1. Background
The World Health Organization has described oral health as a significant public health issue (1). Some chronic diseases are related to oral and dental problems (2, 3). Accordingly, attention to oral health is on the agenda of the World Health Organization (WHO) to prevent chronic diseases and promote health (4). On average, the overall oral health costs worldwide account for 13% of total health costs, which is a high percentage (5). On a global scale, thousands of people suffer from periodontal diseases, and statistics show that periodontal diseases are of a higher prevalence than cavities (6). Periodontal diseases have many different types, all of which have the common characteristic of altering ideal periodontal conditions and providing the basis for caries (7). Several symptoms, such as inflammation, bleeding, gum disease, bone resorption, a loose tooth and tooth mobility, pain, and many other complications, are complications of periodontal disease. On the other hand, gingival health has a vital role in establishing physical and mental health and would cause depression and anxiety if it interferes with beauty (8, 9).
Studies have shown that a variety of factors underlie periodontal disease, including demographic characteristics such as age and sex, socioeconomic status, inflammatory factors, systemic conditions, medications, tooth-brushing techniques, and many other causes (10, 11). Periodontal diseases are prevalent both in developed and developing countries and affect about 20 - 50% of the global population (3, 12). The Bass technique was reported to be the most effective brushing technique compared with the various tooth-brushing techniques such as Roll or Modified Stillman, Stillman’s, Charters, Bass, Modified Bass, Fones, Leonard, and Scrub (13). This result was based on improved plaque control and reduced gingival inflammation with modified Bass and horizontal scrub techniques. Also, it was reported that the modified Bass technique is superior to normal tooth-brushing practices in terms of reducing supragingival plaques (11, 14).
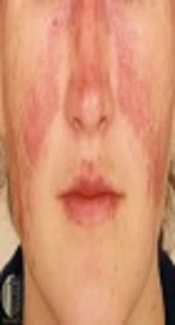
Studies on the association between periodontal diseases and lupus reveal that systemic lupus erythematosus (SLE) is a contributor to the progression of periodontal diseases, and periodontal diseases are an important risk factor in maintaining the inflammatory response in patients with lupus (15). In fact, SLE is a multisystem autoimmune disease with complicated presentations that involves many parts of the immune system. In the context of a favorable genetic predisposition, the disease dysregulates the immune system balance and causes tissue autoimmunity, thereby leading to tissue damage in response to several environmental factors, including the EBV virus (16, 17). The prevalence of lupus is reportedly 1 in 100,000 people (16). Epidemiologic studies of lupus have shown the influence of age, sex, hormones, genetics, and the environment. The prevalence ratio of SLE is 12: 1 in females vs. males, respectively, and women grow a higher risk of developing lupus during pregnancy, which highlights the effect of hormonal changes on the incidence of this disease. In terms of age, it affects people ranging from 2 to 80 years. Studies of racial tendency have shown a higher incidence of the disease in Caucasian and African American individuals (18, 19). Symptoms of lupus may vary depending on the involved organ. Symptoms often include fever, fatigue, mouth ulcers, weight loss, malar rash, light sensitivity, joint pain, renal failure, coronary artery disease, hypertension, and seizures (20, 21).
Early treatment is extremely critical in these patients. In addition, oral findings in patients with lupus can help with early diagnosis (22). The prevalence of oral lesions in patients with SLE was 55.6%. The most affected site was the tongue (25.7%) (23). These lesions can present in various forms, such as red patches, honeycomb plaques, discoid lesions, and lichen planus lesions. Other oral problems include burning sensation, dry mouth, salivary gland disease, TMD, periodontal disease, and oral mucosal ulcers. According to research, the most common site of lesions is lips and buccal mucosa (18). These symptoms present following the severity of the disease (18, 24). The common role of the immune response in lupus and periodontal diseases has been identified. Patients with active lupus often have nonspecific inflammatory markers such as elevated erythrocyte sedimentation rate (ESR) and serum C-reactive protein (CRP) (25). C-reactive protein is an acute inflammatory marker produced in the liver. In the process of inflammation, this protein binds to the membrane of microorganisms and contributes to their elimination through macrophage. Other activities of this protein include a decreased probability of the immune system’s response to the opsonization of bacteria and pathogens (26). Erythrocyte sedimentation rate denotes the rate of erythrocyte sedimentation and is a further elevated marker in lupus patients (27, 28).
