


1. Background
Activities of daily living (ADL) include activities and tasks that patients must be capable of living independently (1). Chronic obstructive pulmonary disease (COPD), a life-threatening chronic inflammatory disease of the lungs, significantly impacts patients' ADL (2, 3). Chronic obstructive pulmonary disease, with 212.3 million (200.4 – 225.1) prevalent cases, was the primary cause of deaths from chronic respiratory diseases (CRD), accounting for 3.3 million (2.9 – 3.6) (4). It is estimated that COPD will become the fourth most common cause of morbidity and mortality worldwide by 2030 (5).
Chronic obstructive pulmonary disease is the major cause of chronic morbidity and will rank 7th in the global burden of diseases in 2030. The estimated prevalence of COPD is 4 - 20% worldwide in adults over 40 years of age and 6.3% in the Asian population (6). Dyspnea represents the most important symptom in COPD patients affecting ADL (7, 8). The reduction of performed ADL is among the most significant implications of COPD progression (9, 10). Insufficient physical activity has been found to be a major cause of disability, decreased lung function, early morbidity and mortality (11), dyspnea, and exacerbation of disease in COPD patients (12).
Limitations of ADL are well-known in COPD patients; however, its severity, types, and causes are not yet comprehensively understood (13). A lack of a consensus regarding the concept of ADL in COPD patients causes problems in their measurement, scientific communication, comparison of results of studies, data retrieval, and synthesis of findings (14-16). Concept analysis represents a group of methods for clarifying and understanding concepts that have multiple applications and vague meanings more comprehensively (17). An analysis of the concept of ADL in COPD patients will certainly contribute to a more in-depth understanding of its definition and attributes.
2. Objectives
Considering the applications of the ADL concept in the clinical care of COPD patients, the purpose of the present study was to describe the current conceptualization of ADL in COPD patients in the literature and compare findings from the literature and patient-based ADL descriptions to achieve an in-depth and comprehensive definition of ADL in the social and cultural context of Iranian patients with COPD.
3. Methods
3.1. Study Design
A number of different approaches have been developed to perform a concept analysis. The scope of interest and the aim behind the analysis are the most important determinants in adopting an approach (18). For this study, we adopted the three-step hybrid concept analysis that seemed to be well suited to the purpose of this study. The inclusion of the patient's perspective provided the opportunity for a more patient-centered definition of the concept. The hybrid concept analysis consists of three phases: The theoretical phase, the fieldwork phase, and the final analytical phase (19).
3.1.1. Theoretical Phase
In the theoretical phase, the literature was reviewed using an integrative review method to identify conceptual and operational definitions of ADLs in COPD patients (18). Articles about ADLs in COPD patients published in English within 2000 and 2022 were retrieved by searching international and national online databases, such as Web of Science, MEDLINE, Google Scholar, Science Direct, Elsevier Cochrane, PubMed, ProQuest, and CINAHL using the keywords: ‘chronic obstructive pulmonary disease’, ‘COPD’, ‘activity of daily living’, ‘ADL’, ‘activities of daily living’, ‘day to day activities’, ‘daily life activities’, ‘daily activities’, and ‘physical activity’ (15).
The inclusion criteria included being related to the definition of ADLs in COPD patients and being published in a peer-reviewed journal. The search yielded 676 articles. After eliminating duplicates, 593 articles remained for review. Their titles and abstracts were reviewed and were selected if the focus of the article was on ADLs in COPD patients. As a result, 178 articles were retrieved and read in full. Fifty-six articles were finally selected and used for the purpose of this phase. Data analysis was performed as the textual content analysis (19). The authors read each article and identified words and phrases that stood for attributes of ADLs in COPD patients. Then, the identified words and phrases were arranged in descending order according to frequency to reveal the attributes of ADLs in COPD patients. Finally, the attributes of ADLs in COPD were categorized according to similarities and differences. The MAXQDA10 software package was used for data management. At the end of this phase, a working definition was developed. After an extensive review, the fieldwork phase was initiated. During the fieldwork phase, empirical observation and continual review of the literature were conducted (18).
