1. Background
Cancer is a group of diseases characterized by uncontrolled and abnormal cell growth and proliferation (1). Breast cancer is the second most often diagnosed cancer globally, with an estimated 2.1 million new diagnoses and about 627,000 deaths in 2018 (2). In Iran, breast cancer accounts for 16% of the total cancer cases and ranks first among all malignancies in women (3). Breast cancer is a biologically and clinically heterogeneous disease, with several recognized histotypes and molecular subtypes with different etiologies, profiles of risk factors, responses to treatments, and prognoses (4). People with breast cancer have an increased survival rate and live longer than those with other cancers but its complications and stress, can affect the psychological well-being of this group (5).
Cancer causes physical problems, such as hair loss or loss of a limb, psychological problems, such as anxiety, depression, post-traumatic stress, feelings of sadness, deprivation, and anger, family problems, and problems with psychological capital (6). Definitions of social capital depend partly on the source; however, social capital is generally regarded as resources that can be accessed from groups or networks to which individuals belong. It is further divided into individual and collective social capital. Psychological capital is one of the essential characteristics that make one adapt to difficult living conditions (7). Psychological capital has a positive and significant relationship with social capital (8). From an explanatory point of view, social capital takes precedence over psychological capital. Therefore, the lack of weakness of social capital leads to the isolation of the individual and negative individualism and ultimately leads to the weakening of psychological capital (9). Psychological capital enables people to cope better and more constructively in stressful situations, experience less tension, have higher capabilities when facing difficulties, achieve an enlightened view of themselves, and be less affected by daily events (10). Cancer patients have problems with the four components of psychological capital (11). The construct of hope is one's ability to set goals, visualize the necessary paths toward the goals, and have the necessary motivation to achieve the goals (12). Optimism refers to positive causal attributions and how people explain positive and negative events and expect a positive outcome. Resilience refers to one's capacity to respond to their abilities to perform a particular task (13). Self-efficacy is a measure of one's confidence in their ability to perform a series of actions, which is associated with one's adaptation to cancer (14). Kordan et al. in a study showed a positive and significant relationship between psychological capital and cancer patients’ resilience (15). Also, Rasouli Badrani et al. showed in a study that the components of psychological capital, namely optimism, self-efficacy, and resilience, had a significant positive relationship with quality of life in patients with breast cancer (16).
Researchers and clinicians have increasingly focused on attachment theory as a framework for studying illness and disease adjustment in recent years (17). Attachment insecurity is associated with difficulties in adapting to cancer (18). Attachment can be examined from two perspectives: the amount of value one has for themselves, and the amount of value one places on others. Among the introduced attachment styles (safe, anxiety, avoidance, and ambivalence), some experts believe that atmosphere and insecurity have a pathological basis (19). Research evidence after developing various attachment styles has concluded that adjoining behaviors can generally be considered one of the most vulnerable attachment styles (20). Studies have shown a positive and significant relationship between anxiety attachment and psychological disturbance in women with breast cancer (17, 21, 22).
Schema therapy is one of the treatments that has not been considered effective on psychological capital and vulnerable attachment in women with breast cancer. Schema therapy is an innovative and integrated method founded by Young and Behary (23). According to Stopa and Waters, psychological damage results from the formation and stabilization of early maladaptive schemas. It is hypothesized that childhood experiences of neglect or abuse can lead to early maladaptive schemas (24). The differences between schema therapy and traditional cognitive therapy include more emphasis on early childhood experiences, greater use of emotional techniques such as guided daydreaming, use of therapeutic relationships as a means to change, and longer treatment periods due to resistance. Khademi et al. found in a study that schema-based interventions were significant in the resilience of women with breast cancer (25). Moreover, Amiri et al. found in a study that schema therapy reduced rumination and depression in cancer patients (26).
Women with breast cancer experience anxiety and depression when dealing with diagnosis, prognosis, and treatment options. Cancer patients often develop negative thoughts after the onset of the disease, leading to various psychological disorders. According to cognitive approaches, the most important psychological factors affecting medical diseases are early maladaptive schemas that cause immune and disease changes. It seems that by intervening and performing schema therapy, the vicious cycle of incompatible schemas can be disrupted, contributing to the treatment process's effectiveness. As mentioned, one of the effective therapeutic approaches to reduce the psychological effects of physical illnesses is schema therapy (27). Schema therapy helps clients design and execute behavioral tasks to replace consistent behavioral patterns with inappropriate and ineffective coping responses. This, in turn, can increase happiness, improve mental health, and reduce physical problems in people with breast cancer (28).
