1. Background
The well-being and advancement of a community are highly dependent on women, and pregnancy and delivery have a noticeable effect on their health. Hence, maternal and newborn health is one of the priorities of health services. During pregnancy, many biological, chemical, physiological, and anatomical changes happen in women (1). Sleep is an essential and crucial behavior affected by physiological and pathological changes during pregnancy. The quality and quantity of this behavior are changed due to respiratory problems (because of fetus growth and its effects on the diaphragm), nocturia, back pain, and leg cramps. Some physical and emotional factors can disrupt the sleep pattern and cause sleep disorders. Hormonal changes, such as estrogen and progesterone increase and elevated plasma cortisol levels, also lead to sleep pattern changes (2). On the other hand, researchers have reported that sleep disorders have a significant relationship with diseases such as hypertension, cardiovascular diseases, diabetes, and depression (3).
Approximately 30% of people suffer from sleep disorders. It is reported that almost 49% of women suffer from sleep disorders during pregnancy (4). The findings of different researches differ in this regard. One study showed that 75.2% of women in the third trimester, 63% in the second trimester, and 48% in the first trimester suffer from sleep disorders during pregnancy (5). There is also evidence that pregnancy-related complications, such as gestational diabetes (6), pregnancy-induced hypertension (7), fetus growth retardation (8), preterm labor, and stillbirth (9), are related to sleep disorders. Sleep deprivation leads to deleterious neurodevelopment consequences for the newborn and endangers its viability (10). Recently, it has been demonstrated that sleep deprivation is associated with higher diastolic blood pressure and higher BMI in the offspring (11). Researchers have also reported that mood and sleep are interconnected. Moreover, it is observed that women with post-partum depression are more commonly affected by sleep disorders (12). The prevalence of anxiety during pregnancy varies from 2.6 to 39% (13, 14). Antenatal anxiety is prevalent in pregnancy; approximately 23% of pregnant women experience anxiety symptoms during pregnancy. It is noteworthy that antenatal anxiety is approximately 2 - 3 times more prevalent than antenatal depression (15). Anxiety during pregnancy is a risk factor for post-partum depression in the mother and behavioral and emotional changes in the offspring (16). Considering the influence of sleep on health, particularly during pregnancy, on both the offspring and the mother, it is imperative to identify related contributing factors and address them. Thus, detecting and monitoring these factors in this period is important.
2. Objectives
This study aimed to investigate the correlation between sleep quality and mental health among pregnant women.
3. Methods
Study design and setting: This cross-sectional study was conducted in a multi-stage manner from 2018 to 2019 in Babol/ Iran. First, the healthcare centers were randomly selected through coin toss from a list provided by the authorities; then, the participants entered the study by convenience sampling method.
Study participants and sampling: All pregnant women presenting to the healthcare centers who volunteered to participate through signing a written consent form were included in the study.
Inclusion criteria were as follows: basic reading and writing literacy, singleton pregnancy, intentional pregnancy, and filling out and signing the consent form. Pregnant women without any history of infertility, pregnancy complications (asthma, thyroid and kidney disorders, diabetes, preeclampsia, fetus-growth retardations, rupture of the membranes, etc.), accidents during the past year, drugs and alcohol addiction, shift-work jobs, history of psychological disorders, soporific drug use history, antihistamine intake, and excessive consumption of tea, coffee, and herbal medicines. Exclusion criteria were incomplete questionnaires and refusal to participate. The sample size was calculated according to the equation
3.1. Data Collection Tools and Techniques
The participants completed four questionnaires, namely demographic, Beck Depression Inventory (BDI), The State-Trait Anxiety Inventory (STAI), and Pittsburgh sleep questionnaire index (PSQI). The participating pregnant women were divided into two groups according to their PSQI score.
PSQI was developed by Buysse et al. (18) to evaluate sleep quality in adults. This instrument consists of 18 questions, and differentiates good and poor sleep by evaluating 7 sleep components during the past month. This instrument is a self-reporting questionnaire and includes multiple domains (subjective sleep quality, latency, duration, habitual sleep efficiency, disturbances, sleep medication consumption, and Hypersomnia). Most of the questions are in a multiple-choice form, and the scores range from 0 to 3. The total score ranges from 0 to 21. A score of 5 or higher denotes a significant sleep disorder. This questionnaire has been psychometrically tested in Iran (19).
BDI includes 21 multiple-choice questions (with four choices each), and similar to PSQI, the scores range from 0 to 3. A score of 9 and below is considered not depressed, 10 - 12 at risk, and 12 and above are considered depressed. The Persian version of this questionnaire has high internal consistency according to Alpha-Cronbach of 87%, and its reliability has been reported to be 73% (20).
The revised form of STAI includes 40 questions. Items 1 - 20 measure state anxiety (overt) with four options (never, sometimes, usually, and very much), and items 21 - 40 for the trait anxiety with four options (Rarely; sometimes; often; almost always) (21). Panahi Shahri used the test-retest method to calculate Alpha-Cronbach for trait anxiety (92%) and state anxiety (90%) (22).
