




1. Background
Currently, lifestyle modification, especially attention to health-promoting lifestyle, is a prerequisite for maintaining and promoting individuals’ health (1). Many health problems, various chronic diseases such as obesity, various cancers, hypertension, diabetes, and the deaths caused by them are the result of people’s unhealthy behavior and lifestyle (2). If behavioral and lifestyle problems are identified and changed in time, their adverse consequences on health will be prevented (3).
In its declaration at the First World Conference on Healthy Living in Moscow, the World Health Organization (WHO) stated that 60% of the deaths worldwide and 80% of deaths in developing countries are due to unhealthy lifestyles, increasing to 75% of the deaths worldwide by 2030 (4). Thus, modern health care has gradually shifted its focus from examining mortality as a health consequence to broader areas such as health promotion, lifestyle, and quality of life (5).
A health-promoting lifestyle empowers people to increase control over and improve their health (6). A health-promoting lifestyle is known as a balanced lifestyle in which people always make informed choices about their health and well-being and improve their health by engaging in behaviors such as regular physical activity and a healthy diet, establishing friendly relationships with others, controlling and reducing stress in daily life, and other health-promoting activities (7).
One of the widely-used models for predicting factors affecting health-promoting behaviors and quality of life is Pender’s health promotion model that includes the concepts that determine health-promoting behaviors such as personal experiences and characteristics, specific feelings, cognitive-perceptual elements, and behavioral outcomes. Individual characteristics and experiences have direct or indirect effects on the likelihood of engaging in health-promoting behaviors through cognition and emotions and include personal factors and similar behaviors in the past. Cognition and specific emotions directly affect behavior and include constructs such as perceived benefits and barriers, perceived self-efficacy, behavior-related emotions, interpersonal influencers, and situational influencers. According to Pender, health-promoting behaviors, especially when adapted to a healthy lifestyle, lead to the development of health, the improvement of structural abilities, and a better quality of life at all stages of development (8).
The four most important components of a health-promoting lifestyle include nutrition, exercise, stress management, and health responsibility. A review of previous studies suggests that lifestyle correlates with individual-societal characteristics (9, 10). Some studies have shown that people with lower levels of education are less likely to follow health-promoting behaviors (11, 12). Living with a partner increases the likelihood of following health-promoting behaviors (11), and the health-promoting lifestyle is related to economic status and social class (13) and the number of family members (14). Previous studies (e.g., Hajizadeh Meimandi and Dehghan Chenary, 2015; Hirth, 2010; Rakhshani et al., 2014) have indicated that married people have a better health-promoting lifestyle. A study by Mirghafourvand et al. (15) in Tehran on women of childbearing age also showed that social support, age, marriage, and education are related to health-promoting behaviors. Movahed et al. (16) showed that social support is the most important factor in the lifestyle of the elderly and is a strong determinant promoting the health of individuals. Zanjeri (17) highlighted the importance of self-efficacy in women’s lifestyle and considered it the most important factor after social support. A study by Mirghafourvand et al. (15) showed that age and income are the factors associated with health-promoting behaviors.
Experts also believe that a health-promoting lifestyle is a useful source to reduce life stressors and has a significant effect on reducing health costs, increasing people’s life expectancy, and improving their quality of life. Therefore, such a lifestyle has special importance and position in society (18). Besides, paying attention to the health and social welfare of women, who make up half of the population, is not only recognized as a right, but it has received considerable attention due to its impact on family and community health. In addition, since women play a vital role in caring for themselves, children, the elderly, the sick, and other family members at home (19), women’s choice of lifestyle not only affects their personal life but also other people’s lifestyles and behaviors. Accordingly, disregard for women’s health can lead to permanent problems related to the lifestyle and health of future generations (20).
According to the latest 2016 Population and Housing Census, the population of Sistan and Baluchestan Province is 2775014 persons, and the population of women of childbearing age is 720459 people, accounting for 52% of the population of women and 26% of the population of the province. However, there is little research on the health-promoting lifestyle of women of reproductive age. The total fertility rate in the province is 3.96, which is the highest fertility rate in the country (21). Furthermore, socio-cultural conditions, underdevelopment, low literacy, the lack of full access to health care facilities, and social inequalities always threaten the health of women in this province, so that they have lower ranks in most health indicators compared to the national average.
2. Objectives
Considering that health promotion activities and a healthy lifestyle are the main strategies to facilitate and protect health, and since no study has addressed the health-promoting lifestyle and its factors among women of reproductive age in the province, the present study aims to determine the predictors of a health-promoting lifestyle among women aged 15 - 49 based on Pender’s health promotion model.
