1. Background
Although the main purpose of nursing education is to reduce the gap between theoretical concepts and clinical practice, many nursing students with a good theoretical background do not have sufficient skills in the clinical environment and cannot use problem-solving skills for creative performance (1, 2). Problem-based learning (PBL) is a structured, student-centered and active strategy that can help students apply science and skills in new situations (3). The PBL strategy promotes students’ learning and helps them solve real-life problems by seeking scientific information (4). According to the literature, the concurrence of using PBL with team-based learning (TBL) is more effective (5, 6).
TBL engages students in goal setting and problem-solving (7). So, the audience actively participates in the learning process instead of inactive presence in teacher-centered methods (8). This strategy increases students’ interest in team working, and enhances their critical thinking (9). Time constraints, the difficulty of team management, and the lack of participation of shy students in the discussion have been listed as the disadvantages of team-based learning; however, they can be solved using virtual social networks (10). Today, there is great potential for using collaborative web platforms that allow online groups to be created, and health ideas, advice, and experiences can be shared (11).
For example, researchers indicated the use of Twitter has been successful to disseminate public health and emergency information and predict disease outbreaks (12, 13). Free et al. stated smartphones and apps have promising and exciting roles in enhancing medical education, patient care, and communication (14). Other authors confirmed that smartphones enhance the nursing students’ knowledge and practice by sending video anytime and anywhere (15). Also, the usefulness of educational video clips to improve communication skills and emotional intelligence, and clinical competence were confirmed in a quasi-experimental study (16). For the last case, we can mention a study in Iran that pointed out the positive effect of virtual education on students’ metacognitive self-regulation as well as attitudes (17).
All of these studies showed that using new teaching methods and technologies can help to better outputs in education aspects. However, it is necessary to do more researches. To the best of our knowledge, there was not a study that measured the impact of team-based education on clinical skills and problem-solving perception through social networking apps in nursing students. Therefore, our study is the first one that investigated the effect of virtual team-based education on the acquisition of clinical skills and problem-solving skills in nursing students.
2. Methods
2.1. Study Design
It was a quasi-experimental study with pretest-posttest design that investigated the effect of implementing a team-based educational program through virtual social networking apps on nursing students’ clinical skills and problem-solving ability in Fasa University of Medical Science, Fasa, Iran.
2.2. Participants
The inclusion criteria for the participants were being a nursing student who did not pass the Post CCU and CCU Internships, having a smartphone, and willingness to participate in the study. Exclusion criteria included non-attendance at all training sessions and current psychological symptoms that may impair participants’ attendance in training sessions and assessment. The total sample size was calculated to be 60 participants according to the 95% confidence interval, 80% test power, and 0.8 effect size in the study of Naderi et al. (17) with a 20% attrition rate. Then, 30 participants were assigned to each group by a convenience sampling method.
2.3. Intervention
The educational content was selected according to the nursing internship curriculum in the CCU and post-CCU wards, which includes all emotional, cognitive, and psychomotor domains. Students in the control group received only routine training. Students in the experimental group received team-based learning in addition to routine training, they were also members of Telegram groups that had access to training online. The Telegram group was created due to students could access educational materials at any time and share what they had learned. Team-based learning (TBL) steps in the experimental group are displayed in Table 1 in detail. This training included the following:
(1) Emotional domain: Teaching effective methods of communication with classmates, the patient, and his family and supporting the patient to make decisions about treatment and self-care.
(2) Cognitive domain: Identifying and diagnose critical situations and selecting appropriate solutions to deal with these situations.
(3) Psychomotor domain: Suitable clinical performance in different conditions and working with the devices and equipment available in the ward.
Table 1.
