1. Background
Middle age is a significant phase in a woman's life, typically spanning from 40 to 60 years of age (1). According to a report from the Statistical Centre of Iran, 23% of Iranian women are middle-aged (2). Middle-aged women are usually exposed to several health conditions, including physical changes such as decreased physical ability and visual acuity, as well as alterations in their overall health status (3). Additionally, they may experience a decline in self-confidence, a sense of diminished control over their lives, decreased well-being and self-worth, and a higher prevalence of depression and psychological problems (4).
Unhealthy lifestyles are another major concern, as highlighted by the World Health Organization (WHO). The WHO reports that 60% of global deaths and 80% of deaths in developing countries are attributed to unhealthy lifestyle choices. These statistics are projected to reach 75% of the global mortality by 2030 (5). Individuals are encouraged to adopt a health-promoting lifestyle to mitigate this trend; this lifestyle is characterized by conscious efforts to improve health through self-initiated and sustained behaviors. This lifestyle includes practices such as maintaining a proper diet, prioritizing sleep, engaging in physical activity, managing body weight, abstaining from smoking and excessive alcohol consumption, and receiving immunizations (6).
The concept of a health-promoting lifestyle involves six dimensions: Interpersonal relationships, responsibility for one's health, spiritual growth and self-actualization, stress management, nutrition, and physical activity. Embracing these dimensions and actively pursuing a health-promoting lifestyle can contribute to maintaining and enhancing an individual's overall health, psychological well-being, and self-fulfillment (7). The study conducted by Abbaspoor et al. in Ahvaz, Iran, examined 600 urban middle-aged women and found that the prevalence of overweight was 36.5%, while the prevalence of obesity was 36.5%. This highlights the significance of weight-related problems among middle-aged women in that particular region (8).
Furthermore, another study conducted in Tehran, Iran, revealed that approximately 34% of individuals aged 15 years and above, including 37.9% of women and 28.6% of men, potentially suffer from psychological disorders (8). The high prevalence of psychological health disorders in the population emphasizes the crucial need for effective interventions to address these problems (9).
Mindfulness counseling has emerged as a widely used approach in modifying and improving lifestyles to promote better health (3). Mindfulness is a state of awareness that is present-focused and nonjudgmental about an experience that is within the scope of a person's attention at a particular moment, and it involves acknowledging and accepting the experience (10). The goal of mindfulness therapy is to encourage people to be present in the moment, to be nonjudgmental, accepting, patient, open, curious, kind, and undoing (11). It is expected that by practicing mindfulness, patients should develop the skills needed to pay full attention to the present moment with nonjudgmental awareness and cope with their physical pain or psychological distress (12).
Various studies have demonstrated the positive impact of mindfulness counseling on reducing health-threatening factors (13) and enhancing positive psychological components, ultimately leading to an improved quality of life (14). Mahdipour et al. demonstrated the beneficial effects of a counseling program on different aspects of women's lifestyles (15).
Given the various psychological, social, and biological factors that impact the lives and lifestyles of women in their middle age (16) acknowledging the crucial role of women's health in increasing overall public health and societal progress and based on the effectiveness of mindfulness-based counseling in promoting health and well-being, the present study aimed to assess the effectiveness of this intervention in promoting the lifestyle of middle-aged women.
2. Objectives
The objective of this study was to examine the effectiveness of mindfulness-based counseling on health-promoting lifestyles in Iranian middle-aged women.
3. Methods
3.1. Study Design and Participants
An experimental design was employed, involving 48 middle-aged women who were referred to Comprehensive Health Services Center No. 1 in Lordegan, Iran, from October 2020 to February 2021.
The participants were randomly assigned to two groups, intervention (which received counseling) and control, using a block size of 4. Allocation concealment was ensured by writing the type of study written on a piece of paper and placing the pieces in opaque envelopes, which were consecutively numbered. The envelopes were opened in the order of participant enrollment to determine group assignment.
3.2. Sampling
Sample size determination was based on a previous similar study conducted by Karimlou et al. (3) using the MDE-Calculator statistical software and the following formula:
In this formula, Z1-α/2 = 1.96, β = 63.11, Zβ = 1.32, Sd1 = 11.37, Sd2 = 14.63, µ1 = 66.21, µ2 = 63.11, µ1-µ2 = 14.1. The calculated sample size was 20 per group. An additional 20% was added to account for potential attrition during the research period, resulting in a final sample size of 24 per group. If the following criteria were met, the participants were eligible to participate in the study: Being able to read and write, having given informed consent, being between 30 and 59 years old, and obtaining a score lower than 135 on the HPLP-II questionnaire. Moreover, based on the exclusion criteria, participants who had a history of known chronic or acute physical or mental illnesses, were currently taking psychoactive drugs prescribed by a doctor or psychiatrist, were involved in similar programs, showed unwillingness to continue to participate in the study, or did not complete the questionnaires were excluded.
