treating depressive symptoms than anxiety. The most common and practical strategies were exercise, concentration, and breathing exercises. Using mindfulness and finding it helpful were also associated with lower depression and anxiety symptoms. No other strategy was associated with improved mental health. Individuals’ prior knowledge of psychotherapy strategies may play a role in mental health management in unprecedented public health events such as the global pandemic. The widespread promotion of these techniques in the community to manage general distress in such situations may also contribute (12). The simultaneous provision of treatment and psychological support may reduce the burden of mental illnesses and improve individuals’ health.
This article used the paradoxical psychotherapy (PT) model to treat COVID-19 anxiety. The PT model, called “Paradox + Timetable = Cure (PTC)," as a treatment method for psychological disorders, has overcome many limitations and shortcomings of other methods. The PTC treatment is a systemic-behavioral model with two fundamental components. The first component, “paradox," refers to prescribing a behavioral symptom or disorder. According to this model, clients must reconstruct behavioral and disorder symptoms. In other words, they must reconstruct the same behaviors and symptoms they suffer. The second component, “timetable," is a task, according to which the client is supposed to reconstruct and experience the same symptom or behavior prescribed in the form of paradox at a specific time for a certain period. The combinations of these two therapeutic techniques forms a paradoxical timetable. The paradoxical timetable creates therapeutic changes based on four mechanisms. The first mechanism is grammaticality or artificiality, in which an individual activates and experiences symptoms when he/she desires.
The second mechanism is formed when a patient experiences artificial symptoms as such, it is the disconnection of the relationship between symptoms and anxiety. When the disorder symptoms are artificially reconstructed and experienced, the individual is exposed to a new phenomenon and experience. Symptoms may still be present; however, they contain no bitter taste of anxiety. When a behavior or a symptom is without anxiety, it will no longer be pathogenic as such the relationship between symptoms and anxiety is disconnected. The underlying principle of this treatment is to eliminate anxiety. The third mechanism is to change the symptom’s meaning. When a client reconstructs his/her symptom, the symptoms’ meanings change for him/her and his/her surrounding system (i.e., family members) as such the client is supposed to experience them voluntarily. The fourth mechanism is the “ego” strength. According to the psychoanalytic model, when the relationship between symptoms and anxiety is disconnected, the “ego” can become powerful once more. The strength and weakness of the “ego," which differ in each person and are functions of their past experiences and individual differences, are considered the main factors affecting the speed and slowness of realizing such power (13). This method has been effective in treating a large number of psychological disorders (American Psychiatric Association (2013), including a wide range of anxiety disorders, obsessive-compulsive disorder and relevant disorders, trauma- and stress-related disorders, and physical symptom disorders (13). Accordingly, given the effectiveness of this treatment model in treating anxiety disorders, its role in decreasing the level of COVID-19 anxiety may be significant. The present study was to detect whether paradox therapy can be used as an effective psychotherapy method to reduce and treat anxiety in patients with COVID-19 anxiety.
