





1. Background
The coronavirus disease 2019 (COVID-19) has become a global public health emergency. The World Health Organization (WHO) reported almost 531 million confirmed cases globally, including seven million cases in Iran as of June 2022 (1). This high incidence rate has caused severe anxiety and feeling of helplessness in communities including healthcare workers (HCWs) (2) who have been in constant exposure to the virus over the past two years. In addition, HCWs are concerned about spreading the virus to their family members and being stigmatized because of their interactions with COVID-19 patients (3). Besides, this psychological distress, COVID-19 has led to increased working hours, increased inpatient demands, and increased patient mortality (2). These developments have collectively made HCWs vulnerable to impaired function (4) and burnout (5). Burnout negatively affects the mental health of HCWs and the quality of their provided services (6). These issues highlight the importance of the early detection of anxiety symptoms among HCWs. However, timely anxiety detection cannot be adequately addressed without utilizing reliable and valid anxiety assessment tools (4).
Our literature review suggests that the existing tools for evaluating anxiety symptoms among Iranian HCWs during the COVID-19 pandemic have some limitations. For example, a recent Iranian study has developed a compound questionnaire about COVID-19-related stress and job burnout among HCWs (5). It used two available questionnaires, the Depression, Anxiety, and Stress Scale-21 (DASS-21) (7) and the Copenhagen Burnout Inventory (CBI) (8, 9). This study has validated these scales among Iranian nurses (5). In contrast, a review study argued that traditional screening tools might lead to underdiagnosis or overdiagnosis of mental health disorders in a newly emerged situation, such as the current pandemic (10). Hence, new instruments may contribute better to epidemiological studies during the pandemic.
Several questionnaires measure COVID-19-related anxiety. Some examples are the COVID-19 Anxiety Syndrome Scale (C-19ASS) (11), the COVID-19 Anxiety Scale (12), the Persian COVID Stress Scale (13), the Coronavirus Disease Anxiety Scale (CDAS) (14), and the Coronavirus Anxiety Scale (CAS) (15). Among these screening tools, we decided to validate the CAS among HCWs in Iran for several reasons. The CAS is a brief questionnaire that includes five items, which assesses and identifies dysfunctional anxiety induced by the current COVID-19 pandemic. This assessment is based on distinct manifestations of anxiety within cognitive, behavioral, emotional, and physiological dimensions (15). The CAS has been validated among different general papulations with different languages including Bengali (16), Portuguese (17, 18), Korean (19), Turkish (20), Polish (21), Spanish (22, 23), Urdu (24), and Persian (25, 26). The last two cases were studies that validated the CAS in two major cities of Iran, including Kermanshah (25) and Tehran (26). Both studies have validated the Persian version of the CAS among the general population. They have pointed out that it is necessary to conduct a similar study among HCWs, who are facing more anxiety. Hence, we found this scale to be useful, functional, and popular. Our objective is to assess the validity and reliability of the Coronavirus Anxiety Scale among Iranian nurses, as a group of healthcare workers.
2. Methods
This cross-sectional study was conducted from January 22, 2021, to March 19, 2021, which is the period between the second and third peaks of COVID-19 in Iran (1). The University Ethics Committee approved the study. The ethical code was IR.MUMS.REC.1399.639. All participants completed informed consent. The authors received translation permission from the author of the original Coronavirus Anxiety Scale article, Dr. Sherman Lee (15). Subsequently, they began the translation and validation of the CAS. Next, they sent the following two online questionnaires to participants: the demographic questionnaire and the CAS. Inclusion criteria for participation in the study were working in the medical and nursing profession at the hospitals affiliated with Mashhad University of Medical Sciences, being within the age range of 18 to 60, and completing the two online questionnaires. Exclusion criteria were having one or more major psychiatric disorders (e.g. major depressive disorder, schizophrenia, and bipolar disorder), leaving more than two questions unanswered, and unwillingness to fill out the consent form. Eligible participants were provided an invitation form through their academic email.