3. Methods
The present study is a descriptive-analytical cross-sectional study conducted in the fall of 2019. The respondents were 200 women aged 15 - 49 living in Zahedan who were randomly selected from five districts of the city using the multi-stage sampling method. To this end, based on the latest census and blocking of the Statistical Centre of Iran, the urban districts were selected as clusters, and two blocks were randomly selected from each cluster. Then, of every two women meeting the inclusion criteria in each block, one woman was selected randomly. Accordingly, 20 women aged 15 - 49 years were selected from each block. The inclusion criteria were being at the age of 15 - 49, having no drug addiction, and having no history of underlying diseases and mental health problems.
The sample size was calculated using the Cochran’s formula and based on the population of 15 - 49 women in Zahedan and lifestyle variance (Mohamadian et al., 2011) with 95% confidence interval and 95% test power (Equation 1):
Where Z = 1.96, S2 = 0.13, d = 0.05, and N = 182483.
The instruments used to collect the data were the demographic information form, the Perceived Self-Efficacy scale, the Perceived Social Support scale, the Perceived Emotions scale, the perceived barriers scale, and the health-promoting lifestyle profile II (HPLP II):
The Demographic Information Form: It was used to assess the respondents’ age, education, occupation, household income, ethnicity, religion, and the number of children.
The Perceived Self-Efficacy Scale: The scale was adapted from the Smith et al.’s Health scale, and it contains 8 items scored based on a 5-point Likert scale ranging from “strongly agree” to “strongly disagree”. The score range on this scale is from 8 to 40, with a higher score on this scale indicating that the individual has a high ability to control the outcomes and consequences of his/her health-related programs. Smith et al. (22) estimated the reliability of the scale equal to 0.84 using Cronbach’s alpha coefficient. In the present study, the reliability of the scale was calculated as 0.77 using Cronbach’s alpha coefficient.
The Perceived Social Support Scale: The scale was adapted from the scale developed by Canty-Mitchell and Zimet (23) This scale measures social support received from three separate sources, including family, friends, and significant others. The scale contains 12 items (4 items for each source) that are scored on a seven-point Likert scale ranging from “strongly agree” to “strongly disagree”. The total score for each source ranges from 4 to 24, and a higher score indicates more support from family, friends, and significant others. The Cronbach’s alpha value reported by Canty et al. for the whole scale was 0.91, and the corresponding values for each source vary from 0.90 to 0.95 (23). In the present study, the reliability of the scale was calculated and reported as 0.88 using Cronbach’s alpha coefficient.
The Perceived Emotions Scale: This scale was developed based on Watson et al.’s (24) tool and contains 20 items that are scored on a 5-point Likert scale from “never” to “always”. The scale has two subscales, including positive affect (10 items) and negative affect (10 items). The total score on each subscale ranges from 10 to 50 with a higher score reporting better emotional states over the past 24 hours. Watson et al. reported a Cronbach’s alpha coefficient of 0.94 for positive affect and 0.91 for negative affect (24). In the present study, the reliability of the instrument was calculated using Cronbach’s alpha coefficient with a value of 0.75.
The Perceived Barriers Scale: The instrument was adapted from a scale developed by Becker and Stuifbergen (25) and contains 18 items scored on a 4-point Likert scale ranging from “never” to “always”. The total score ranges from 18 to 72, and a higher score indicates that the respondent faces more barriers to engagement in health-promoting behaviors. Cronbach’s alpha coefficient was reported by Becker et al. 0.80, and the test-retest coefficient was 0.75 (25). In the present study, the reliability of the instrument was calculated using Cronbach’s alpha coefficient as 0.83.
The Health-Promoting Lifestyle Profile II: This instrument was developed by Walker et al. (26) and contains 32 items that are scored based on a 4-point Likert scale ranging from “never” to “always” and are categorized into four subscales: nutrition, exercise, stress management, and health responsibility. The total score on this scale ranges from 32 to 128, and higher scores indicate that respondents are following a better health-promoting lifestyle. Cronbach’s alpha coefficient for the tool was reported by Walker et al. as equal to 0.94 (26). The reliability of the instrument was calculated using Cronbach’s alpha coefficient in the present study, and the related value was 0.89.