Team-based Learning (TBL) Steps in the Experimental Group in Detail
| Goals | Content | Teaching Methods | |
|---|---|---|---|
| Phase 1 | |||
| Pre-class study | Preparation | The topic of each session according to the education curriculum was provided to the students, and the student was required to review the topics before the start of the class and get prepared. | Student-centered; cooperative learning |
| On the first day of the internship, groups of three were formed, and students in each group were asked to make a video on how to use medical equipment and issues in the CCU ward and to set them in the telegram group according to schedule. | |||
| Phase 2 | |||
| Individual readiness assurance test (iRAT) | Diagnosis; feedback | At the beginning of every internship day, an individual test was taken from all students based on educational content in every day. | Inquiry-based learning; cooperative learning |
| Team readiness assurance test (tRAT) | Immediately after the individual tests, students were asked to take the same test as a group. Questions were asked in the telegram group, and students shared their answers. | ||
| Team appeals | Students were allowed to refer to the book about their arguments and leave their answers in the form of text, photos, or videos in the telegram group and request an appeal of their answers. | ||
| Feedback | The instructor provided feedback to the students, and further controversial questions were discussed. The instructor showed feedback to the students both through the web and in the ward. | ||
| Phase 3 | |||
| Application-oriented activity | Application of course concepts | Putting case-based scenarios in the Telegram group for increasing opportunity to discuss among groups, share the best diagnosis, treatment, or care by students to improve problem-solving skills in them. | Cooperative learning; problem-solving learning |
2.4. Study Instruments
According to the purpose of the study, three forms were used to collect data, the first part of which included a demographic data form (age, sex, marital status). The second part was a 17-item researcher-made questionnaire that measured clinical skills, and the third part was the 35-choice Heppner’s Problem-Solving Inventory (P.S.I.) (18).
The clinical skills questionnaire is evaluated students’ clinical performance in three domains of learning related to special cardiac wards including cognitive, affective, and psychomotor. Cognitive domain questions include recognizing the symptoms of heart disease, diagnosing common heart dysrhythmias, and planning for patient care. Items of affective domain included meeting the patient's emotional needs, the ability to communicate effectively with the patient, and self-confidence in doing performance. The psychomotor domain’s questions included doing proper nursing care, working with various devices in the ward, and following up the patients’ needs. The content validity of the clinical skill questionnaire was calculated by the content validity index using the opinions of 10 faculty members, the value of which was 88%. The reliability of this questionnaire was confirmed using Cronbach's alpha coefficient, and 0.89 was achieved. Clinical skill questionnaire items were scored on a Likert scale from 1 to 5 (strongly disagree 1, relatively disagree 2, no comment 3, relatively agree 4, strongly agree 5) with a scoring range of 17 to 85.
Heppner’s Problem-Solving Inventory has been used in various studies and has shown acceptable reliability in independent samples and different cultural groups (19, 20). This tool includes three factors of problem-solving confidence, approach-avoidance style, and the factor of personal control (18). In this study, the content validity of this questionnaire was determined by the content validity index using the opinions of 10 faculty members, the value of which was estimated at 86%. The Cronbach's alpha coefficient was 0.93 for the whole Problem-Solving Inventory, 0.85 for the problem-solving confidence factor, 0.89 for the factor of approach-avoidance style, and 0.73 for the personal control factor. This Questionnaire's items were graded on a Likert scale from 1 to 5 (strongly disagree 1, relatively disagree 2, no comment 3, relatively agree 4, strongly agree 5), and the score range was 35 to 175.
2.5. Data Collection and Analysis
At first, the questionnaires were given to the trainee students of the two intervention and control groups. While the control group routinely learned the necessary skills in PCCU and CCU, the intervention group also joined the Telegram online training group and received the training intervention in addition to routine training for four consecutive weeks. Follow-up data were also collected 12 weeks later. The interventions were designed so that it was not possible to communicate between the intervention and control groups at the time of the educational intervention. SPSS software version 24 was used for data analysis. A repeated measurement test was used to determine the difference in scores between the three periods at baseline and week four, and week 12 follow-ups, and paired t-test was used to analyze the differences between the groups.
3. Results
The participants included sixty nursing students (30 in the intervention group and 30 in the control group). Their average age was 21 ± 0.9 years. In the intervention group, there were 17 female and 13 male students, of which only three were married. In the control group, there were 16 female and 14 male students.
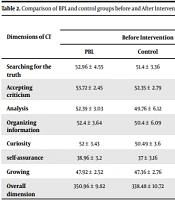
Independent t-test did not show a significant difference between the experimental and control groups in terms of problem-solving skills and clinical skills before the intervention, and the two groups were identical in terms of these variables (Table 2).
Table 2.
Comparison Between Mean Scores of Problem-Solving and Clinical Skills Before Intervention in Interventional and Control Groups a
| Variables | Mean ± SD | Levene's Test | t-test | |||
|---|---|---|---|---|---|---|
| F | P-Value | t | df | P-Value | ||
| Problem-Solving Inventory | 0.513 | 0.477 | -0.335 | 58 | 0.739 | |
| IG | 99.66 ± 19.44 | |||||
| CG | 101.30 ± 18.27 | |||||
| Clinical skills questionnaire | 0.081 | 0.777 | -0.292 | 58 | 0.771 | |
| IG | 46.96 ± 7.95 | |||||
| CG | 47.60 ± 8.78 | |||||
Abbreviations: IG, interventional group; CG, control group.
aSignificant at the level of P < 0.05.