The CAS is a concise mental health-screening questionnaire. It can identify dysfunctional anxiety due to the coronavirus crisis based on cognitive effects (repetitive thoughts and worries), behavioral effects (dysfunction and compulsive behaviors, or avoidance), emotional effects (fear, anxiety, and anger), and physiological effects of anxiety (sleep disorders and physical distress). Answers were measured using the five-point Likert scale (from 0 = never to 4 = almost every day, for the past two weeks). The cut-off score for this scale was ≥ 9, with 90% sensitivity and 85% specificity (15). A recent study lowered the cut-off score from 9 to ≥ 5 for the general population, and ≥ 9 when screening at-risk or anxious groups (27). For validation of the CAS among Iranian HCWs, the authors translated the CAS into Persian using the forward-backward translation method. Initially, an English expert translated it into Persian. Then, two Persian language professors working in the United States back translated it. Next, the authors compared them to the original English version. Ultimately, the Persian translation was modified in the required parts. For assessment of the content validity, six psychiatrists, who had recently served at the COVID-19 wards of public hospitals, evaluated the translated questionnaire. An online questionnaire was sent to all of them. It consisted of questions about relatedness (completely related, related, relatively related, unrelated), transparency (completely transparent, transparent, relatively transparent, not transparent), simplicity (completely simple, simple, relatively simple, non-simple), and necessity (it is necessary, useful but not necessary, not necessary) of each item. In addition, the psychiatrist expressed their opinions to qualify the questionnaire by answering a qualitative question at the end. Accordingly, the evaluation of psychiatrists’ opinions was qualitative and quantitative. Ultimately, they made modifications to the translated content. The content validity was calculated based on the content validity index (CVI) and the content validity ratio (CVR). For evaluating the face validity, 10 medical interns working at the Mashhad University of Medical Sciences reviewed and modified the questionnaire form. Their corrections regarding the language and writing of the items were submitted. For assessing the construct validity, the confirmatory factor analysis (CFA) was used based on the nurses’ responses to the online questionnaire. Finally, Cronbach's alpha coefficient was used to assess the internal consistency, and the test-retest method was used to evaluate the reliability of the questionnaire. To this aim, 30 psychiatric residents filled out the online form of the questionnaire twice within two weeks.
2.1. Statistical Analysis
Statistical analysis was conducted using AMOS 23.0 and IBM SPSS 16.0. A P-value of less than 0.05 was considered significant. The required sample size for CFA is 10 samples for each item (28, 29).
3. Results
Based on the inclusion criteria, 250 nurses participated. In the assessment of their answers to the questionnaire, 65 participants were excluded (20 people had completed the questionnaire twice, and 45 people had left many questions unanswered). Therefore, 185 participants were included (Table 1). In correlating the total CAS score with demographic variables, the mean total CAS score was 2.3 (SD = 3.3) in the target sample, 1.86 (SD = 3.03) in men, and 2.4 (SD = 3.4) in women, ranging from 0 to 18. There was no significant relationship between gender and the total CAS score (P = 0.32). However, the CAS score in participants aged 30 to 40 years was significantly higher than the score for other participants (P = 0.022). There was no significant difference between the CAS scores between married and single participants (P = 0.872).
| Variables | Frequency (%) | Mean |
|---|---|---|
| Age | ||
| 20 to 30 | 32 (17.3) | |
| 30 to 40 | 96 (51.9) | |
| 40 to 50 | 53 (28.6) | |
| 50 to 60 | 4 (2.2) | |
| Total | 185 (100) | 36.05 |
| Gender | ||
| Female | 143 (77.3) | |
| Male | 42 (22.7) | |
| Total | 185 (100) | |
| Marriage | ||
| Yes | 153 (82.7) | |
| No | 32 (17.3) | |
| Total | 185 (100) |
Descriptive Statistics Analysis
3.1. Content Validity
The answers of six psychiatrists to the online questionnaire based on the Likert scale were statistically analyzed, using the CVI and CVR. The item “When I thought about the coronavirus or was exposed to information about it, I felt paralyzed,” in terms of relevancy, transparency, and simplicity, received the lowest score, which was 0.83; however, according to the cut-off point of 0.79, this item was also confirmed.
3.2. Construct Validity
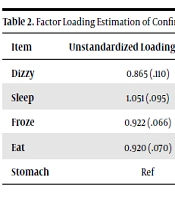
The CFA of answers indicated that the CAS with a one-factor structure fitted the data well (Figure 1 and Table 2), and the standardized factor loading values were greater than 0.4, which was within an acceptable range (30). The results of the goodness of fit index of the model are presented in Table 3.
| Item | Unstandardized Loading Factor (S.E.) | Statistic (P-value) | Standardized Loading Factor | Acceptable Range (Threshold) | Result |
|---|---|---|---|---|---|
| Dizzy | 0.865 (.110) | 7.861 (< 0.001) | 0.602 | Above 0.4 | Acceptable |
| Sleep | 1.051 (.095) | 11.113 (< 0.001) | 0.743 | Above 0.4 | Acceptable |
| Froze | 0.922 (.066) | 13.982 (< 0.001) | 0.884 | Above 0.4 | Acceptable |
| Eat | 0.920 (.070) | 13.198 (< 0.001) | 0.842 | Above 0.4 | Acceptable |
| Stomach | Ref | 0.825 | Above 0.4 | Acceptable |
Factor Loading Estimation of Confirmatory Factor Analysis for the Coronavirus Anxiety Scale
| Fitting Index | Value | Acceptable Range (Threshold) | Result |
|---|---|---|---|
| Chi-square/df | 2.367 | Between 1 to 3 | Acceptable |
| CFI | 0.992 | > 0.90 | Acceptable |
| TLI | 0.974 | > 0.90 | Acceptable |
| RMSEA | 0.086 | < 0.10 | Acceptable |
Goodness Fit Indices and Confirmatory Factor Analysis for Coronavirus Anxiety Scale

Conceptual model for assessing the construct validity of the CAS. CAS: Coronavirus anxiety scale, Dizzy: Dizziness; Sleep: Sleep disturbance; Froze: Tonic immobility; Eat: Appetite loss; Stomach: Nausea or abdominal distress. All of the standardized coefficients are significant at the 0.4 level.