Patients with lupus are susceptible to infection due to immunosuppressive drugs and immune abnormalities, where the infection has been reported as one of the leading causes of death in these patients (26). Some studies have shown that periodontal disease is an important risk factor in maintaining the inflammatory response in lupus patients (15). According to research, these inflammatory biomarkers are also linked with oral problems such as periodontal disease (29). In addition, studies have shown that oral problems in patients with lupus are related to their oral health (18, 30).
2. Objectives
This study aimed to evaluate the effect of oral health education on inflammatory factors of patients with lupus to better manage the disease by raising awareness and enhancing services.
3. Methods
3.1. Study Design, Statistical Population, and Sample Size
In the present field trial study, the study population is the patients referred to the specialized rheumatology clinic of Bu Ali building in Birjand. The sample size was computed as 20 participants per group based on the formula:
and the results related to the Biofilm-Gingival Interface index in Fabbri et al.’s study (31).
3.2. Inclusion and Exclusion Criteria
Inclusion criteria comprised a minimum age of 18 years, the fulfillment of SLE criteria, lupus diagnosed not less than six months earlier, SLE-DAI scores smaller than 10, no dental plaque, presence of at least six normal teeth, absence of systemic diseases such as diabetes, and no smoking. Exclusion criteria included pregnancy and intake of xerostomia-inducing medications.
3.3. Sampling Method
Patients were selected by convenience sampling method and divided into two groups by block randomization method. Explanations were presented initially about the necessity, aim, and procedure of completing the research whereby the patients signed written consent forms. Subsequently, they were assigned to two 20-member groups.
3.4. Study Implementation
The intervention group participated in a 20-minute training session on the correct way to brush and floss. The control group did not receive any training. Clinical examination confirmed the absence of dental plaques in both groups, and the Decayed, Missing, and Filled Teeth (DMFT) index was assessed to ensure the presence of at least six healthy teeth in the mouth (inclusion criteria). In both groups, the plaque index was measured using plaque-disclosing tablets. Both groups were matched for the plaque index and subsequently tested for blood ESR, CRP, and dsDNA. In the intervention group, the in-person health education was delivered at the rheumatology clinic by a dental student. After 20 minutes of face-to-face training using teaching aids (molasses, toothbrush, and dental floss), in order to ensure that the participants received the training completely, they were asked to perform the steps in the presence of the trainer, and, if necessary, correction tips were taught to them. Moreover, the project supervisor supervised the health education method. Health education was delivered through the simplest and most common method of health education, i.e., the Bass method. The index plaque was measured for both groups after 3 months (32). Blood samples were taken from the two groups to determine the ESR, CRP, and anti-dsDNA mediators.
3.5. Educational Content
After educating about the characteristics of a suitable toothbrush, the patients were instructed about the way to employ the Bass method using a large-sized dental model. They were told to brush their teeth at least twice a day (before breakfast and before bedtime) and brush their tongue and use dental floss every time they brushed their teeth. In the Bass method, the soft toothbrush head is posited in parallel with the occlusal plan such that the head can cover 3 to 4 teeth. Brushing initiates from the most distal tooth in the maxillary arch. The toothbrush fibers are posited in the gingival margin at a 45-degree angle to the longitudinal axis of the tooth. There will be a gentle tremor pressure, using short back-and-forth movements without removing the tip of the toothbrush fibers. The pressure should produce a noticeable whiteness in the gingiva. As concerns with how to use tooth floss, the participants were taught to break off 12 to 18 inches of the floss. The two ends of the floss are wrapped around the index fingers. The floss gently passes through the interdental contact and is then slid over the proximal side of a tooth to slide below the gingival groove. The tooth floss should move tightly over the tooth. It should then be slowly pushed back into the sulcus, and the procedure be repeated several times (33).
3.6. Statistical Analysis
Data were analyzed by SPSS software using independent t-test, Wilcoxon test, Mann-Whitney, and covariance tests. The significance level was set at α = 0.05.
3.7. Ethical Consideration
Informed consent forms were signed by the participants after the aim and procedure of the study were explained to them, including the steps of examination and measurement of plaque index (due to the temporary staining of teeth after using plaque-disclosing pills). The present study was approved by the Ethics Committee of Birjand University of Medical Sciences (Code: IR.BUMS.REC.1398.031). Also, to comply with ethical principles, a similar training course was held for the control group after the end of the study and measuring the considered variables.