2. Objectives
Given the above and epidemiological studies on the high prevalence of psychological disorders in cancer patients (29), this study aimed to investigate the effect of schema therapy on psychological capital and vulnerable attachment in women with breast cancer.
3. Methods
The research method was quasi-experimental with a pretest-posttest design and a control group. The statistical population included all women with breast cancer admitted to the Imam Khomeini Hospital, Tehran, Iran, from 23/07/2019 to 20/11/2019. Of the total population, 30 patients, according to statistics experts (30), were purposefully and accessibly selected and assigned to an experimental and a control group (each group with 15 women) based on a table of random numbers. The experimental group was exposed to schema therapy for 11 weekly 90-minute sessions, while the control group did not receive any training. The inclusion criteria were (1) diagnosis of breast cancer and exposure to chemotherapy; (2) no chronic diseases; (3) no problems and history of psychiatric diseases; (4) one to five years of illness; (5) age between 30 and 50 years; (6) ability to answer questions (no physical problem to fill out questionnaires); and (7) filling out the informed consent and residency form in Tehran. The exclusion criteria included (1) dissatisfaction with participation in research; (2) participating in another psychological intervention; and (3) absence from more than two consecutive sessions. Regarding ethical considerations, the necessary permission was obtained from the university and the vice chancellor for research to conduct the research, and the letter of introduction required to perform all the research steps was received. The information about how to perform was explained to the subjects, they can ask all their questions with enough time. They were assured that the information and results of the investigation would be kept strictly confidential by the project manager. The following three tools were used to collect data: information data (age, education, marital status, and history of disease), Luthans Psychological Capital Questionnaire, and Vulnerable Attachment Questionnaire.
3.1. Luthans Psychological Capital Questionnaire
Luthans Psychological Capital Questionnaire was used to measure psychological capital. The questionnaire consists of 24 items with four subscales of hope, resilience, optimism, and self-efficacy. Each subscale consists of six items, and each item is rated on a 6-point Likert scale (strongly disagree to strongly agree). To calculate the score of psychological capital, the score of each subscale is calculated, and the score of psychological capital is obtained from the sum of the subscales' scores. The minimum and maximum scores of items in the questionnaire are 24 and 144, respectively. Higher scores in the questionnaire show better mental health status. The confirmatory factor analysis results indicated that this test had factors and structures desired by the test manufacturers. Using factor analysis and structural equations, Luthans reported the ratio of this test to 24.6, which confirmed the factor validity of the test (31). The reliability of the questionnaire in Iran has been reported 0.87 based on Cronbach's alpha (32).
3.2. Vulnerable Attachment Questionnaire
A 22-item questionnaire was used by Bifulco et al. to assess the vulnerable attachment styles. The items of the questionnaire are rated on a 5-point Likert scale (strongly disagree = 1 to strongly agree = 5). Scores in the questionnaire range from 22 to 110, with lower scores indicating more favorable mental states (33). Bifulco et al. documented this questionnaire's validity based on heuristic factor analysis and reported Cronbach's alpha of 0.82 and 0.67 and the retest reliability of 0.73 and 0.65 (33). In a study on 30 people, Cronbach's alpha for the questionnaire was 0.83. Subsequently, exploratory factor analysis was performed by rotating the varimax nugget (based on the answers of the study's final sample, which had a sample size of 345 people) based on principal components on 22 questions. Evidence showed that the questionnaire had favorable conditions for assessing the totality of vulnerable attachments (20).
3.3. Intervention
The therapist (a Ph.D. student) conducted weekly 90-minute schema therapy sessions for the experimental group under the supervision of supervisors and counselors according to the guidelines and tactics of Young’s schema therapy (34). It should be noted that this treatment package has been used in reputable studies such as Goli et al.’s (35), Khademi et al.’s (25), and Ansarishahidi’s studies (36). As shown in Table 1, a summary of the schema therapy sessions is provided.