3.3. Reliability
The internal consistency of the questionnaire was confirmed by Cronbach's alpha coefficient of 0.878. Removing any of the questions did not increase the internal consistency of the questionnaire. Moreover, the reliability of the test-retest was evaluated on 30 participants with an interval of two weeks using the intra-class correlation coefficient (ICC). Considering the two-way mixed model, the ICC was 0.931 (95% confidence interval: 0.852 - 0.967).
4. Discussion
The Coronavirus Anxiety Scale, developed in March 2020, is among the first few published screening tools for assessing dysfunctional anxiety induced by the current COVID-19 pandemic (15). The questionnaire was first evaluated among 775 individuals, with an average age of 32.72 (SD = 9.35) years. In that study, Cronbach’s alpha was 0.93. The study reported the questionnaire’s diagnostic qualities (90% sensitivity and 85% specificity) and indicated that it is comparable to other psychiatric screening tests (15). There are 20 translated versions of the CAS on an online site for resources (27), and it has been validated in 10 languages as of now (16-24). A recent study verified the findings of the CAS and lowered the cut-off score from 9 to ≥5 for the general population, and ≥9 when screening at-risk or anxious groups (27). A brief review study indicated that the CAS has been validated in non-clinical samples consisting of middle-aged adults; however, future studies focusing on vulnerable groups are necessary. The study indicated that the CAS is an easy-to-administer and useful tool for clinicians that is consistent with the DSM-5’s cross-cutting symptom measures (10).
We know that evaluating mental health problems among Iranian Healthcare Workers (HCWs) has been somewhat neglected, partly due to the lack of novel and globally standardized scales. Two studies have validated the CAS in Persian among the Iranian general population (25, 26). In both studies, participants had different occupational and socioeconomic statuses. For confirming the reliability, Cronbach's alphas were 91.5 (25) and 0.80 (26), which were in line with our findings. Although the CAS was shown to be reliable and valid in these studies, it was not validated among HCWs. Hence, we contribute to the literature by applying the CAS, as a brief but valid instrument, to evaluate coronavirus anxiety among Iranian nurses as a group of HCWs. Subsequently, 185 nurses participated in the study. They were working in different hospitals and different departments of hospitals affiliated with Mashhad University of Medical Sciences. Accordingly, the survey was conducted among an admissible represented population of HCWs. assessing the results of this study, all five questions of the questionnaire had a content validity Ratio > 0.99 and a CVI > 0.79, confirming its content validity. The construct validity was approved by confirmatory factor analysis. The internal consistency of the questionnaire was confirmed by Cronbach's alpha coefficient of 0.878. Moreover, the reliability of test-retest at two-week intervals showed a high correlation of 0.931 between scores, approving the reproducible results and reliability of the questionnaire.
A remarkable finding of this study was the total CAS score among the nurses. The men's score was 1.86 (SD= 3.03) and the score of women was 2.4 (SD = 3.4). There was no significant relationship between gender and total CAS score (P = 0.32). However, the CAS score in the group of participants aged 30 to 40 years was significantly higher than the score for other participants (P = 0.022). Although Iranian HCWs experienced several challenges during the COVID-19 pandemic, the total CAS score was low. There are two potential explanations for this finding. First, the CAS mean score was low possibly because the study was conducted at the end of the third peak of COVID-19. Second, chronic exposure to anxiety-provoking events and stressors may make people unaware of their anxiety symptoms; therefore, the self-report questionnaire may be biased.
Our study has several limitations. First, we used the available sampling method, which limits the generalizability of the results to the entire healthcare worker community. In addition, we had to distribute the questionnaires online due to social isolation during the pandemic, limiting the researchers' supervision during data collection. As a result, in the final data review, we found that some participants did not answer all the questions, while some filled out the questionnaires twice. We suggest that future researchers use programming and software tools to limit these errors.
4.1. Conclusions
Healthcare workers are one of the most vulnerable groups during the COVID-19 pandemic, for whom, the early detection of coronavirus-related anxiety can facilitate further research and practice on mental health issues. We found that CAS is a valid and reliable tool to evaluate anxiety among Iranian healthcare workers.