4. Results
This study was conducted with 40 SLE patients, including 20 patients in the intervention group and 20 patients in the control group. The average age of the participants in the intervention group and in the control group was 35.9 ± 11.2 and 42.8 ± 11.1 years, respectively, with no significant difference between the groups (P = 0.06). In terms of gender composition and DMFT index, no significant difference was observed between the two groups. More details are presented in Table 1.
| Variables | Intervention Group | Control Group | Test Statistics | P-Value |
|---|---|---|---|---|
| Age | 35.9 (11.2) | 42.8 (11.1) | 1.96 | 0.06* |
| Sex | 1 | 0.08** | ||
| Male | 1 (5) | 2 (10) | ||
| Female | 19 (95) | 18 (90) | ||
| DMFT index | 12.1 (5) | 14.2 (6.1) | 1.2 | 0.02*** |
Abbreviation: DMFT, decayed, Missing, and Filled Teeth
a * Independent t-test; ** Fisher’s exact test; *** Wilcoxon test.
b Values are presented as No. (%) or mean ± SD.
The mean CRP and SLE-DAI in both groups showed a statistically significant decrease over time, and the difference between the groups both at baseline and after 3 months from baseline was not statistically significant. The mean ESR and dsDNA scores in the intervention group showed a significant reduction after the intervention; however, the difference between groups both at baseline and after 3 months was not significant. The mean O'Leary plaque index (OPI) score reduced significantly in the intervention group after the intervention compared to baseline, but no significant decrease was found in the control group after 3 months. In addition, the two groups were similar in terms of OPI at baseline (Table 2).
Table 2.
Comparison of Mean CRP, SLE-DAI, ESR, dsDNA, and O'Leary Plaque Index in Intervention and Control Groups Before and After the Intervention a
| Time and Point Group | Mean ± SD | P-Value *** | ||
|---|---|---|---|---|
| Baseline | Three Months Later | Changes | ||
| CRP (mg/L) | ||||
| Intervention | 1.15 (0.67) | 0.2 (0.52) | - 0.95 (0.6) | < 0.001 |
| Control | 1.25 (0.64) | 0.3 (0.47) | - 0.95 (0.7) | < 0.001 |
| P-value* | 0.68 | 0.048 | < 0.099 | |
| SLE-DAI | ||||
| Intervention | 7.3 (2.2) | 5.7 (2) | - 1.6 (1.9) | 0.002 |
| Control | 8 (1.8) | 5.9 (1.4) | - 2.1 (1.1) | < 0.001 |
| P-value** | 0.28 | 0.72 | 0.33 | |
| ESR (mm/hr) | ||||
| Intervention | 24.85 (10.7) | 7.25 (5.7) | 17.6 (6.6) | < 0.001 |
| Control | 29.4 (8.7) | 9.1 (5.7) | 20.3 (5.8) | < 0.001 |
| P-value** | 0.15 | 0.31 | 0.18 | |
| dsDNA | ||||
| Intervention | 28.2 (21.9) | 17.3 (13.3) | - 10.8 (11.5) | < 0.001 |
| Control | 30.5 (14.4) | 18.2 (8.5) | - 12.3 (8.4) | < 0.001 |
| P-value** | 0.7 | 0.8 | 0.6 | ---- |
| OPI (mm) | ||||
| Intervention | 80.5 (23) | 64.5 (22.1) | - 16 (10.9) | < 0.001 |
| Control | 95.7 (13.4) | 79.8 (23.5) | - 6.8 (18.8) | < 0.01 |
| P-value* | 0.17 | 0.001 | < 0.001 | ---- |
Abbreviations: CRP, C-reactive protein; dsDNA, double-stranded DNA; ESR, erythrocyte sedimentation rate; OPI, O’Leary plaque index; SLE-DAI, systemic lupus erythematosus disease activity index.
a * Mann-Whitney test; **Independent t-test; *** Wilcoxon test.
The results of covariance analysis showed that by controlling for the effect of patient performance, the educational intervention had a significant effect on ESR (effect size = 9.6). Moreover, the intervention was effective on CRP, dsDNA, and SLE-DAI to the effects of 1.7%, 0.3%, and 6%, respectively; however, the effect was not significant (Table 3).
Table 3.