Table 1.
Content Title of Schema Therapy Sessions
| Meeting | Goals Content | Goals Meetings |
|---|---|---|
| 1 | Introducing the intervention | Communication and empathy, how early maladaptive schemas are formed, schema functions, and maladaptive coping styles and responses |
| 2 | Pre-test run | Assessing the initial condition of the group and conceptualizing the patients' problem according to the schema-based approach |
| 3 | Defining schema therapy | Understanding the concepts of schema therapy and how to use it, its evolutionary roots, and areas |
| 4 | Training and recognizing early maladaptive schemas | Accurate and scientific learning of early maladaptive schemas, training, and practice of two cognitive techniques including a schematic validity test and a new definition of schematic confirming evidence |
| 5 | Introducing the areas of early incompatible schemas | Familiarity with the areas of incompatible schemas and their diagnosis and identifying disrupted areas of the relevant schema |
| 6 | Teaching and understanding the concept of cognitive coordination and dysfunctional coping responses | Recognizing ineffective coping responses with personal experiences and writing a schema registration form during daily life and when schemas are evoked |
| 7 | The scheme of assessing and training schema therapy | Recognizing and diagnosing maladaptive individual schemas to identify feelings toward parents and help release their blocked emotions |
| 8 | Using cognitive schema therapy strategies | Improving dysfunctional coping schemes and styles, finding new ways to communicate, and coping with avoidance, surrender, and extreme compensation |
| 9 | Using empirical schema therapy strategies | Changing and improving the emotional level of maladaptive schemas, performing imaginary dialogue, identifying unsatisfied emotional needs, and trying against schemas at the emotional level |
| 10 | Teaching patterning methods | Replacing healthy and efficient behaviors with inconsistent behaviors, mental imaging of problematic situations, and exercising healthy illustrative behaviors |
| 11 | Post-test run | Evaluating the effectiveness of schema therapy, overcoming barriers to behavior change, summarizing, and concluding |
In this study, descriptive statistical methods, such as mean and standard deviation, were used, and the Shapiro-Wilk test was used to check the normality of the distribution. The paired-samples t-test was used to compare the mean scores in each group before and after the intervention, the independent samples t-test was run to examine intergroup differences, and the chi-square test was used to compare the frequencies of the qualitative variables for the two groups. Also, SPSS-21 was used to investigate the assumption of homogeneity of variances from the Leven and Box test and analyze data from multivariate variance (MANCOVA).
4. Result
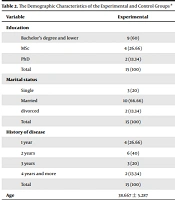
The mean age was 30 years in both experimental and control groups. The results of the independent samples t-test did not show any difference between the groups in terms of the patients’ age (P = 0.55). Also, an analysis of the patients’ demographic variables using the Fisher exact test indicated no significant difference between the groups in terms of education, marital status, and history of the disease (P < 0.05) (Table 2).
Table 2.
The Demographic Characteristics of the Experimental and Control Groups a
| Variable | Experimental | Control | P-Value |
|---|---|---|---|
| Education | 0.772 b | ||
| Bachelor's degree and lower | 9 (60) | 8 (53.33) | |
| MSc | 4 (26.66) | 5 (33.33) | |
| PhD | 2 (13.34) | 2 (13.34) | |
| Total | 15 (100) | 15 (100) | |
| Marital status | 0.807 b | ||
| Single | 3 (20) | 8 (53.33) | |
| Married | 10 (66.66) | 5 (33.33) | |
| divorced | 2 (13.34) | 2 (13.34) | |
| Total | 15 (100) | 15 (100) | |
| History of disease | 0.496 b | ||
| 1 year | 4 (26.66) | 7 (46.66) | |
| 2 years | 6 (40) | 4 (26.66) | |
| 3 years | 3 (20) | 2 (13.34) | |
| 4 years and more | 2 (13.34) | 2 (13.34) | |
| Total | 15 (100) | 15 (100) | |
| Age | 38.667 ± 5.287 | 38.600 ± 5.937 | 0.551c |
aValues are expressed as No. (%) or mean ± SD.
bFisher Exact test
ct-test.
