1. Background
Stroke is among the leading cause of morbidity and mortality internationally (1). It occurs as a result of either occlusion or rupture of arterial blood supply to the brain (2), resulting in neurological impairments in which type and severity depend on the extent of the injury and the area of the brain affected (3). After stroke, sensory, motor, and cognitive impairments are common neurological issues (4). Depending on the severity of the impairment, stroke survivors need support in performing activities of daily living (ADLs) and community participation (5). It has been documented that about 87% of stroke survivors are usually dependent on family or caregivers to carry out their ADLs (6).
A caregiver is a person who cares for the sick or disabled (7). Depending on the severity of the condition, caregiving of stroke survivors requires significant effort over a prolonged period of time (8). The caregiving may include offering complete or partial assistance in carrying out common daily tasks such as transfer from bed to wheelchair, feeding, hygiene, and toileting among others (6). Provision of caregiving activities for a long period of time may negatively impact the caregivers economically, ranging from loss of hours of work to complete loss of jobs (9). Other effects of prolonged caregiving may include musculoskeletal disorders and mental health problems (10). Caregivers of stroke survivors are at great risk of developing musculoskeletal pain (MSP) such as low back pain (LBP) (11, 12), with female caregivers being more likely to be affected than their male counterparts (9, 12). Moreover, it is expected that adult caregivers may present with MSP rather than adolescent caregivers, given that MSP such as LBP is highly prevalent among adults (13).
In developing countries like Nigeria, there is increasing prevalence of stroke (14, 15). This increase will lead to a substantial economic burden, which is progressive in terms of the cost of physiotherapy and other medical care (16). Therefore, caregivers play a significant role in managing stroke survivors (11, 12). According to the report by Rahman et al. (17), about 44.1% of caregivers always faced awkward posture, whereas 41.5% faced constant repetitive hand movement during manual handling, and blamed awkward posture and constant repetitive hand movements for being the key problems experienced by the caregivers. Consequently, caregivers may experience high levels of physical and psychological stress, which may lead to exhaustion (18, 19). Thus, there is a likelihood of increased reports of MSP by caregivers of stroke survivors (12).
A previous study among ninety stroke caregivers in northeastern Nigeria showed that the prevalence of musculoskeletal symptoms was as high as 82.2%, with LBP being the most common symptom (12). However, studies using a large sample size with power calculation to allow extrapolation of findings are limited. Moreover, due to cultural and environmental differences, affectation and pattern of MSP might likely vary even within the same nation.
2. Objectives
This study aimed to determine the prevalence and pattern of MSP and associated factors among informal caregivers of stroke survivors in northwestern Nigeria.
3. Methods
3.1. Study Design
This was a hospital-based cross-sectional study of informal caregivers of stroke survivors in Kano State, northwestern Nigeria.
3.2. Participants
The participants were informal caregivers of stroke survivors attending out-patient physiotherapy clinics of Aminu Kano Teaching Hospital (AKTH), Murtala Muhammad Specialist Hospital (MMSH), and Muhammadu Abdullahi Wase Teaching Hospital (MAWTH) between February and August 2019. They were recruited consecutively and included in the study if they were 18 - 60 years old and provided care for at least one week. Stroke survivors who suffered from stroke for at least one month and were discharged from the hospital were eligible to participate in the study. Informal caregivers who had a history of musculoskeletal pain/disorder prior to caring for stroke survivors were excluded. A signed informed consent form was obtained from all eligible participants (both informal caregivers and their stroke survivors) after explaining the purpose and procedure of the study. We defined an informal caregiver as an unpaid person who is most closely involved in providing care and assistance to stroke patients (9).
3.3. Sample Size Estimation
The sample size required for this study was calculated using the Cochran’s formula (20);
where N = required sample size; Z = confidence level = 1.96; P = population proportion; d = marginal errors = 5%. Using an estimated population proportion of 82.8% (caregivers with MSP) from a previous similar study (11), the total sample size required for present study was estimated to be 218.
3.4. Data Collection Procedure
Sociodemographic characteristics of caregivers (e.g., age, gender, height, weight, body mass index [BMI], tribe, marital status, educational level, and occupational status), as well as information regarding nature of caregiving and duration of caregiving were obtained using a researcher-designed datasheets. Corresponding stroke survivors’ data, specifically, age, gender, age, post-stroke duration, and side of affectation were also recorded on the datasheets. These data were obtained using self-report from the caregivers and care recipients as appropriate during their visit to physiotherapy for treatment.