In order to determine the effect of team-based training on problem-solving perception and clinical skills, a repeated measurement test was used, and the results showed that training caused a significant difference in total scores of clinical skills and problem-solving perception in the experimental group at baseline and week four, and week 12 of follow-up (Table 3).
Table 3.
| Baseline | Week 4 | Week 12 | Repeated Measurement ANOVA (Intra Group Differences) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mauchly's W | df | P-Value | Greenhouse-Geisser | F | P-Value | ||||
| Problem-Solving Inventory (total) | 99.66 ± 19.44 | 149.03 ± 7.24 | 113.76 ± 10.96 | 0.778 | 2 | 0.03 | 0.718 | 94.26 | < 0.001 |
| Problem-solving confidence | 31.80 ± 5.47 | 46.96 ± 3.02 | 35.16 ± 4.08 | ||||||
| Approach-avoidance style | 46.40 ± 10.87 | 67.46 ± 4.36 | 52.16 ± 5.84 | ||||||
| Personal control | 13.33 ± 2.72 | 21.70 ± 1.41 | 16.76 ± 2.38 | ||||||
| Clinical skills questionnaire | 46.96 ± 7.95 | 69. 03 ± 4.28 | 54.66 ± 5.95 | 0.665 | 2 | 0.003 | 0.749 | 146.97 | < 0.001 |
aValues are expressed as mean ± SD.
bSignificant at the level of P < 0 .05
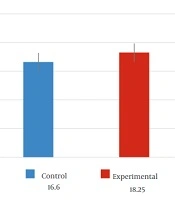
It is noteworthy that there was also a significant difference in the total score of clinical skills and problem-solving perception in the control group (Table 4). But the mean scores in the intervention group increased more than the control group (Figure 1).
Table 4.
| Baseline | Week 4 | Week 12 | Repeated Measurement ANOVA (With In-group Differences) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mauchly's W | df | P-Value | Greenhouse-Geisser | F | P-Value | ||||
| Problem-Solving Inventory (total) | 101.30 ± 18.27 | 133.86 ± 8.02 | 109.23 ± 8.43 | 0.778 | 2 | 0.002 | 0.730 | 53.62 | < 0.001 |
| Problem-solving confidence | 31.43 ± 6.80 | 41.73 ± 3.21 | 35.33 ± 2.90 | ||||||
| Approach-avoidance style | 47.63 ± 10.87 | 61.23 ± 4.45 | 48.86 ± 5.11 | ||||||
| Personal control | 14.50 ± 3.31 | 19.60 ± 2.72 | 15.16 ± 2.16 | ||||||
| Clinical skills questionnaire | 47.60 ± 8.78 | 61. 90 ± 8.11 | 51.30 ± 8.34 | 0.343 | 2 | < 0.001 | 0.604 | 57.17 | < 0.001 |
aValues are expressed as mean ± SD.
bSignificant at the level of P < 0 .05

Figure 1.
Average scores of clinical skills and Problem-Solving Inventory in the experimental and control groups
Table 5 indicates changes of the mean and standard deviation of the dimensions of Problem-Solving Inventory and clinical skills across the intervention and control groups in the baseline, from baseline to week four, and from baseline to week 12. The analysis shows that the total score of the Problem-Solving Inventory in the intervention group is greater than that of the control group from baseline to week four and from baseline to week 12 and the problem-solving confidence, approach-avoidance style, personal control for the intervention group is significantly greater than that of the control group. Particularly, the approach-avoidance style for the control group from baseline to week four was not significant as compared to intervention group scores (P = 0.389). It was shown that the scores four weeks after the intervention were higher than the baseline, i.e., before the intervention, and the scores 12 weeks after the intervention were higher than the baseline scores; therefore, the scores of both columns were negative. The difference between scores of four weeks after the intervention and 12 weeks after the intervention was positive, which indicated a higher score of four weeks after the intervention. These changes also existed in the control group but to a lesser extent.