3.2. Data Analysis
The statistical analysis was performed using SPSS version 22.0 (SPSS Inc., Chicago, IL). Assessment of data normality was performed by the Kolmogorov-Smirnov test. The descriptive statistics were presented as the mean (SD) for quantitative data and the frequency and percentage for categorical data. The data were analyzed using t-test, chi-square, and logistic regression. P < 0.05 was considered statistically significant.
4. Results
The respondents were 600 individuals comprised of 240 (40%) pregnant women with good quality of sleep and 360 (60%) with poor quality of sleep. The average ages of participants in the group with good quality of sleep and those with poor quality of sleep were 26.45 ± 4.32 and 26.36 ± 5.2 years, respectively. Most of the participants were housewives (90.2% and 88.9%) with higher education (97.7% and 98.7%), and most of the spouses had higher education (88.3% and 87.5%), as well. Demographic status (including age, education, employment, and spouse education) displayed no considerable differences between the two groups. The group with good sleep quality had a higher body mass index (BMI) before pregnancy. The number of pregnancies showed a considerable relationship with sleep quality, such that sleep disorder was more prevalent among women with a higher number of pregnancies (Table 1). Gestational age also displayed a significant relationship with sleep quality (Table 2).
Table 1.
Comparison of Demographic Characteristics of Pregnant Women According to Their Sleep Quality a
| Variables | Good Quality of Sleep (N = 360) | Poor Quality of Sleep (N = 240) | P-Value |
|---|---|---|---|
| Age | 0.98 | ||
| ≤ 30 | 287 (79.9) | 192 (80) | |
| < 30 | 72 (20.1) | 48 (20) | |
| Education | 0.36 | ||
| ≤ Diploma | 4 (1.3) | 5 (2.3) | |
| > Diploma | 311 (98.7) | 213 (97.7) | |
| Employment | 0.60 | ||
| Yes | 37 (11.1) | 23 (9.8) | |
| No | 295 (88.9) | 212 (90.2) | |
| Spouse education | 0.78 | ||
| ≤ Diploma | 37 (12.5) | 25 (11.7) | |
| > Diploma | 258 (77.5) | 188 (88.3) | |
| Gravid | 0.002** | ||
| 1 | 239 (64.2) | 133 (35.8) | |
| ≥ 2 | 112 (35.8) | 107 (48.9) | |
| Pre-pregnancy BMI | 0.028* | ||
| Underweight/normal | 163 (50.9) | 83 (41.1) | |
| Overweight/obese | 157 (49.1) | 119 (58.9) |
a Chi-square test, ** P < 0.05, * P < 0.001
Table 2.
Comparison of Sleep Quality in Pregnant Women According to the Gestational Age
| Variables | Good Quality of Sleep (N = 360) | Poor Quality of Sleep (N = 240) | χ2 | df | P-Value |
|---|---|---|---|---|---|
| Gestational age | 15.725 | 2 | < 0.001 a | ||
| 1st trimester | 68 (18.8) | 28 (11.7) | |||
| 2nd trimester | 168 (46.8) | 92 (38.3) | |||
| 3rd trimester | 124 (34.3) | 120 (50) |
a P < 0.001
The present study demonstrated a significant relationship between depression score and sleep quality (r = 0.11, P = 0.008). The average subscale of trait anxiety for women with poor sleep quality was significantly higher than in women with poor sleep quality (Table 3). The results showed a significant correlation between depression scores and sleep subscales. Pearson test, proved that sleep latency (r = 0.33, P < 0.001), disturbances (r = 0.35, P < 0.001) and Hypersomnia (r = 0.24, P < 0.001) display remarkable relationship with depression score. In addition to those, sleep duration (r = 0.15, P < 0.001) and sleep efficiency (r = -0.15, P < 0.001), proved to have an inverse correlation with depression score.
Table 3.
Comparison of Depression and Anxiety in Pregnant Women According to the Sleep Quality a
| Variables | Good Quality of Sleep (N = 360) | Poor Quality of Sleep (N = 240) | t | P-Value |
|---|---|---|---|---|
| Depression | 2.25 ± 3.41 | 4.72 ± 4.93 | 7.149 | < 0.001 b |
| Trait-anxiety | 39.44 ± 9.63 | 41.68 ± 12.68 | -2.420 | 0.016 c |
| State-anxiety | 42.29 ± 11.24 | 42.03 ± 10.49 | 0.285 | 0.776 |
a Values are expressed as mean ± SD.
b P < 0.001
c P < 0.05
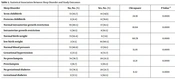
The probability of poor sleep quality was higher in women in their 3rd trimester, overweight women, and those with high anxiety, as demonstrated by the logistic regression analysis results (Table 4).
Table 4.