2. Methods
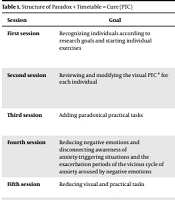
This study aimed to evaluate the effectiveness of paradox therapy in treating COVID-19 anxiety. This quasi-experimental research design used pretest-posttest with a control group and follow-up. The research population encompassed all individuals willing to participate in the present study who were residing in Jahrom during 2020 - 2021. To this end, a call for participation in an intervention study on COVID-19 anxiety was first published via social networks, and the applicants were assessed using the COVID-19 anxiety questionnaire. Then 30 participants with high levels of COVID-19 anxiety were selected using the convenience sampling method and were randomly assigned to experimental (n = 15) and control (n = 15) groups. Considering Cohen’s table with an effect size of 0.5 and a test power of 0.75, the sample size was estimated to be15 persons per group. In the preliminary assessment, the participants received some explanations on the research design, and they were examined regarding inclusion criteria. The inclusion criteria were being aged above 20 years, holding a diploma and having higher education, being motivated and satisfied to take part in intervention sessions, and not suffering from comorbid psychological disorders associated with COVID-19 anxiety. As presented in Table 1, the experimental group received eight sessions of paradox therapy intervention, and the control group remained on the waiting list. Due to the following readons Friedman’s non-parametric test was used to examine the two groups: The significance level of the Kolmogorov-Smirnov test (the data normality prerequisite) in the two groups regarding the difference between the posttest of physical anxiety (P = 0.001) and the follow-up physical symptoms of the COVID-19 anxiety (P = 0.001) was P < 0.05; no normal distribution of the collected data; the significance level of the Leven test (non-observance of homogeneity of variances) in the follow-up phase of COVID-19 anxiety (P = 0.018) and its psychological symptoms (P = 0.034) and the follow-up physical symptoms of the COVID-19 anxiety (P = 0.026); and the non-establishment of regression slope default in the COVID-19 anxiety index and its physical symptoms. Friedman’s statistical test was used to evaluate the effectiveness of paradox therapy in reducing the COVID-19 anxiety and its physical and psychological symptoms. SPSS software version 21 was used in this study to analyze the collected data. This study was extracted from a master’s thesis approved by the Ethics Committee in Biomedical Research at the Payame Noor University (Code: IR.PNU.REC.1400.085).
2.1. Data Collection Tools
2.1.1. COVID-19 Anxiety Scale
This questionnaire was developed by Alipour et al. to determine the level of COVID-19 anxiety in a clinical sample. It consists of 18 items and two psychological and physical factors and provides a total score (11). Items 1-9 address the psychological subscale, and Items 10-18 deal with the physical subscale. The scale is scored based on a four-point Likert scale ranging from 0 to 3. Moreover, the minimum and maximum score of this questionnaire are0 and 54, respectively, with scores 0 - 18 indicating mild anxiety, 19 - 36 indicating moderate anxiety, and 37 - 54 indicating severe anxiety requiring intervention. The scores of psychological and physical symptoms ranged from 0 to 27, depending on the number of items per factor. Cronbach’s alpha coefficients determined the reliability of the first factor (a = 0.879), the second factor (a = 0.861), and the total questionnaire (a = 0.919). To evaluate the criterion validity of this questionnaire, its correlation of this tool with the General Health Questionnaire-28 (GHQ-28) was estimated. The results showed that the reliability of the COVID-19 Anxiety Scale with the total score of the GHQ-28 and the components of anxiety, physical symptoms, social dysfunction, and depression were 0.483, 0.507, 0.418, 0.333, and 0.269, respectively. In this regard, the coefficients were significant at P = 0.01 (11).
2.1.2. Intervention
This protocol was performed in the experimental group in 8 two-hour sessions once a week. The pretest was performed before implementing the protocol, and the posttest was performed after the full implementation of the treatment protocol. The follow-up test was run two months later to evaluate the treatment stability.
| Session | Goal | Content | Tasks |
|---|---|---|---|
| First session | Recognizing individuals according to research goals and starting individual exercises | 1- Performing a pretest; 2- Defining COVID-19 anxiety; 3- Defining and expressing the concepts of cognition, behavior, and the feeling of COVID-19 anxiety by examples; 4- Presenting the treatment goal | Presenting a paradoxical visual program |
| Second session | Reviewing and modifying the visual PTC a for each individual | Adjusting the visual PTC by increasing or decreasing the symptom prescription at times allocated to each person according to the strength and weakness of his/her emotions | Continuing paradoxical visual tasks |