3.1.2. Fieldwork Phase
In the fieldwork phase, participant observation and in-depth interviews were used to develop insight and explore the nature of ADLs in COPD patients. Exploration in the fieldwork phase included the empirical validation of the preliminary concept developed in the theoretical phase by using a content analysis approach (20). Eighteen participants were recruited by a purposeful sampling with the maximum variation sampling to achieve representative variation in patient gender and educational level, in addition to severity and duration of COPD, from the National Research Institute of Tuberculosis and Lung Diseases (NRITLD), a university hospital located in Tehran, Iran, which represents a referral center for COPD. The majority of participants were male (n = 12, 66.6%). The mean age of the participants was 71.6 ± 7.2 years, and the mean duration of the disease was 8.6 ± 4.3 years. Moreover, 50% of the participants were married, and 61.1% were illiterate. In addition, 44.4% lived alone.
The inclusion criteria were a diagnosis of COPD as defined by the Global Initiative for Chronic Obstructive Lung Disease and consent to participate in the study. The data were collected via a semi-structured interview, in which the participants were encouraged to talk freely. The interview was composed of three open-ended questions, which were selected based on the literature review. The interview questions were designed with regard to the participants’ definitions of the concept of ADLs and were as follows:
‘Would you please describe the activities that you do on a typical day?’
‘Do your breathing problems limit what you like to do in your daily life?’
The first author performed all interviews in the participants' homes. The interviews lasted between 30-60 minutes, and each interview was audiotaped. The data were analyzed within 48 hours of the interview. Based on the data analysis, further probing questions were asked until data saturation occurred and a detailed description of ADLs in COPD was obtained. The data collection was stopped after 18 interviews because it was apparent that no new themes or statements had emerged after the 17th interview. The field observational notes were also transcribed, and the contents of those transcripts and the interview transcripts were analyzed via a conventional content analysis approach. The MAXQDA10 software package was used to identify and classify categories within the data. Each transcript was read, and condensed meaning units were labeled with a code; then, codes were compared based on similarities and differences and sorted into subcategories (19). Finally, subcategories were transformed into categories according to their similarities and differences.
3.1.3. Final Analytical Phase
In the final analytical phase, definitions derived from the first two phases were combined.
3.2. Trustworthiness
Trustworthiness is among the most important issues in qualitative approaches. Confirmability, credibility, dependability and transferability according to Lincoln and Guba (19) have been applied. To ensure credibility, member checking was used. Peer checking was applied for confirmability of the data. An expert in qualitative research reviewed all transcripts and categories; in case of disagreement, further explanation and clarification were provided to reach a consensus. In addition, purposive sampling was used to facilitate transferability of the inquiry.
3.3. Ethical Considerations
The head of the Department of Nursing (Project No.902501003) and the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Tehran, Iran) approved the study (IR.USWR.REC.1393.244). Written informed consent was obtained from all participants before participation in the investigation.
4. Results
4.1. Review of Literature: Theoretical Phase
4.1.1. Characteristics and Definition of Concept
Activity is considered one of the most important signs of health and has been used as an index for outcome assessment in clinical studies since 1970 in healthcare disciplines (21). Physical activity is defined as movement generation by the musculoskeletal system, which requires more energy consumption than maintaining a resting position (22). Daily physical activity is defined as the actual level of physical performance of a person in the course of their daily living (23). Activities of daily living include the most important activities that an individual must be capable of performing in order to be able to live independently (9).
According to Mlinac and Feng (24), ADLs include taking care of oneself and one’s surrounding environment, moving around the house and within the community, playing social roles and personal activities, such as communication with others, having fun, maintaining a presence in the society, playing an active role in life, and maintaining a sense of self-satisfaction and wellness. Pashmdarfard and Azad (25) classified ADLs into three groups: Basic ADL (BADL), instrumental ADL (IADL), and advanced ADL (AADL). Basic ADL includes personal care; instrumental ADL includes cooking, household chores, and shopping; advanced ADL includes voluntary activity affected by cultural and motivational factors, which indicate satisfactory activities beyond independence. These three types of ADLs encompass all possible ADLs in one’s life. A review of the literature resulted in the identification of three attributes of ADLs in COPD: The complexity and multifactorial nature of activity, the effects of dyspnea, and changes in daily activity patterns (Table 1).