Crude OR (CI 95%) Association Between Quality of Sleep and GA, BMI, and Severity of Anxiety
| Variables | B | OR (CI 95%) | P-Value |
|---|---|---|---|
| Gestational age | |||
| 1th trimester | -0.678 | 0.50 (0.227 - 10.136) | 0.069 |
| 2nd trimester | -0.715 | 0.489 (0.281 - 0.852) | 0.012 |
| 3rd trimester | Ref. | 0.030 | |
| BMI | 0.0240 | ||
| Underweight/normal | -0.630 | 0.502 (0.297 - 0.920) | |
| Overweight/obese | Ref. | ||
| Severity of anxiety | |||
| Low | 00.847 | (10.27 - 40.26) 20.33 | 00.006 |
| Moderate | 00.113 | (10.70 - 0.735)10.120 | 00.598 |
| Severe | Ref. | 00.012 |
5. Discussion
The current study investigated the correlation between sleep quality and mental health (anxiety and depression) among women. The results demonstrated significant differences between the depression scores of women with good quality of sleep and that of women with poor quality of sleep. In addition, trait anxiety scores were significantly different in the women with good quality of sleep compared to those with poor quality of sleep. Results showed that depression was more prevalent among pregnant women with poor sleep quality.
Rad et al. reported that the risk of depression among women with sleep disorders was twice higher. They also observed significant relationships between delayed sleep phase disorder, early awakening, continuous sleep problems, disruption of daily activities, and depression (23). Asltoghiria concluded that 11.4% of pregnant women without sleep disorders and 56.2% of pregnant women with sleep disorders suffered from depression, and the risk of depression was increased 9-fold among them (24). Field et al. (25) also found that “sleep disorders had a significant relationship with depression during pregnancy; however, contrary to other studies, Kamysheva et al. did not find any relationship between sleep disorders and depression (26). This indicates that the relationship between sleep quality and depression might be complicated beyond the information presented in the literature. Santiago et al. found that the durations of REM and NREM phases of sleep decrease in the last 24 hours of gestation before delivery. This was accompanied by an increase in estrogen and progesterone during this period. This shows that these two hormones influence sleep during pregnancy. The combined effects of these hormones are dependent on their concentrations in blood. In addition, cortisol levels were lower in the patients with depression compared to the control group. Considering the two mentioned reports, a potential role for the pituitary gland in the development of depression may be proposed (27). It might be suggested that sleep quality is related to circadian rhythm, sleep disorders, and melatonin levels, all demonstrated to be involved in mood disorders (28).
Similar to other studies, the current study showed that depression significantly correlated with sleep quality subscales in women with sleep disorders. Many studies have investigated the relationship between sleep disorders and depression in both genders (29). Since postpartum depression and insomnia have a significant relationship, this might indicate a relationship between sleep disorders and depression during pregnancy (30).
The present study demonstrated a significant correlation between anxiety and sleep quality. This finding was similar to the research by Afsah and Astuti, which revealed that anxiety was significantly correlated with sleep quality. They conducted a multivariate analysis on pregnant women. They showed that women with severe anxiety are 15 times more susceptible to poor sleep quality (31). Another study reported a strong relationship between average sleep score and anxiety level, and the relationship between average sleep score and depression was reported as weakly associated. (2). It can be inferred from the existing literature that sleep quality, depression, and anxiety are correlated during pregnancy. However, many complicated and obscure aspects exist regarding the correlation among these factors.
The present study demonstrated that sleep quality deteriorates with increasing gestational age. This is consistent with the results reported by Shojaie et al. (32), Facco et al. (33), and a recent systematic review by Salari et al. (34), which demonstrated that women had sleep disorders and suffered from poor sleep quality in the final months of their pregnancy. This study showed that sleep quality and gestational age are significantly correlated. The results also showed that poor sleep quality is more prevalent among pregnant women during the third trimester. Polo-Kantola et al. (35) noted that women had increased delayed sleep phase disorder since the 20th week. Nonetheless, a study by Taskiran found no relationship between sleep quality and advanced gestational age (36).
In the present study, we have found a correlation between pre-pregnancy BMI and sleep quality. A study in Saudi Arabia reported a similar result, which indicated that people with higher BMI had poor sleep quality (37). Even though obesity is a multi-factorial condition caused by complicated genetic interactions and environmental factors (physical activity, nutrition, caffeine intake, etc.), these factors can per se affect sleep quality (38).
These findings suggest that the screening for sleep disorders and prenatal mental disorders should include not only antenatal depression but also anxiety and other mental problems if possible. This can lead to better prenatal sleep disorder management.
5.1. Limitation and Recommendation
It appears that the relationship between sleep quality and anxiety and depression is too complicated for a cross-sectional study with no follow-up cases to be conclusive. The cross-sectional design without any follow-ups can be considered a limitation of this study. To determine a causal relationship between the variables of this study, we recommend that a comprehensive cohort study commencing from the pre-pregnancy stage is designed and conducted.
5.2. Conclusions
Women with poor sleep quality may have mental health problems. Therefore, screening for mental health by health professionals and referring them to a clinical psychologist can improve their sleep quality. To investigate the causal relationship between the study variables, it is necessary to conduct an extensive cohort study that starts before the pregnancy.