| Third session | Adding paradoxical practical tasks | Investigating individuals’ anxious behaviors, adding a practical PTC to visual exercises at specific times | Performing visual tasks along with practical tasks |
| Fourth session | Reducing negative emotions and disconnecting awareness of anxiety-triggering situations and the exacerbation periods of the vicious cycle of anxiety aroused by negative emotions | Checking tasks and modifying them, increasing or decreasing the tasks if necessary (according to each person’s progress) | Continuing in-person visual and practical programs |
| Fifth session | Reducing visual and practical tasks | Modifying visual and practical tasks and reducing them to twice a day | Continuing in-person visual and practical program |
| Sixth session | Ensuring the reduction of negative emotions and disconnecting the awareness of anxiety-triggering situations and the exacerbation periods of anxiety symptoms | Examining individuals’ tasks and performance and reducing the visual and practical program to once a day | Continuing in-person visual and practical program |
| Seventh session | Evaluating therapeutic exercises and each person’s progress in paradoxical visual and practical exercises | Evaluating individuals’ performance during treatment and reducing visual and practical tasks to every other day | continuing in-person visual and practical program |
| Eighth session | Evaluating individuals’ feedback regarding treatment and treatment completion and providing necessary recommendations | Receiving feedback from the participants about the treatment plan |
Structure of Paradox + Timetable = Cure (PTC)
3. Results
The experimental and control groups' age mean and standard deviation were 27.60 ± 8.83 and 31.07 ± 9.28, respectively. The chi-square test revealed no significant difference between the experimental and control groups in terms of gender (P = 1.00), marital status (P = 0.713), employment status (P = 0.116), and level of education (P = 0.079). Table 2 presents the other demographic features of the participants. Table 3 shows the effectiveness of PTC in the experimental group in the posttest and follow-up stages and reduced COVID-19 anxiety (P = 0.001). In Table 4, PTC was effective in the experimental group in the posttest and follow-up phases (P = 0.001) and reduced physical symptoms caused by the COVID-19 anxiety. As presented in Table 5, PTC was effective in the experimental group in the posttest and follow-up phases and reduced psychological symptoms caused by the COVID-19 anxiety (P = 0.001).
| Groups | Control (n = 15) | Experiment (n = 15) | P-Value (Chi-Square) |
|---|---|---|---|
| Gender | 1.00 | ||
| Female | 14 (93.3) | 14 (93.3) | |
| Male | 1 (6.7) | 1 (6.7) | |
| Marital status | 0.713 | ||
| Single | 7 (46.7) | 6 (40.0) | |
| Married | 8 (53.3) | 9 (60.0) | |
| Employment | 0.116 | ||
| Student | 10 (66.7) | 4 (26.7) | |
| Housewife | 1 (6.7) | 5 (33.3) | |
| Self-employment | 2 (13.3) | 2 (13.3) | |
| Employee | 2 (13.3) | 4 (26.7) | |
| Level of education | 0.079 | ||
| Diploma | 2 (13.3) | 4 (26.7) | |
| Associate | 9 (60.0) | 3 (20.0) | |
| Bachelor | 2 (13.3) | 7 (46.7) | |
| Master and higher education | 2 (13.3) | 1 (6.7) |
Frequency Distribution of Demographic Variables
| Group | Time | Friedman’s Test | ||
|---|---|---|---|---|
| Before Median (Q1 - Q3) | After Median (Q1 - Q3) | Two-month follow-up Median (Q1 - Q3) | ||
| Experimental | 28 (21 - 32) | 3 (1 - 8) | 2 (0 - 7) | 0.001 |
| Control | 25 (14 - 32) | 14 (9 - 18) | 14 (6 - 18) | 0.796 |
| Mann-Whitney U test | 0.430 | 0.001 | 0.001 | |
Score Comparison of COVID-19 Anxiety Before, After, and in Two-Month Follow-up Between Experimental and Control Groups
| Group | Time | Friedman’s Test | ||
|---|---|---|---|---|
| Before Median (Q1 - Q3) | After Median (Q1 - Q3) | Two-month follow-up Median (Q1 - Q3) | ||
| Experimental | 10 (7 - 12) | 0 (0 - 1) | 0 (0 - 1) | 0.002 |
| Control | 7 (1 - 13) | 4 (2 - 4) | 2 (1 - 4) | 0.285 |
| Mann-Whitney U test | 0.189 | 0.001 | 0.002 | |
Score Comparison of Physical Symptoms of COVID-19 Anxiety Before, After, and in Two-Month Follow-up Between Experimental and Control Groups
| Group | Time | Friedman’s Test | ||
|---|---|---|---|---|
| Before Median (Q1 - Q3) | After Median (Q1 - Q3) | Two-month follow-up Median (Q1 - Q3) | ||
| Experimental | 18 (15 - 23) | 3 (1 - 7) | 2 (0 - 7) | 0.001 |
| Control | 18 (12 - 22) | 11 (9 - 14) | 10 (5 - 14) | 0.439 |
| Mann-Whitney U test | 0.708 | 0.001 | 0.001 | |
Score Comparison of Psychological Symptoms of COVID-19 Anxiety Before, After, and in Two-Month Follow-up Between Experimental and Control Groups
4. Discussion
The findings of this study showed that paradox therapy effectively reduced the COVID-19 anxiety in individuals suffering from this type of anxiety. According to Table 3, the PTC treatment was effective in the experimental group in the posttest and follow-up phases and reduced the COVID-19 anxiety (P = 0.001). This finding implies the effectiveness of PTC in reducing anxiety in individuals with this type of anxiety. The present findings are in line with some other studies (13-17) regarding the effectiveness of paradox therapy in reducing the physical symptoms of anxiety.