| Attributes | Literature Review |
|---|---|
| Complexity and multifactorial nature of activity | ‘Some combination of physiologic, symptomatic, and psychosocial factors influence performance in individuals with COPD’ (26, 27). |
| ‘The variation in functional performance observed in individuals with COPD is perplexing’ (28). | |
| Effect of dyspnea | ‘Dyspnea was the main reason to stop ADL’ (29). ‘Dyspnea is a complex multifactorial and highly personalized sensory experience’ (30). |
| Change in pattern of daily activity | ‘Patients with COPD had higher sitting time and lying time’ (31). |
| ‘COPD patients spend less time standing and walking in daily life than healthy elderly individuals’ (32). |
Attributes of Activities of Daily Living (ADLs) in Chronic Obstructive Pulmonary Disease (COPD) Patients in the Theoretical Phase
The first attribute of ADLs in COPD patients is the complexity and multifactorial nature of activity. In passive communities, such as COPD patients, economic, social, and cultural factors play different roles in determining activity levels, compared to healthy individuals (26, 27). Differences in their activity level can neither be sufficiently justified by clinical and anthropological factors nor by the difference in severity of disease (27). Some patients in advanced stages of COPD are capable of performing all ADLs; however, others with mild or moderate-severe symptoms become homebound (28). Clinical parameters, such as the level of airway obstruction, the distance walked within 6 minutes, or the degree of dyspnea, can only partly determine the level of physical activity of COPD patients (7). Additionally, some authors believe that reduced daily activity in COPD patients does not necessarily imply a decreased pulmonary function; it includes a combination of behavioral components (33), physiological factors (e.g., age and sleep) (34), psychosocial factors, and symptomatic disease (35, 36).
The effect of dyspnea was the second attribute of ADLs in COPD patients. Exertional dyspnea is the most common complaint among COPD patients (29, 37), and most complaints of COPD patients are related to dyspnea (29). It affects all dimensions of life and the general health of these patients (38) and is a complex and multifactorial phenomenon with physiological, mental, and social components. It is an irritating and frightening symptom for patients, which is highly subjective, and only patients can determine its severity. Dyspnea is the most important cause of reduced ADLs in COPD patients (9). It can cause fatigue, mood swings, reduced patient tolerance of activity, change in the individual’s perception of health, depression, and eventually reduced ADLs (8, 39). Moreover, as COPD advances, dyspnea is exacerbated when performing ADLs; therefore, patients become anxious and scared of activity. Patients’ fear of dyspnea and coughing during activity results in reduced ADLs; consequently, patients can become reluctant to perform any activity (30).
The third attribute of ADLs in COPD patients was a change in the pattern of ADLs. As the disease advances, patients' dyspnea during activity becomes worse, and performance of physical activity becomes harder (8, 29). As a result, patients gradually cut down or quit some of their daily activities. Some ADLs, such as fun and leisure activities, are among the first activities that are cut down or quit because these activities can require more energy than other activities and are not as important as other activities in life (31).
4.1.2. Working Definition of ADLs in COPD Patients (Theoretical Phase)
Activities of daily living in COPD patients are complex and multifactorial and are influenced by dyspnea and factors affecting it. Changed patterns of activity in these patients lead to an elimination or reduction of some activities.
4.2. Participant Observation and In-depth Interviews: Fieldwork Phase
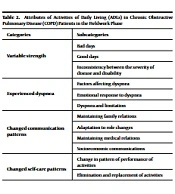
The attributes of ADLs in COPD patients obtained in the fieldwork phase included variable strength, experienced dyspnea, changed communication patterns, and changed self-care patterns (Table 2).
| Categories | Subcategories |
|---|---|
| Variable strength | Bad days |
| Good days | |
| Inconsistency between the severity of disease and disability | |
| Experienced dyspnea | Factors affecting dyspnea |
| Emotional response to dyspnea | |
| Dyspnea and limitation | |
| Changed communication patterns | Maintaining family relations |
| Adaptation to role changes | |
| Maintaining medical relations | |
| Socioeconomic communications | |
| Changed self-care patterns | Change in pattern of performance of activities |
| Elimination and replacement of activities |
Attributes of Activities of Daily Living (ADLs) in Chronic Obstructive Pulmonary Disease (COPD) Patients in the Fieldwork Phase
The first attribute of ADLs in COPD patients was variable strength. The physical condition of COPD patients might not change for several consecutive days. Patients divide their days into capability and disability days. Disability days are the days when patients are not capable of performing any activity; however, on capability days, patients are capable of performing many tasks.