The results of paired t-test showed a significant difference in the mean scores of the components of psychological capital and vulnerable attachment between the groups. Therefore, it can be stated that the effectiveness of schema therapy was associated with increased self-efficacy (P = 0.013), hope (P = 0.001), resilience (P = 0.034), optimism (P = 0.001), and decreased vulnerable attachment (P = 0.029) (Table 3).
Table 3.
The Comparison of Mean and SD of the Psychological Capital and Vulnerable Attachment Scores in the Two Groups Before and After the Intervention
| Variables | Before | After | P-Value a |
|---|---|---|---|
| Psychological capital | |||
| Efficacy | |||
| Experimental | 15.066 ± 0.883 | 19.400 ± 2.773 | 0.013 |
| Control | 15.333 ± 1.379 | 12.400 ± 2.414 | 0.091 |
| Hope | |||
| Experimental | 16.600 ± 1.352 | 21.066 ± 3.712 | 0.001 |
| Control | 15.133 ± 1.302 | 13.200 ± 1.567 | 0.203 |
| Resilience | |||
| Experimental | 17.666 ± 1.447 | 23.200 ± 3.447 | 0.034 |
| Control | 19.466 ± 1.302 | 15.866 ± 1.641 | 0.910 |
| Optimism | |||
| Experimental | 21.133 ± 1.552 | 26.553 ± 3.778 | 0.001 |
| Control | 20.466 ± 1.864 | 16.733 ± 2.658 | 0.213 |
| Total score | |||
| Experimental | 70.466 ± 2.614 | 88.933 ± 7.731 | 0.005 |
| Control | 70.400 ± 2.640 | 58.200 ± 4.783 | 0.403 |
| Vulnerable attachment | |||
| Experimental | 94.666 ± 3.811 | 61.667 ± 8.440 | 0.029 |
| Control | 69.600 ± 5.138 | 76.866 ± 4.853 | 0.817 |
aPaired test
The Wilks' Lambda results showed that the effect of schema therapy was significant on at least one of the variables (Wilks' Lambda = 0.395, P < 0.01). Accordingly, by establishing the assumptions of Wilks' Lambda to control the significant effect of pre-test scores, it was shown that the mean scores of self-efficacy (P = 0.009), hope (P = 0.021), resilience (P = 0.025), optimism (P = 0.010), and vulnerable attachment (P = 0.020) were significantly different after the intervention in the groups (Table 4).
Table 4.
The MANCOVA Analysis Results Regarding the Effect of Schema Therapy on Psychological Capital and Vulnerable Attachment
| Source | Dependent Variable | df | Mean Square | F | P-Value | Effect Size | Observed Power |
|---|---|---|---|---|---|---|---|
| Pre-test | Efficacy | 1 | 6.31 | 1.05 | 0.31 | 0.04 | 0.16 |
| Hope | 1 | 1.74 | 0.21 | 0.64 | 0.00 | 0.07 | |
| Resilience | 1 | 2.49 | 0.38 | 0.54 | 0.01 | 0.09 | |
| Optimism | 1 | 0.44 | 0.04 | 0.83 | 0.03 | 0.05 | |
| Vulnerable Attachment | 1 | 1.31 | 0.03 | 0.84 | 0.00 | 0.14 | |
| Group | Efficacy | 1 | 48.335 | 8.043 | 0.009 | 0.259 | 0.77 |
| Hope | 1 | 50.242 | 6.141 | 0.021 | 0.211 | 0.66 | |
| Resilience | 1 | 37.521 | 5.710 | 0.025 | 0.199 | 0.62 | |
| Optimism | 1 | 77.804 | 7.870 | 0.010 | 0.255 | 0.76 | |
| Vulnerable Attachment | 1 | 295.756 | 6.256 | 0.020 | 0.214 | 0.66 |
5. Discussion
This study aimed to evaluate the effect of schema therapy on psychological capital and vulnerable attachment in women with breast cancer. Based on the first finding of this study, schema therapy promotes psychological capital and its components (self-efficacy, hope, resilience, and optimism) in women with breast cancer. This finding is consistent with the results of research by Khademi et al. (25), Carmona-Halty et al. (37), Luthans and Youssef-Morgan (38), and Videler et al. (39). Khademi et al. found in a study that schema-based interventions were significant in the resilience of women with breast cancer (25). Also, Amiri et al. found in a study that schema therapy reduced rumination and depression in cancer patients (26).