3.3. Data Collection Tools
The researchers utilized a sociodemographic questionnaire and the Persian version of the HPLP-II (19). Both groups filled out the HPLP-II through interviews with the first author (Mojgan Nekoei) at the health center before and 4 weeks after the intervention.
Sociodemographic questionnaire: This questionnaire was developed by the researchers to obtain the personal information of the participants. It collected information about age, marital status, education level, occupation, place of residence, length of marriage, body mass index (BMI), number of children and their age, the spouse's occupation, and his education level.
Walker's HPLP II: The original version of this questionnaire was designed by Walker et al. (7). It consists of 52 items (7) that measure the health-promoting lifestyle across 6 domains: Nutrition (having a food pattern and choosing food, 9 items, score: 9 - 36), physical activity (following a regular exercise pattern, 8 items, score: 8 - 32), responsibility for health (9 items, score: 9 - 36), stress management (8 items, score: 8 - 32), interpersonal support (maintaining relationships with a sense of closeness, 9 items, score: 9 - 36), and self-actualization involves having a sense of purpose, seeking personal development, and experiencing self-awareness and satisfaction (9 items, score: 9 - 36).
The questionnaire uses a 4-point Likert scale for each item, with responses ranging from 1 (never) to 4 (always and usually). The total score of the items of each dimension shows the total score related to that lifestyle dimension (20). The questionnaire has a maximum score of 208, while the minimum score is 52.
A score of 52 to 81 represents an undesirable lifestyle, a score between 81 to 135 indicates a moderately desirable lifestyle and a score of ≥ 135 shows a desirable lifestyle (21).
The content validity assessment method was applied to determine the validity of the sociodemographic questionnaire.
The questionnaire was initially drafted by reviewing scientific texts and articles, and after the approval of the research team, 10 academic staff members with expertise in midwifery and reproductive health reviewed the questionnaire; the final version was confirmed after making the necessary corrections for its qualitative face and content validity.
Mohammadi Zeidi et al. confirmed the validity and reliability of the HPLP-II questionnaire through exploratory factor analysis. Cronbach's alpha coefficients for the components of nutrition, responsibility, stress management, interpersonal relationships, and self-actualization were 0.74, 0.84, 0.80, 0.74, and 0.74, respectively, while the coefficient for the entire scale was 0.82. Confirmatory factor analysis revealed an acceptable fit for the 6-factor model (19).
3.4. Intervention Program
The intervention group participated in 8 weekly sessions (60 to 90 minutes each) of group mindfulness-based counseling held at one of the classes of the Comprehensive Health Center in Lordegan. Before data collection, oral and written informed consent was obtained from each participant. The first author (Mojgan Nekoei), who had undergone appropriate training and obtained certification in mindfulness-based counseling through workshops, led the counseling sessions. A psychologist consultant, who attended some of the counseling sessions to ensure the validity of the intervention, supervised the sessions. Each counseling session presented a mindfulness-based counseling program that combined the principles of mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT) (22). The contents of the MBSR sessions are presented in the Appendix 1.
Eight sessions of mindfulness training were administered to the women in the mindfulness group to promote a healthy lifestyle (1 session per week). The mindfulness group was divided into 3 groups of 8 women.
Each group received 8 sessions of 60 - 90 minutes each.
The participants were provided with guiding booklets and were encouraged to practice the presented mindfulness techniques for 45 minutes a day, 6 days a week. The counseling sessions aimed to establish effective communication with the participants, create a friendly and respectful atmosphere for group discussions, and enhance the women's self-confidence. The counseling sessions covered a range of topics related to health-promoting behaviors, such as healthy nutrition, physical activity, stress management, techniques for building better relationships, and strategies for enhancing spiritual growth and health responsibility.
The control group was given standard care provided by the health center. After the intervention period, the control group was provided with CDs that contained the same content as the topics discussed in the counseling sessions. Four weeks after the completion of the mindfulness counseling sessions, the researcher administered the HPLP II questionnaire once again to both groups to collect follow-up data.
3.5. Data Analysis
The Kolmogorov-Smirnov test was used to assess the normality of the data distribution.
Descriptive statistical methods such as mean and SD for quantitative variables and frequency and percentage for qualitative variables were used to analyze the data, along with independent and paired t-tests, chi-square, and Fisher's exact test. For data analysis, SPSS v. 24 (IBM Corp., Armonk, NY, USA) was utilized. The statistical significance of the findings was determined based on a P-value of less than 0.05.