“Some days, I cannot even pick up a matchstick.”
Patients have variable physical and emotional strength, fatigue, and psychological function levels on different days.
“Some days, I do not want to see anybody, not even myself.”
Some patients with more severe disease reported relatively higher activity. However, some with milder disease reported relatively lower activity and higher disability. For example, a 74-year-old male with stage COPD III reported hiking every weekend and exercising in a park every weekday with his peers.
The second attribute was that experienced dyspnea not only affects ADLs in COPD patients but is also a part of their ADLs. Dyspnea is very frightening for patients and can create a sense of impending death. Fear of a dyspnea attack indirectly inhibits the patient from attempting many activities. One participant said:
“I always suffer from dyspnea. When eating, when taking a shower ... all the time.”
On the other hand, there are some factors and situations that definitely cause dyspnea or affect it, such as climbing uphill, using stairs, and some emotional situations.
“When my grandchildren are coming to visit me, I totally forget about my dyspnea…. I start cooking for them.”
Patients believe that several factors affect the occurrence of dyspnea, such as air pollution, hot or cold weather, and frustration and anxiety.
“My dyspnea becomes much worse when the air pollution is high.”
The third attribute of ADLs was a change in their patterns of communication. Patients often recognize the importance of family relations after they become severely ill. One participant said:
“I only get out of bed for the sake of my sons.”
The role of a patient in their family as a spouse or parent or in their community changes after the onset of COPD. Patients often try their best to play their previous roles; however, they eventually cope with the change when they no longer have the strength or the energy to fulfill their previous roles.
“There are times that I cannot even park my car in the garage.”
Maintaining good communication with medical professionals helps them better control the disease and cope with the new situation. Some of them were still working despite their activity limitations in order to make money, prevent negative thoughts and a sense of futility, and remain in touch with individuals. One patient explained:
“I had a bakery, and I used to bake bread. But I cannot stay close to the oven now because my dyspnea aggravates. Therefore, I drive a cab now.”
Change patterns of self-care were the fourth attribute of ADLs. These patients try to simplify and slow down their ADLs. They reduce the intensity, level, and number of activity attempts in order to maintain their independence. One patient said:
“I have placed one chair in the kitchen and one in the bathroom. I sit on the chair and cook.”
The findings also revealed that the intensity of activity decreases in COPD patients. These patients walk slower than before for two reasons. One is to maintain their independence, and the second is to prevent dyspnea attacks and the associated limitations. Therefore, although COPD patients cannot be as active as they were prior to the onset of the disease, they tend to try their best not to be dependent on others. They often try to rest between activities. They also take their medications with them wherever they go. They live in places without stairs or with elevators and gradually learn to cope with their disability. They spontaneously cut down or eventually quit some of their activities and reserve their energy for more important tasks.
4.2.1. Working Definition of ADLs in COPD Patients (Fieldwork Phase)
Activities of daily living in COPD patients are affected by perceived shortness of breath and a continuum from relative ability to complete disability. Moreover, the pattern of communication and daily self-care in these patients has changed.
4.3. Final Analytical Phase: Integration of the Literature and Fieldwork
Based on the findings obtained from the theoretical and fieldwork phases, three attributes of ADLs in COPD patients were determined: Complexity and multifactorial nature of activity, dyspnea and factors affecting it, and trying to live normally and independently (Table 3).
| Theoretical Phase | Fieldwork Phase | Final Phase |
|---|---|---|
| Complexity and multifactorial nature of activity | Variable strength | Complexity and multifactorial nature of activity |
| Effect of dyspnea | Experienced dyspnea | Dyspnea and factors affecting it |
| Change in pattern of daily activity | Changed communication patterns | Trying to live normally and independently |
| Changed self-care patterns |
Categories of Activities of Daily Living (ADLs) in Chronic Obstructive Pulmonary Disease (COPD) Patients in the Final Phase
4.3.1. Practical Definition
Based on the attributes obtained in the final analytical phase, the following definition was obtained for ADLs in COPD patients: ADLs in COPD patients are complex and multifactorial and are affected by dyspnea and factors influencing it. The pattern of daily activities, communication, and self-care in COPD patients changes toward living normally and independently.