Data on MSP prevalence and pattern of prevalence by body parts were collected using the standardized Nordic Musculoskeletal Questionnaire (NMQ) (21). The questionnaire is widely used to assess the prevalence of musculoskeletal problems in various body regions among different Nigerian populations (22-26), including physiotherapists and nurses who typically provide care to stroke patients (25, 26). The NMQ has good sensitivity (66 - 92%) and specificity (71 - 88%) as well as acceptable reliability and validity (0 - 20% disagreement for validity tested against clinical history) (27). The NMQ was self-administered to the caregivers, and they were asked to respond to the questions appropriately if they had experienced ache, pain, or discomfort in different parts of the body (i.e., neck, shoulder, elbow, wrist/hand, upper back, low back, hips/thighs/buttocks, knees, and ankle/feet) in the previous 12 months that may be due to caregiving using body map. As described in a previous study (28), the questionnaire was pilot tested among five caregivers recruited conveniently to improve comprehensibility and clarity of the questionnaire items and instructions.
3.5. Statistical Analysis
Descriptive statistics were used to summarize data using mean and standard deviation for continuous data, and frequency and percentage for categorical data. Inferential statistics of chi-square test was used to test the association between perceived factors (age, gender, BMI, marital status, educational level, occupational status, nature of caring, and duration of caring) and the most prevalent MSP. All statistical analyses were conducted using SPSS for Windows (version 23, IBM Corporation, Armonk, NY, USA) at an alpha level of 0.05.
4. Results
4.1. Characteristics of the Informal Caregivers and Stroke Survivors
A total of 218 informal caregivers of stroke survivors, with mean (SD) age of 28.1 (13.7) years, participated in the study. The majority of the caregivers (60.6%) were females within the age range of 18 - 27 years and engaged in full-time caregiving per day (63.8%) (Table 1).
Table 1.
Characteristics of the Informal Caregivers
| Variables | No. (%) |
|---|---|
| Age (y) | |
| 18 - 27 | 111 (50.9) |
| 28 - 37 | 78 (35.8) |
| 38 - 47 | 27 (12.4) |
| 48 - 57 | 2 (0.9) |
| Gender | |
| Male | 86 (39.4) |
| Female | 132 (60.6) |
| BMI | |
| Under weight | 17 (7.8) |
| Normal weight | 122 (55.9) |
| Overweight | 52 (23.8) |
| Obese 1 | 2 (1.0) |
| Obese 2 | 25 (11.5) |
| Tribe | |
| Hausa | 156 (71.6) |
| Fulani | 44 (20.2) |
| Others | 18 (8.3) |
| Marital status | |
| Single | 115 (52.8) |
| Married | 95 (42.7) |
| Divorce | 10 (4.6) |
| Educational level completed | |
| Primary | 17 (7.8) |
| Secondary | 112 (51.4) |
| Tertiary | 89 (40.8) |
| Occupational status | |
| Civil servant | 37 (17.0) |
| Housewife | 83 (38.1) |
| Self-employed | 98 (45.0) |
| Nature of caregiving | |
| Full-time | 139 (63.8) |
| Part-time | 79 (36.2) |
| Duration of caregiving (weeks) | |
| 1 - 26 | 204 (93.6) |
| 27 - 52 | 12 (5.5) |
| 53 - 78 | 1 (0.5) |
| 79 - 104 | 1 (0.5) |
Abbreviation: BMI, body mass index.
The mean (SD) age of the stroke survivors was 46.7 (10.9) years. Most of them (71.1%) were males within the age range of 39 - 53 years and presented with right side affectation (58.7%) (Table 2).
Table 2.