Some studies examining the effectiveness of PTC in reducing anxiety symptoms compared to pharmacotherapy and cognitive-behavioral therapy indicate that the clinical significance and improvement percentage of the PTC treatment are higher than other therapies and that the PTC treatment is an appropriate and quick way to reduce anxiety symptoms (14, 16, 18). In their research, Besharat and Naghipour (14) examined the effect of the PTC model on an individual with anxiety disorder. Their study showed the effectiveness of this psychotherapy model and its acceptable stability after a 28-month follow-up period. In another study, Besharat (18) also examined the effect of the PTC model on an individual with social anxiety disorder. The results of the three-session treatment and the three-years follow-up period indicated satisfactory changes as well as the stability and continuity of the treatment. In general, studies have confirmed the PTC model as a practical, short-term, and economical method in treating psychological disorders, including anxiety disorders, with the slightest likelihood of disease recurrence in mental disorders (13).
The PTC model was used due to its shorter treatment duration compared to long-term treatments making individuals abandon it half-finished. This model plays a critical role in treating individuals highly resistant to treatment as it is based on symptom prescription. In this model, the therapist’s instructions and prescribed tasks are all functions of the principles minimizing the anxiety of performing tasks and maximizing the patient’s potentials to obey. The model principles, including inseparability of paradox from PTC, prescription of the same disease symptoms, the delayed execution of tasks, and the exclusive reliance on practical treatment techniques, pave the way for a practical, emotional experience and consequently the realization of therapeutic changes as quickly and efficiently as possible. The ultimate goal of this fast and highly short-term treatment is to make some changes in the “ego” level and in its relation and distance to the “id” and the "super-ego," thereby leading to the “ego” strength (i.e., a degree of strength predicting the stability of treatment changes and the sharp decline in the recurrence of symptoms) (19).
According to the findings, paradox therapy effectively reduces the physical symptoms of COVID-19 anxiety in individuals suffering from this type of anxiety. The findings in Table 4 indicate that the PTC treatment was effective in the experimental group in the posttest and follow-up phases (P = 0.002) and reduced the physical symptoms of the COVID-19 anxiety. This concept indicates the effectiveness of PTC in reducing the physical symptoms of COVID-19 anxiety. The present findings are in line with some other studies (13-17) regarding the effectiveness of paradox therapy in reducing the physical symptoms of anxiety.
Coronavirus research has indicated that anxious individuals afraid of COVID-19 experience a coherent set of unpleasant and physiological symptoms aroused by thoughts or information about this infectious disease (20, 21).
Excess COVID-19 anxiety may be a unique type of health anxiety, one of the unique symptoms of which is the fear of infection by COVID-19. According to previous studies on the COVID-19, anxiety, disgust, intolerance of hesitation, anxiety sensitivity, and fear of physical arousal are the predictors of excess anxiety triggered by COVID-19 (22, 23).
One type of anxiety is disease-related anxiety. In particular, infectious diseases often trigger extreme fear and anxiety, thereby leading to many widespread disturbances in behavior and psychological well-being in society (24).