Table 5.
| Variables | Change from Baseline to Week 4 | Change from Baseline to Week 12 | Change from Week 4 to Week 12 |
|---|---|---|---|
| Problem-solving confidence | |||
| IG | -15.16 ± 6.66 | -3.36 ± 6.23 | 11.80 ± 5.40 |
| P-value | < 0.001 | 0.006 | < 0.001 |
| CG | -10.30 ± 8.03 | -3.90 ± 7.25 | 6.40 ± 3.81 |
| P-value | < 0.001 | 0.006 | < 0.001 |
| Approach-avoidance style | |||
| IG | -21.06 ± 13.17 | -5.76 ± 13.03 | 15.30 ± 7.63 |
| P-value | < 0.001 | 0.022 | < 0.001 |
| CG | 13.60 ± 11.60 | -1.23 ± 10.03 | 12.36 ± 7.49 |
| P-value | < 0.001 | 0.389 | < 0.001 |
| Personal control | |||
| IG | -8.36 ± 2.98 | -3.43 ± 3.43 | 4.93 ± 2.97 |
| P-value | < 0.001 | < 0.001 | < 0.001 |
| CG | -5.10 ± 4.46 | -0.66 ± 4.17 | 4.43 ± 3.84 |
| P-value | < 0.001 | < 0.001 | < 0.001 |
| Total score of Problem-Solving Inventory | |||
| IG | -49.36 ± 22.95 | -14.10 ± 22.11 | 35.26 ± 14.78 |
| P-value | < 0.001 | < 0.001 | < 0.001 |
| CG | -32.56 ± 21.81 | -7.93 ± 18.76 | 24.63 ± 11.82 |
| P-value | < 0.001 | 0.028 | < 0.001 |
| Total score of the clinical skills questionnaire | |||
| IG | -22.06 ± 8.94 | -7.70 ± 5.54 | 14.36 ± 6.55 |
| P-value | < 0.001 | < 0.001 | < 0.001 |
| CG | -14.30 ± 9.59 | -3.70 ± 3.60 | 10.60 ± 8.27 |
| P-value | < 0.001 | < 0.001 | < 0.001 |
Abbreviations: IG, interventional group; CG, control group.
aValues are expressed as mean ± SD.
bSignificant at the level of P < 0 .05.
4. Discussion
The study demonstrated that significant improvements were created in nursing students’ clinical skills and problem-solving perceptions following virtual team-based training. The total score of the Problem-Solving Inventory and clinical skills of the intervention group was greater than that of the control group from baseline to week four and from baseline to week 12. This finding is consistent with the results of previous studies that have shown that team-based learning is an effective training strategy to increase problem-solving ability and improve clinical performance in nursing students (16, 21, 22). On the other hand, other researchers confirm a blended learning model, which includes online video resources, is a beneficial tool for teaching clinical skills to nursing students that not only strengthens students' knowledge and skills but also students can practice multiple times without worrying about mistakes in a non-judgmental learning environment (23-25). Mettiainen et al. explained that nursing students in the web-based groups shared their knowledge and experience, and progress in the clinical learning process simultaneously with each other by reflecting on their own experiences and those of others (26).
The present study also revealed that changes in approach-avoidance style, one dimension of problem-solving, were not significant in week four in the control group. This finding showed that routine training in week four had no effect on how to deal with the problem in the students in the control group. While students who have received team-based training through a smartphone application used the approach method when dealing with a problem and did not avoid facing a problem because consensus and sharing information in the virtual team has solved problems and answered questions in the shortest possible time. Burgess et al. believe that medical students in team-based learning have the opportunity to solve problems together and learn different perspectives on a patient (27). It seems that the way of dealing with problems in the students of the control group has not changed due to due to the stress of entering a new learning environment and the lack of opportunity to interact and share information with each other.
According to the results, the follow-up scores of week 12 decreased compared to week four. This finding indicates that the changes in the problem-solving ability and clinical skills of nurses fade over time; therefore, it is recommended that student training should be continued in person or online. Based on Liu et al.’s study, nurses’ knowledge and practice should be continuously developed, and that it is better to use smartphone training platforms to improve and sustain education (28).
A combination of routine clinical training and team-based training through smartphone applications is most influential in the improvement of nursing students’ clinical skills and problem-solving ability compared with routine training alone. This training method in internships provides students with the opportunity to share their experiences and feelings and help each other learn, regardless of time or place. This method of teaching can create an environment away from judgment and encourage students to participate in improving the level of clinical performance of each other. It is suggested that in the future, team training through smartphone applications will be used continuously in nursing students’ internship training.