Characteristics of the Stroke Survivors
| Variables | No. (%) |
|---|---|
| Age (y) | |
| 24 - 38 | 13 (6.0) |
| 39 - 53 | 106 (48.6) |
| 54 - 68 | 66 (30.3) |
| 69 - 83 | 33 (15.1) |
| Gender | |
| Male | 155 (71.1) |
| Female | 63 (28.9) |
| Duration of caring (weeks) | |
| 1 - 26 | 196 (89.9) |
| 27 - 52 | 17 (7.8) |
| 53 - 78 | 1 (0.5) |
| 79 - 104 | 4 (1.8) |
| Side of affectation | |
| Right | 128 (58.7) |
| Left | 90 (41.3) |
4.2. Musculoskeletal Pain and Associated Factors Among Informal Caregivers
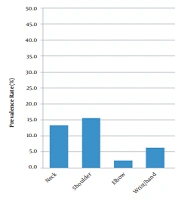
The overall prevalence of MSP among informal caregivers of stroke survivors in the past 12 months of caring was 16.5%. The prevalence of MSP according to the body regions was 13.3%, 15.6%, 2.3%, 7.3%, 6.3%, 28%, 8.3%, 17.4%, and 8.3% in neck, shoulder, elbow, wrist, upper back, low back, hips, knee, and ankle, respectively (Figure 1).

Figure 1.
The prevalence of musculoskeletal pain by body region among informal caregivers of stroke survivors.
Chi-square test showed that there was a statistically significant association between prevalence of most occurring MSP (i.e., LBP) and age (χ2 = 45.506; P < 0.001), gender (χ2 = 27.749; P < 0.001), BMI (χ2 = 41.358; P < 0.001), marital status (χ2 = 47.018; P < 0.001), educational level (χ2 = 8.141; P = 0.017), occupational status (χ2 = 39.492; P < 0.001), duration of caregiving (χ2 = 12.502; P = 0.006), and nature of caregiving (χ2 = 16.920; P < 0.001) (Table 3).
Table 3.
Association Between Prevalence of Low Back Pain Among Informal Caregivers and Their Characteristics
| Variables | No. (%) | χ2 | P-Value |
|---|---|---|---|
| Age (y) | 45.506 | < 0.001* | |
| 18 - 27 | 111 (50.9) | ||
| 28 - 37 | 78 (35.8) | ||
| 38 - 47 | 27 (12.4) | ||
| 48 - 57 | 2 (0.9) | ||
| Gender | 27.749 | < 0.001* | |
| Male | 86 (39.4) | ||
| Female | 132 (60.6) | ||
| BMI | 41.358 | < 0.001* | |
| Underweight | 17 (7.8) | ||
| Normal weight | 122 (55.9) | ||
| Overweight | 52 (23.8) | ||
| Obese 1 | 2 (1.0) | ||
| Obese 2 | 25 (11.5) | ||
| Marital status | 47.018 | < 0.001* | |
| Single | 115 (52.8) | ||
| Married | 95 (42.7) | ||
| Divorce | 10 (4.6) | ||
| Educational level completed | 8.141 | 0.017* | |
| Primary | 17 (7.8) | ||
| Secondary | 112 (51.4) | ||
| Tertiary | 89 (40.8) | ||
| Occupational status | 39.492 | < 0.001* | |
| Civil servant | 37 (17.0) | ||
| Housewife | 83 (38.1) | ||
| Self-employed | 98 (45.0) | ||
| Nature of caregiving | 16.920 | < 0.001* | |
| Full-time | 139 (63.8) | ||
| Part-time | 79 (36.2) | ||
| Duration of caregiving (weeks) | 12.502 | 0.006* | |
| 1 - 26 | 204 (93.6) | ||
| 27 - 52 | 12 (5.5) | ||
| 53 - 78 | 1 (0.5) | ||
| 79 - 104 | 1 (0.5) |
Abbreviations: χ2, chi-square statistics; df, degree of freedom; BMI, body mass index.
5. Discussion
Caregivers of stroke survivors, especially in Africa, experience severe caregiving burden (9), which could be due to MSP. Thus, exploring the prevalence of MSP and underlying factors is of great importance for health professionals and policymakers. This study determined the prevalence of MSP and associated factors among informal caregivers of stroke survivors in northwestern Nigeria.