4. Results
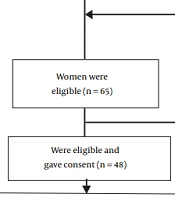
A total of 48 participants were recruited for the study, and there were no instances of attrition or participant dropout (Figure 1).

Figure 1.
The flow diagram of the recruitment and retention of participants
There was no significant difference between the mean age of the participants in the intervention (38.91 ± 3.51) and control (37.29 ± 3.81) groups (P = 0.132). Most of the participants in both intervention (54.2%) and control (72%) groups had a university education, and more participants in both intervention (62.5%) and control (79.2%) groups were employed. In general, the two groups exhibited homogeneity in sociodemographic characteristics (P > 0.05; Table 1).
Table 1.
Comparison of Sociodemographic Characteristics Between the Two Groups of Counseling and Control a
| Sociodemographic Characteristics | Counseling Group n = 24 | Control Group n = 24 | P-Value |
|---|---|---|---|
| Age (y) | 38.91 ± 3.51 | 37.29 ± 3.81 | 0.132 b |
| Duration of marriage | 14.29 ± 4.26 | 13.50 ± 4.67 | 0.558 b |
| Spouse's age | 42.16 ± 4.34 | 41.58 ± 4.33 | 0.643 b |
| Number of children | 2.62 ± 0.87 | 2.08 ± 1.01 | 0.054 b |
| Level of education | 0.157 c | ||
| High school | 1 (4.2) | 1 (4.2) | |
| High school diploma | 10 (42.7) | 5 (20.8) | |
| University | 13 (54.2) | 18 (72.0) | |
| Job | 0.204 d | ||
| Homekaer | 9 (37.5) | 5 (20.8) | |
| Employed | 15 (62.5) | 19 (79.2) | |
| Place of residence | 0.074 d | ||
| City | 24 (100.0) | 21 (87.5) | |
| Village | 0 (0.0) | 3 (12.5) | |
| Marital status | 0.312 d | ||
| Married | 23 (95.8) | 24 (100.0) | |
| Single | 1 (4.2) | 0 (0.0) | |
| Body mass index (kg/m2) | 0.620 c | ||
| < 18.5 | 0 (0.0) | 1 (4.2) | |
| 18.5 - 25 | 7 (29.2) | 5 (20.8) | |
| 25 - 30 | 11 (45.8) | 10 (41.7) | |
| > 30 | 6 (25.0) | 8 (33.3) | |
| Husband's job | 0.390 c | ||
| Employed | 8 (33.3) | 13 (54.2) | |
| Worker | 5 (20.8) | 0 (0.0) | |
| Freelancer | 10 (41.7) | 11 (45.8) | |
| Unemployed | 1 (4.2) | 0 (0.0) | |
| Spouse's education level | 0.878 c | ||
| High school | 7 (29.2) | 8 (33.3) | |
| High school diploma | 7 (29.2) | 6 (25.0) | |
| University | 10 (41.7) | 10 (41.7) |
a Values are expressed as No. (%) or mean ± SD.
b Independent t-test.
c Fisher's exact test.
d Chi-square.
Before the intervention, the mean (SD) score of the health-promoting lifestyle was 113.04 ± 24.05 in the counseling group and 109.41 ± 15.68 in the control group. Four weeks after the intervention, the mean (SD) score of the health-promoting lifestyle was 151.66 ± 14.01 in the counseling group and 107.75 ± 12.27 in the control group. The paired t-test indicated a significant difference in the mean score for the health-promoting lifestyle and its dimensions after the intervention compared to before the intervention (P < 0.001). Additionally, after the intervention, an independent t-test showed a significant difference between the mean score of the two groups for the health-promoting lifestyle and its dimensions (P < 0.001; Table 2).
Table 2.