Trained interviewers referred to the respondents’ homes to complete the questionnaires. The questionnaires for each respondent were completed in one session. If the respondent was literate, she would complete the questionnaire after receiving some instructions from the interviewer on how to answer the questions. However, if the respondent was illiterate, she would be interviewed, and the questionnaires would be completed by the interviewer. All respondents in the present study were informed of the objectives of the study, and informed written consent was obtained from them. Besides, to ensure the confidentiality of the information, the questionnaires were completed without recording the respondents’ names.
The collected data were analyzed through descriptive statistics, Pearson correlation coefficient, independent samples t-test, one-way analysis of variance (ANOVA), and multiple linear regression analysis using the enter method in SPSS software (version 25). Before doing multivariate analysis, regression assumptions, including normality and homoscedasticity of residuals, the collinearity of outlier data, and residual independence, were checked. All statistical procedures were performed at a significant level of less than 0.05 (P < 0.05).
4. Results
The mean age of the respondents was 31.36 ± 8.53 years. Most respondents were married (74%). Besides, 30.5% of them were employed, and 34.5% had associate’s and bachelor’s degrees. Furthermore, 54.5% of the respondents stated that their access to health services was moderate.
The mean score of health-promoting lifestyle for the respondents was 69.82 ± 13.59. Besides, among the lifestyle subscales, nutrition and exercise had the highest and lowest mean scores (20.08 ± 4.23 vs. 14.19 ± 4.51), respectively (Table 1).
| Variable | Values | Range |
|---|---|---|
| The total score of the health-promoting lifestyle | 69.82 ± 13.59 | 32 - 128 |
| Nutrition | 20.08 ± 4.23 | 8 - 32 |
| Exercise | 14.19 ± 4.51 | 8 - 32 |
| Stress management | 19.02 ± 4.27 | 8 - 32 |
| Health responsibility | 16.25 ± 4.61 | 8 - 32 |
aValues are expressed as mean ± SD.
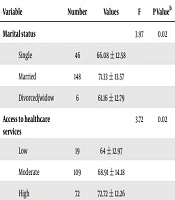
The results of one-way ANOVA and independent samples t-test indicated that the respondents’ mean scores of health-promoting lifestyle were not significantly different in terms of age, education, household income, and the number of children. However, the respondents’ lifestyle showed significant differences in terms of marital status and access to health services (P = 0.02). For instance, the married respondents (with a mean score of 71.33) and those who had high and very high access to health services (with a mean score of 72.72) had a healthier lifestyle than other groups (Table 2).
| Variable | Number | Values | F | P Valueb |
|---|---|---|---|---|
| Marital status | 3.97 | 0.02 | ||
| Single | 46 | 66.08 ± 12.58 | ||
| Married | 148 | 71.33 ± 13.57 | ||
| Divorced/widow | 6 | 61.16 ± 12.79 | ||
| Access to healthcare services | 3.72 | 0.02 | ||
| Low | 19 | 64 ± 12.97 | ||
| Moderate | 109 | 68.91 ± 14.18 | ||
| High | 72 | 72.72 ± 12.26 |
aValues are expressed as mean ± SD.
bOne-way ANOVA
The results of the study concerning the relationship between health-promoting lifestyle and the variables in Pender’s health-promoting model suggested that health-promoting lifestyle had a significant positive relationship with perceived self-efficacy, perceived social support, and perceived emotions (P < 0.001), and a negative relationship with perceived barriers (P = 0.005). Perceived self-efficacy also had the highest correlation with the women’s health-promoting lifestyle (r = 0.56) (Table 3).
| Variable | Correlation (r) | P Value |
|---|---|---|
| Perceived self-efficacy | 0.56 | 0.001 |
| Perceived social support | 0.48 | 0.001 |
| Perceived emotions | 0.16 | 0.01 |
| Perceived barriers | -0.19 | 0.005 |
Multiple linear regression analysis was run to evaluate the predictors of a health-promoting lifestyle. The results showed that perceived self-efficacy was the strongest predictor of a health-promoting lifestyle (P < 0.001). In total, the three variables of perceived self-efficacy, perceived social support, and perceived emotions were able to predict 37% of lifestyle variations, and perceived barriers had no role in predicting lifestyle (Table 4).
| Predictor Variables | Non-Standardized Coefficients | Standardized Coefficients | t | P Value |
|---|---|---|---|---|
| B ± SD | Beta | |||
| Perceived self-efficacy | 1.17 ± 0.18 | 0.43 | 6.31 | 0.001 |
| Perceived social support | 0.26 ± 0.07 | 0.24 | 3.66 | 0.001 |
| Perceived emotions | 0.17 ± 0.08 | 0.11 | 1.92 | 0.05 |
| Perceived barriers | -0.04 ± 0.10 | -0.02 | -0.39 | 0.69 |
aR = 0.62; R2 = 0.38; adjusted R2 = 0.37; constant = 0.434; Durbin Watson = 1.92; F = 30.42; P < 0.001.