A Summary of Univariate Covariance Analysis Results for the Effects of the Educational Intervention on ESR, CRP, dsDNA, and SLE-DAI
| Test | Sum of Changes | df | Change Means | F | P-Value | Effect Size (%) |
|---|---|---|---|---|---|---|
| ESR (mm/hr) | 141.17 | 1 | 141.17 | 3.95 | 0.05 | 9.6 |
| CRP (mg/L) | 0.16 | 1 | 0.16 | 0.64 | 0.42 | 1.7 |
| dsDNA | 14.64 | 1 | 16.64 | 0.11 | 0.74 | 0.3 |
| SLE-DAI | 0.68 | 1 | 0.68 | 0.22 | 0.64 | 0.6 |
Abbreviations: CRP, C-reactive protein (CRP); dsDNA, double-stranded DNA; ESR, erythrocyte sedimentation rate; SLE-DAI, systemic lupus erythematosus disease activity index.
5. Discussion
The relationship between periodontal diseases and inflammatory conditions, diabetes, and cardiovascular diseases is well explicated. SLE and periodontitis are both inflammatory diseases that affect the immune system (34-36). B lymphocyte plays a significant role in the development of SLE and periodontitis. Moreover, an increased level of IgG2, a subgroup of IgGs, has been observed in lupus and periodontitis (37, 38). Many case studies have demonstrated the association between periodontal disease and lupus (36, 39, 40). Based on the findings of the present study, of the 40 patients studied, 3 were males, and 37 were females. These findings are in agreement with those of Rees et al.’s study (41), which indicates a range of 2: 1 to 9: 1 ratio of lupus incidence in females compared to males.
The mean age was 35.9 ± 11.2 years in the intervention group, and it was 42.8 ± 11.1 years in the control group. This age range of lupus incidence corresponds with the range defined in Burket as a reference source. Burket reports the highest age of lupus incidence from 20 to 40 years (42).
Based on the results of the present study, the mean O'Leary plaque index score in the intervention group showed a significant decrease after the intervention compared to baseline, while there was no significant decrease in the control group. This difference indicates the effectiveness of the intervention in reducing dental plaques of patients present in the intervention group. Amiri et al. also reported that the preventive health education program improved oral hygiene indices, including the plaque index (43). According to the findings of the present study, the mean OPI index score in both the control and intervention groups was 83.6 at baseline. An OPI score above 70% indicates poor oral health (33). Fernandes et al.’s study, which examined the oral health and masticatory system in juvenile patients with SLE, reported poorer oral health and higher prevalence rates of gingivitis and jaw disorders in this group of patients, which is in agreement with the results of the present study (44).
The results of this study showed that there was a significant decrease in the mean ESR index score after 3 months of intervention in both groups. This decrease in ESR is justifiable in both groups, given the fact that patients with SLE are treated with anti-inflammatory drugs. In the present study, the difference between the mean ESR reductions in the two groups was not statistically significant. Investigating the effect of periodontitis treatment on improving the efficacy of immunosuppressive therapy in patients with SLE, Fabbri et al.’s study showed that periodontal treatment slightly decreased ESR after 3 months. However, the reduction was significant in our study. In Fabbri’s study, the ESR index score showed a significant decrease after six months of treatment compared to the control group. In comparison to the results of our study, this finding may suggest the effect of the time factor on the effectiveness of health intervention on inflammatory factors such as ESR (31). In Al-Katma et al.’s study (37), the ESR index score in the group receiving health education and dental plaque removal increased by 76.4%, while only the improvement rate was 16.7% in the control group. The reduction in both groups is in line with the findings of the current study. In Al-Katma et al.’s study, there was a significant difference between the two groups in terms of ESR after 8 weeks, indicating the significant effect of dental plaque removal on ESR improvement. In this regard, the percentage is not consistent with our findings. Given that the lack of dental plaque was an inclusion criterion in the present study, the patients did not need to have plaque removal but only received health education. On the other hand, the time duration considered for the impact of the intervention was longer than that of Al-Katma et al.’s study.