Health-Promoting Lifestyle Score Within and Between Groups Before and After the Intervention a
| Health-Promoting Lifestyle and Time | Counseling Group (n = 24) | Control Group (n = 24) | P-Value |
|---|---|---|---|
| Total HPLP-II score | |||
| Pretest | 113.04 ± 24.05 | 109.41 ± 15.68 | 0.539 |
| Posttest | 151.66 ± 14.01 | 107.75 ± 12.27 | < 0.001 |
| P-value | < 0.001 | 0.298 | |
| Self-actualization | |||
| Pretest | 27.70 ± 6.47 | 26.20 ± 4.26 | 0.348 |
| Posttest | 33.04 ± 3.45 | 25.41 ± 4.09 | < 0.001 |
| P-value | < 0.001 | 0.193 | |
| Responsibility | |||
| Pretest | 26.54 ± 4.61 | 25.66 ± 5.71 | 0.562 |
| Posttest | 33.36 ± 4.34 | 24.91 ± 4.51 | < 0.001 |
| P-value | < 0.001 | 0.221 | |
| Stress management | |||
| Pretest | 9.79 ± 3.13 | 9.91 ± 1.74 | 0.865 |
| Posttest | 14.75 ± 2.69 | 9.25 ± 1.70 | < 0.001 |
| P-value | < 0.001 | 0.130 | |
| Interpersonal support | |||
| Pretest | 17.95 ± 4.45 | 18.79 ± 3.76 | 0.488 |
| Posttest | 23.41 ± 3.13 | 18.29 ± 2.89 | < 0.001 |
| P-value | < 0.001 | 0.124 | |
| Physical activity | |||
| Pretest | 12.70 ± 5.64 | 11.45 ± 3.78 | 0.372 |
| Posttest | 21.12 ± 3.72 | 11.08 ± 3.39 | < 0.001 |
| P-value | < 0.001 | 0.195 | |
| Nutrition | |||
| Pretest | 18.41 ± 4.08 | 19.37 ± 4.30 | 0.433 |
| Posttest | 23.01 ± 4.65 | 18.04 ± 4.13 | < 0.001 |
| P-value | < 0.001 | 0.127 |
Abbreviation: HPLP-II, health-promoting lifestyle profile II.
a Values are expressed as mean ± SD.
5. Discussion
This study evaluated the effect of mindfulness counseling on the health-promoting lifestyle of middle-aged women. The results showed that 4 weeks after the intervention, the total score of the health-promoting lifestyle and its domains, including self-actualization, responsibility, stress management, interpersonal support, physical activity, and nutrition, improved significantly in the mindfulness group as compared to the control group.
In our review of the literature, we found only one study pertaining to the impact of mindfulness on a health-promoting lifestyle in middle-aged women; still, several studies have explored the influence of mindfulness counseling or training on stress or self-management action plan initiation.
In the present study, the dimension with the most elevated mean score was health responsibility (33.36 ± 4.34), while the dimension of stress management attained the lowest score (14.75 ± 2.69). The mean (SD) scores for self-actualization, nutrition, interpersonal relations, and physical activity were 33.04 ± 3.45, 23.01 ± 4.65, 23.41 ± 3.13, and 21.12 ± 3.72, respectively. In accordance with our findings, in research on 104 menopausal women, Jalambadani also discovered that mindfulness counseling had a significant impact on improving lifestyle behaviors. Note that the dimension of nutrition received the highest mean score of 35.14 ± 3.35, while physical activity received the lowest mean score of 14.89 ± 3.55. The mean (SD) scores of stress management, interpersonal relations, and health responsibility were 21.54 ± 1.12, 26.00 ± 2.54, and 16.87 ± 4.10, respectively (23).
The difference regarding the highest and lowest scores of dimensions between the two studies could be due to the population of the studies. Jalambadani studied menopausal women. Middle-aged women had a higher responsibility but had lower stress management than menopausal women.
Galla et al. examined 127 community residents who received mindfulness training through mindful awareness practices (MAPs) for daily living. They found significant improvements in self-reported mindfulness, self-compassion, and perceived stress post-intervention and concluded that a community-based mindfulness-training program can reduce the level of stress (24). Gawande et al. examined 465 patients who had a diagnostic and statistical manual of mental disorders, fifth edition (DSM-V) diagnosis over 12 months. They found that in an intention-to-treat analysis, participants who were randomized to MTPC had significantly higher adjusted odds of initiation of self-management action plans compared to those who were randomized to low-dose comparator (LDC) (OR = 2.28; 95% CI = 1.02 to 5.06, P = 0.025) (25). Our results regarding the health-promoting lifestyle are similar to those of Galla et al. and Gawande et al. (24, 25).
This research has some limitations that require attention. First, the participants in the mindfulness group did not receive personalized counseling based on their individual educational and sociocultural backgrounds. Second, we assumed that the questionnaire responses provided by middle-aged women were completely accurate. These limitations may have influenced the overall results and should be taken into account when interpreting the findings.
5.1. Conclusions
The present study provided evidence that mindfulness counseling improved the health-promoting lifestyle of middle-aged women after the intervention. The positive effects of the intervention on health-promoting lifestyles suggest that health and medical officials should prioritize the development and administration of preventive and curative policies in this field. By addressing lifestyle-related problems, such interventions can help mitigate potential health problems that may arise during middle age.