The results of the present study revealed that the majority of the informal caregivers were females; this is expected considering the number of housewives recruited in the study, and implies that most of the informal caregivers were taking care of their spouses. Our finding is in line with the study of Vincent-Onabajo et al. (12), who showed a higher proportion of female caregivers of Nigerian community-dwelling stroke survivors (61%) compared to their male counterparts (39%). Similarly, Yalcinkaya et al. (11) found caregivers to comprise more females (56%) than males. The present study also revealed that the majority of the informal caregivers were young, within the age range between 18 and 27 years, and engaged in full-time daily care. This is also in agreement with the findings of Vincent-Onabajo et al. (12), who showed a majority of caregivers of stroke are within their youthful age, with a mean age of 33.2 years. In contrast, more elderly caregivers were found in the study by Yalcinkaya et al. (11).
The results of this study showed that the 12-month prevalence of MSP among informal caregivers of stroke survivors was low (17%). This finding is not surprising considering the average duration of onset of the majority of the stroke survivors (1 - 26 weeks or 1 - 5 months) and the corresponding duration of care provided by the caregivers. This indicates that the majority of the informal caregivers in this study offered to care for a relatively shorter period (less than a year). In contrast to our study, higher prevalence rates (82%) were reported in a previous study that utilized a 7-day prevalence period (12). The 12-month prevalence period used in our study may be, however, subject to recall bias considering the longer recall period. Consistent with previous studies (11, 12, 29), the present study revealed that the most commonly reported site of MSP among informal caregivers of stroke survivors was low back, suggesting that low back pain remains the most common and burdensome MSP disorder.
Regarding the association between the most common MSP (i.e. low back pain) and demographic factors, we found a significant association between MSP and age of the caregivers. As the preponderance (51%) of the caregivers in this study were within the age range of 18 - 27 years old, it can be interpreted that young adults are commonly involved in providing caregiving to stroke survivors in northwestern Nigeria. In contrast to our finding, the study of Vincent-Onabajo et al. (12) conducted in northeastern Nigeria revealed no significant association between MSP and age of family caregivers. However, the variation may be due to the difference in the age groups between the two studies. Relatedly, the result of the study showed that there was a significant association between MSP and gender of the caregivers, with females (61%) being more affected, which is analogous to the reports of previous studies (11, 12).
Marital status was found to be associated with MSP, with being single more likely to be implicated. This finding is not surprising as unmarried individuals may have fewer responsibilities and hence, likely to be readily available to provide caregiving, unlike married individuals. Also, educational level and occupational status were found to be significantly associated with MSP. Specifically, having completed secondary school and being self-employed were more likely to be implicated. On the contrary, education level and occupational status were not found to be associated with MSP among family caregivers in northeastern Nigeria (12), which could be attributed to sociodemographic differences.
Similarly, we found a significant association between MSP and adiposity as measured by BMI. Surprisingly, the majority of the informal caregivers in this study had normal BMI (56%) followed by overweight (24%), suggesting that those with normal weight are likely to report more MSP compared to those with under or overweight. It would be, therefore, difficult to relate higher BMI with MSP in this study as generally thought. In contrast to our finding, Rosa et al. (30) found higher BMI to be associated with MSP. Although the relationship between pain and adiposity is not clearly understood, it is believed that excess adipose tissue may increase mechanical load on the musculoskeletal system, thereby resulting in pain.
Findings of the present study revealed a significant association between MSP and the duration of caregiving as well as the nature of caregiving, with 1 - 26 weeks and full-time being reported to be the commonest duration of caregiving and nature of caregiving, respectively. This may suggest that stroke caregiving in this context, even though it is provided on full-time basis, is usually of short time period. Our findings are in agreement with the findings of Habib et al. (31), who showed that full-time caregivers present with MSP more than their part-time counterparts.
The strength of the present study is that the sample size was relatively large and determined a priori compared to previous studies (11, 12). Nonetheless, it should be noted that our study has some limitations, which should be taken into account when interpreting the results. First, the use of a self-report questionnaire to examine the presence of MSP may be subject to recall bias. Second, our population is comprised of more females than males, which may not allow extrapolation of the findings. Finally, regression analysis was not performed to explore how the examined factors predicted MSP. Thus, future similar studies using robust analyses may be useful.
In conclusion, the results of this study suggest that low back pain is the most common occurring MSP among informal caregivers of stroke, which is associated with age, gender, BMI, marital status, education level, occupation status, duration of caregiving, as well as nature of caregiving. It is recommended that health professionals, especially physiotherapists and nurses in northwestern Nigeria, should educate informal caregivers of stroke survivors on proper ergonomics and other MSP preventive strategies.