Research has shown that psychological capital can be used to treat mental illness, increase hope, mental effort, and resistance, strengthen the defense force, and increase the level of psychological well-being (40). Since the components of psychological capital cover most aspects of life, it is predicted that people with breast cancer will have problems in this area, and their rate of psychological capital will be much lower than that of normal people. A schema is a memory package whose content is shaped by one's teachings over time. Factors, such as the biological foundations of individuals, and factors related to their educational environment, such as family, culture, growing experiences, and major events, affect the emergence of schemas. According to Mami and Safarnia, early maladaptive schemas are emotional and cognitive patterns of self-harm formed in mind at the beginning of growth and development and continue throughout life. Early maladaptive schemas have opposite characteristics. They are deep and pervasive patterns or themes composed of memories, emotions, cognitions, and bodily feelings. They are formed in childhood and adolescence, continue throughout life about oneself and the relationship with others, and are very inefficient (41). It can be concluded that the purpose of schema therapy is to help one better meet their basic emotional needs. Schema therapy helps the therapist to define the chronic and profound problems of breast cancer patients and to correct it in a comprehensible way.
Based on another finding of the present study, schema therapy improves vulnerable attachment in women with breast cancer. This finding is consistent with the results of Masoodi et al. (42). They found a significant relationship between attachment styles and death anxiety through the mediation of early maladaptive schemas in cancer patients. They also realized that early maladaptive schemas as a mediating variable could affect the relationship between attachment styles and death anxiety (42). Therefore, combining psychological interventions to change unhealthy behavioral patterns and consulting with psychologists to identify and modify early maladaptive schemas and essential physical therapies can effectively reduce psychological trauma in cancer patients.
Safe people usually do not experience rejection when their parents are satisfied with their security and social connection. They perform independently to separate from the family, and by having a sense of responsibility toward others or an orientation toward long-term life goals, they set goals and achieve realistic goals. People with a secure attachment style will cope better with this stressful situation and have fewer psychological problems due to the lack of early maladaptive schemas. Young et al. believe that such people suffer from more maladaptive schemas (34), causing anxiety in them. In this regard, Camara in a study showed that the formation of defective schemas causing rejection, self-harm, following, and guidance by others led to symptoms of anxiety and depression in people with vulnerable attachment. This can have a very devastating effect on one's physical and mental health (43). Schema therapy works to change this distorted cognition to make one's self-knowledge, environment, and future in line with reality. In other words, through schematic therapy, we can change our cognition and improve attachment relationships that completely make clear progress in knowledge of ourselves, the environment, and the future. Measuring people's attachment and implementing training programs can improve people's level of mental well-being, make their social relationships more meaningful, and motivate them to live happier lives (44).
According to the research background and the findings of the present study, showing that schema therapy has a significant effect on improving attachment, it can be concluded that schema therapy targets early maladaptive schemas, fundamental beliefs, feelings, emotions, childhood memories, and adolescence, and that relationships with others improve social adjustment and eliminate attachment damage.
Considering that the statistical population of the study of all women with breast cancer admitted to the Imam Khomeini Hospital, Tehran, Iran, from 23/07/2019 to 20/11/2019. So it is possible to generalize the results to the entire population of women with breast cancer it comes with restrictions. Another limitation of this research was related to measurement; these reports are prone to distortion due to unconscious defenses, bias in response, methods of personal introduction, and social desirability, in general. It is suggested to perform this study on a wider sample of individuals and in other centers. Also, considering that the present study is quantitative in nature, it is suggested to use qualitative research (contextual theory based on semi-structured interviews) based on clients' opinions, experts’ opinions, and previous literature.
5.1. Conclusions
Based on the findings of this study regarding the effect of schema therapy on improving psychological capital and reducing vulnerable attachment, it can be concluded that schema therapy can be used as an effective intervention along with other therapies in reducing the problems of women with breast cancer. Therefore, it is recommended to implement schema therapy to improve clinical nursing practice.