5. Discussion
The present study showed that the health-promoting lifestyle had a significant positive relationship with perceived self-efficacy, perceived social support, and perceived emotions and negatively correlated with perceived barriers. In other words, as perceived self-efficacy, perceived social support, and perceived emotions increase, people are encouraged to follow a health-promoting lifestyle. However, as perceived barriers increase, people are less likely to follow a health-promoting lifestyle.
It was also shown that of variables in the health promotion model, perceived self-efficacy, which refers to the evaluation and judgment of an individual about his/her ability to maintain or improve health is the most important factor for predicting health-promoting lifestyle among the women. This finding is in line with those of the studies that applied Pender’s health promotion model (27-29). Most studies that applied the health promotion model highlighted self-efficacy as the most effective factor in performing health-promoting behaviors (29, 30).
The results of the present study concerning the subscales of the health-promoting lifestyle showed that the women of the reproductive age had the highest score on nutrition and the lowest score on exercise, implying that they followed a satisfactory lifestyle in terms of nutrition but an undesirable lifestyle in terms of exercise. Similarly, Yarahmadi and Rousta (31) reported the highest score for nutrition and the lowest score for physical activity. Furthermore, Hosseinnejad and Klantarzadeh reported that students had a moderate score for nutrition but had a lower score for physical activity (32), as was observed in the present study. In contrast, Dukas et al. (33) showed that Spanish pregnant women followed a moderate nutritional style and an optimal physical activity style. Another study by Chen et al. (34) in Taiwan showed that pregnant women had a poor nutritional style and moderate physical activity, which is contrary to the observation made in the present study. It seems that these conflicting results are due to different cultural norms and lifestyles pursued by women in different countries.
The mean score of the women’s health-promoting lifestyle in the present study was lower than average, while the health-promoting lifestyle is an important determining factor in health (30). Yarahmadi and Rousta (31) reported the mean score of the health-promoting life scale as equal to 54 ± 12.80 (on a scale of zero to 100) that was at a medium to a high level. Besides, Lim et al. (11) reported that the score of the health-promoting lifestyle of the studied women was close to the mean score.
The present study showed that married women followed a significantly healthier lifestyle than single people, widows, and divorced people and scored higher on average. This finding is in line with Lim et al.’s study (11). Similarly, Ghaffari Nejad and Pouya (35) found that the highest score of health-promoting behaviors was gained by married people. Marriage seems to reinforce women’s sense of responsibility for choosing and following a healthier lifestyle.
The present study showed no significant relationship between age and lifestyle, as evidenced in some studies (35, 36). However, Singh et al. (37) and Al-kandari et al. (38) found a negative correlation between age and lifestyle, which can be due to differences in the samples under study.
Access to health services enables care, treatment, and prevention of diseases and is effective in improving a health-oriented lifestyle. Likewise, the present study showed the mean score of health-promoting lifestyle was higher in people who had high and very high access to health services than other groups. The type of study and individual, cultural, and social differences were the limitations of the study that could affect the quality of the participants’ responses.
5.1. Conclusions
The findings of the present study showed that the women’s lifestyle, physical activity, and health responsibility are not at favorable levels, and perceived self-efficacy, perceived social support, and perceived emotions were predictors of health-promoting lifestyle in the women of reproductive age and these three variables together predicted 37% of the variations in the health-promoting lifestyle score. Therefore, it is recommended that the necessary interventions and programs incorporating adequate training and information about health responsibility and regular physical activity be planned and implemented for women of reproductive age to improve the health-promoting lifestyle. Besides, given the lack of recreational and sports spaces for women in Sistan and Baluchestan Province and the importance of sports for a healthy lifestyle, related authorities must take effective measures to provide the required facilities. Given that the findings of this study highlighted the importance of self-efficacy in health-promoting lifestyles for women, health managers, and policymakers are required to design and implement effective training programs to increase women’s self-efficacy. Furthermore, considering that the findings of this study showed that social support is the second predictor of women’s lifestyle, and given the importance of interpersonal communication and social support in creating social capital and, consequently, improving women’s health, it is necessary to take effective measures to strengthen women’s support networks in the family and community.