The PTC model is one of the effective models in treating psychological disorders such as anxiety (14, 16, 18). The model had remarkable features in terms of its therapeutic goals. The elimination of symptoms and coercive and imposed behaviors in individuals significantly contribute to the concerned treatment. The PTC model has been used to eliminate such symptoms. In this technique, individuals voluntarily face some of their symptoms (i.e., physical symptoms associated with the COVID-19 anxiety, including palpitations, headaches, tremors, fatigue and lethargy, and nightmares) and utilize complete reconstruction to make the symptoms and the experiences of those compulsive symptoms totally optional. Accordingly, any optional symptom or behavior is no longer a disease, a problem, or a problematic issue.
According to the results, paradox therapy effectively reduces the psychological symptoms of COVID-19 anxiety in individuals suffering from this type of anxiety. Table 5 indicates that the PTC treatment in the experimental group was effective in the posttest and follow-up phases and reduced the psychological symptoms of the COVID-19 anxiety (P = 0.001). This finding indicates the effectiveness of the PTC treatment in reducing the psychological symptoms of the COVID-19 anxiety. The present findings are consistent with those in previous studies on the effectiveness of paradox therapy in reducing psychological symptoms of anxiety (14, 15, 17, 18).
Psychological factors play a vital role in how individuals deal with the threat of an epidemic infection and its consequences (e.g., the loss of a loved one). Although many individuals cope well with the threat of an epidemic, many others experience high levels of anxiety or further mental health problems such as anxiety disorders and other clinical conditions (25).
The main problem with anxious individuals is that they fill their minds with worrying illusions, thereby increasing their anxiety. Anxiety minimizes or sometimes completely destroys an individual’s power (26) and affects his/her psychological well-being. Moreover, lack of scientific information also exacerbates such anxiety. In some cases, individuals look for more information to relieve their anxiety. Anxiety can make individuals misdiagnose true and false information as such, they may be exposed to false news (11), thereby increasing the level of their anxiety induced by a new infectious disease.
The presence of disease anxiety in the community, especially in families at risk of disease (due to living with a sick person or a person having more contact with COVID-19 patients), indicates the need to use a therapeutic intervention. As an alternative treatment to prevent responses, PTC can eliminate maladaptive thinking strategies about anxiety. Paradox therapy is one of Frankel’s semantic therapy methods, which is used to help an individual realize that he/she does not look like his/her perceptual symptoms. Paradoxically, thoughts and feelings are typically designed to over-stimulate the way of thinking about fear or unwanted behavior (27).
One of the goals of the PTC method was to eliminate all negative emotions arising from anxiety and its psychological symptoms. In the paradox therapy exercises, individuals are asked not to control their thoughts, including those about one’s death and their loved ones, fear of hospitalization, fear of infection with COVID-19 as well as relevant practices such as hand washing and disinfection of one’s hands and stuff. This is because one of the therapeutic goals is to communicate with thoughts to prevent resistance or complex perceptual analysis to eliminate maladaptive thinking strategies about being worry and having inflexible control over threats (13). This awareness arouses when the psychological pressures imposed by controlling and blaming thoughts associated with washing and disinfecting hands and equipment and negative feelings about illness and death are eliminated. This implies that when the psychological stress of negative emotions is high, individuals having difficulty in regulating their emotions are inclined to rumination and anger posed by the condition to moderate their mental energy. By relieving COVID-19 anxiety and disconnecting thoughts and their behavioral cycles, this type of therapy makes individuals regulate their emotions better by reinforcing their “ego” and promoting awareness.
4.1. Limitations
Regarding the limitations of the present study, several points need to be mentioned. Diagnosing COVID-19 anxiety was exclusively limited to a questionnaire as such this study can also encompass the limitations mentioned for the questionnaires. This research was conducted in Jahrom, and necessary precautions should be taken in generalizing the findings. The lack of research on physical and psychological indicators in COVID-19 patients, small sample size, and the impossibility of holding in-person meetings were the other limitations of the present study.
4.2. Conclusions
According to the findings, paradox therapy can be used as an appropriate model to treat COVID-19 anxiety and its physical and psychological symptoms in patients.