The results of the present study show that the CRP index significantly decreased in both study groups, but there was no statistically significant difference between the groups. This result is in contrast to the results of Fabbri et al.’s study (31), in which CRP was reduced only slightly after dental plaque treatment and health education. Also, in D'Aiuto et al.’s study on patients with rheumatoid arthritis (RA), there was a significant decrease in CRP and interleukin-6 only in the periodontal disease management group after two months from plaque removal and plaque control (45), which does not correspond with our findings. Calderaro et al. (46) performed a systematic study concerning the effect of periodontal treatment of RA. In all four case-control studies included in this systematic study, the control and intervention groups were followed at six weeks, eight weeks, and six months after the periodontal treatment. Periodontal treatment included plaque removal, root planning, and health education. The results of this study showed that DAS28 decreased in the intervention group, whereas CRP and ESR showed no significant change, which is similar to the results obtained in the present study.
The non-significant difference found in this study between the two groups in terms of reduction in ESR and CRP could be due to the intake of corticosteroid drugs by patients with SLE. These drugs can improve inflammation laboratory markers in patients (47). Al-Mutairi et al. study showed that peritoneal dialysis (PD) in patients with lupus flare-up was significantly lower than in patients with a stable status to justify the finding on the ground that patients with lupus flare-up take increased drug doses, leading to greater control of inflammation and subsequent control of periodontal diseases. In the present study, both study groups were treated with the same doses of medication, and this may be the reason underlying the lack of difference in the extent to which ESR and CRP were reduced in the two groups (48). The results of this study showed that the dsDNA index decreased significantly in both groups after the intervention; however, the difference was not significant between the two groups.
The results of the present study revealed a significant decrease in the mean SLE-DAI in both groups after the intervention. Nevertheless, between-group differences were not significant. After 3 months of non-surgical periodontal treatment, Fabbri et al. (31) reported a significant decrease in the SLE-DAI in the intervention group, which is inconsistent with the results of the present study. Since in both of these studies, lack of dental plaque was an inclusion criterion, and the patients received only health education, the different sample sizes and the methods employed in these two studies may underlie the difference between the studies. Areas et al.'s study, suggests that some inflammatory cytokines are present in lupus and periodontal diseases, including IL-18, which is also associated with SLE-DAI and periodontal parameters (49). Moreover, several studies (32, 37, 41) have demonstrated the impact of periodontal diseases on the therapeutic pathway of SLE and RA diseases. However, the results of the present study did not show a significant relationship between health education intervention and SLE-DAI as an indicator of the severity of lupus disease.
By controlling the effect of patient performance on ESR, CRP, dsDNA, and SLE-DAI, the covariance analysis showed that the oral health education intervention had a significant effect on ESR, with an effect size of 9.6%. The educational intervention was effective on CRP, dsDNA, and SLE-DAI (effect sizes of 0.6%, 0.3%, and 7.1%, respectively); however, the effects were not significant. These results indicate that oral health education had a significant impact on controlling the ESR factor and, consequently, leading to disease management in patients with SLE. Patients with lupus experience higher severity of periodontal disease due to decreased salivary secretion, dry mouth, and subsequently reduced antibacterial effect of saliva (18). Under these conditions, opportunistic microorganisms such as porphyromonas gingivalis (PG) can cause periodontal diseases. Also, gingivitis is more common and severe in individuals with immune defects due to the use of immunosuppressive drugs and chronic diseases such as lupus (50). In patients who do not have dental plaque and do not need scaling, oral flora, such as PG, can reduce with oral and dental hygiene training, where inflammatory pathways can be controlled. Since one of the causes of SLE flare-ups is the activation of these inflammatory pathways (51), health education can have a positive impact on SLE disease control. Also, based on the results of the present study and relying on the results of covariance analysis, this study demonstrated that the educational intervention had a significant impact on the ESR index in patients with lupus, which can make the lupus disease more controlled in these patients.
According to the small sample size in this study, the results may not represent the whole population. Therefore, it is advisable to conduct a similar study with a larger sample size. Also, given the type of intervention employed in this study, it is suggestible to consider longer-term follow-ups to study the effect of oral health education more closely.
5.1. Conclusions
After the effect of the patient performance was controlled, the study found that the educational intervention affected the most substantial change in the ESR index (effect size: 9.6%) and had the least effect on the dsDNA index. In both groups, the dsDNA index decreased after the intervention, although the difference between the groups was not significant. After 3 months, CRP did not show a significant decrease in this study. Also, the OPI index in the intervention group revealed a significant decrease after the intervention, indicating the positive effect of the intervention on reducing plaque index. Therefore, given the significant impact that the intervention had on the ESR index as well as the affordability and low cost of health education, it can be recommended to attempt to inform all patients with lupus about oral hygiene/health.