5. Discussion
In this study, three attributes were indicated for the concept of ADLs in COPD patients, including a complex and multifactorial concept, dyspnea and factors affecting it, and trying to live normally and independently. The complex and multifactorial nature of ADLs in COPD patients was an attribute found in both the theoretical and fieldwork phases. This finding is concordant with the results of previous studies. Hometowska et al. (35) showed that activity in COPD patients was affected by physiological and psychological factors and their complex interactions. The data from the fieldwork showed that some of the patients with relatively severe disease were more active than some of those with relatively mild disease. Moreover, differences in the activity levels of COPD patients could not be attributed solely to differences in disease severity (32). The variable strength of patients represents one expression of the complexity of the ADLs concept, and their strength can vary between days and on one single day. In a study by Scichilone (40), most patients stated that each day differed from the previous day in terms of both symptoms and activities.
"Dyspnea and factors affecting it" was the second attribute of ADLs in COPD patients derived from both theoretical and fieldwork phases. Dyspnea affects all aspects of COPD patients' life (8). Many complaints of COPD patients were closely related to dyspnea (29). Dyspnea is a subjective and cognitive concept (41). The present study showed that some patients with more severe disease had less dyspnea. Other studies revealed that dyspnea is a complex, multifactorial, and subjective concept and has a cognitive and subjective effect on activity (42, 43). When patients experience dyspnea, they notice that they are not well, and therefore, they reduce their ADLs; however, this reduction in physical activity further exacerbates their dyspnea and results in subsequent immobility (44). Moreover, dyspnea is affected by factors such as anxiety, depression, emotional and mood components (45, 46), and weather and climate changes (47, 48). Most patients believe that environmental and emotional factors, such as air pollution, cold weather, happiness, and anxiety, affect their dyspnea. Sharma et al. (49) showed that dyspnea was influenced by emotional and mood components.
Trying to live normally and independently was the third attribute of the concept of ADL in COPD patients. In the fieldwork phase, it was revealed that COPD patients not only reduced the intensity, level, and duration of their ADLs but also changed their method of performance. Furthermore, they cut down or eliminate unnecessary activities in order to save energy for other, more important activities. Patients make these modifications in order to maintain their independence. Chronic obstructive pulmonary disease patients have reduced self-care ability (50-52).
The final theme was the change in their patterns of communication. The results showed reductions in most social activities in COPD patients, which is in line with other studies (53, 54). Trying to live normally and independently means that although COPD patients deal with physical activity limitations, they try to continue to follow their routines. Chronic obstructive pulmonary disease patients try to preserve their energy and adapt to their new condition by lowering the level and intensity of their activities (55). Notably, however, it is not always good for a patient to pretend to be fine because COPD is not a visible disease. Therefore, others might not understand that the patient needs to rest or curtail their activities. This finding might lead to the patient’s exhaustion and induce a feeling of not being understood by others. It might also cause a feeling of insecurity with regard to their ability to perform ADLs.
5.1. Limitations
This study sought to clarify the concept of ADL in COPD patients. Since the majority of COPD patients are elderly and the prevalence of COPD is higher in males than in females, most patients in the current study were elderly males.
5.2. Conclusions
Many concepts, such as ADLs, do not have a widely agreed-upon definition despite years of common usage, and their use in different situations might not yield the same perceptions in different patients or healthcare professionals. This study sought to clarify and describe the concept of ADLs in COPD patients based on both previous studies and the perspectives of patients. It is imperative for the relevant healthcare professionals to have a correct understanding of the conceptual structure of ADLs in COPD patients. Moreover, by using the results of this study, attempts can be made to eliminate the obstacles involving ADLs encountered by COPD patients. The results of the current study might be useful for designing nursing models, developing theories and measurement tools, and increasing the capacity to perform ADLs in COPD patients. Such models can provide strong foundations for improved nursing care
