1. Background
Acute respiratory infections (ARIs) lead to the illness, death, and hospitalization of millions of people around the world annually and can impose a heavy socioeconomic burden on communities (1). In Iran, ARIs have caused several disease outbreaks every year and made a large number of the country’s population to be hospitalized (2). Currently, the novel coronavirus, severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2), has caused acute respiratory infections called Coronavirus disease 2019 (COVID-19) in Iran and the world. The coronaviruses are important pathogens in humans and animals (3). In late 2019, a novel coronavirus was identified as causing a group of pneumonia cases in Wuhan City, Hubei Province, China (4). The novel coronavirus spread rapidly in China and around the world (5). On March 11, 2020, the World Health Organization (WHO) declared a COVID-19 pandemic outbreak (6). According to the WHO report, as of October 18 2020, there have been 39,596,858 confirmed cases of COVID-19, including 1,107,374 deaths (7). The novel coronavirus has imposed a great direct and indirect economic burden on the people and the health system. During the COVID-19 pandemic, the costs, including definitive diagnosis, intensive and general care beds, medicines and medical consumables, income loss due to premature death, economic production loss due to hospitalization, and job absenteeism have been added to the household budget and health system (8). The disease has also imposed heavy costs on the health system, most of which are the costs of bed days, including accommodation, food, and necessary care. In addition, the direct costs of COVID-19 in the health system comprise the provision of personal protective equipment for health care personnel, the supply of patients’ medicines, the provision of diagnostic kits, laboratory and radiology services, hospitalization and intensive care, the provision of the convalescent home and also the supply of items needed by hospitals (9). In recent years, determining the cost to achieve a clear picture of the cost trend and formulating the operating budget and effective use of resources have been considered from the perspective of health economics. Cost analysis as a management tool can help us provide the right data for making more informed investment decisions about actions and infrastructures (10). Although COVID-19 has affected all social, cultural, and political aspects of societies, its economic effects are mainly due to the implementation of social distancing and business closure plans as well as the reduction of the number of workers working in production centers more than other sections (11). In a cost-of-illness study, in January - March 2020, the economic burden of COVID-19 was estimated to be 0.62 US$ in China (12). In addition, it has been estimated that COVID-19 has caused financial impact of an average of 50.7 $ billion per month in lost income for America’s healthcare systems (13). There are several methods to determine the economic burden of diseases (10). The SDCA method is one of the modern methods that divides the costs into three categories (overhead, intermediate, and final costs) and separates the cost groups in each section into a suitable form for separating and recording the cost so that all costs in the overhead start with the intermediate and final wards with the costs of the intermediate wards then being divided into the final wards. Thus, the hospitals costs with any number of products can be calculated accurately and appropriately (14). In line with the prevalence of COVID-19 pandemic in the world and Iran, Qom Province was one of the provinces heavily affected by the disease (15).
2. Objectives
This study aimed to estimate the economic burden of COVID-19 infection in Qom Province, Central Iran, the SDCA method.
3. Methods
3.1. Data Collection
This descriptive, cross-sectional study was conducted on all COVID-19 patients (1,959 patients) in Qom Province over the time period from February 19, 2020, to June 19, 2020 with the first peak of the disease. The patients’ data were collected in the form of major cost groups (personnel costs, medicine, and medical supplies costs, administrative, health and treatment facilities costs, urban amenities costs, and building depreciation and physical spaces costs) registered in the integrated health system (IHS) that is a registration system of hospitalized patients together with the data accumulated by a piece of financial and accounting software called Roozamad, which is an accrual accounting system capable of extracting operating costs for goods or services (available at: [email protected]) used in Iranian Universities of Medical Sciences.
3.2. Ethical Considerations
Ethical approval was obtained from the Institutional Ethics Committee of Qom University of Medical Sciences (Qom, Iran) (IR.MUQ.REC.1399.128).
3.3. Statistical Analysis
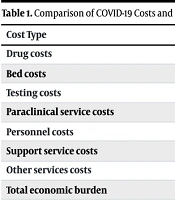
The major cost groups were divided into overhead, intermediate and final service departments. The data were collected in pre-designed tables, entered into Excel software and analyzed using SDCA in seven steps: (1) step 1, defining the final product included in this study for the treatment of COVID-19 patients who were referred to hospitals or hospitalized; (2) step 2: defining cost centers by identifying all service provider units and wards and sub-classifying them into three separate departments based on the SDCA method [Overhead Service Department; providing overhead support services to the intermediate and final service departments, Intermediate Service Department; providing support services to patient care units and organizing as separate, independent units and Final Service Department providing direct services to patients (Table 1)]; (3) step 3, identifying the full costs of each input (in this study major cost groups were considered); (4) step 4, assigning inputs to cost centers (Table 2); (5) step 5, allocating all costs to final cost centers; (6) step 6, computing total and unit costs for each final cost center; (7) step 7, reporting the results (14). Thus, the governmental, out-of-pocket, and opportunity costs paid by patients and hospitals in Qom Province in the specified time period (February 19 to June 19, 2020) were evaluated to calculate the economic burden using SDCA in Microsoft Excel 2010 software.
Table 1.
Classification of Service Provider Units and Wards Based on Overhead, Intermediate and Final Costs Associated with COVID-19 Cases in Qom Province, Central Iran
| Overhead Service Departments | Intermediate Service Departments | Final Service Departments |
|---|---|---|
| The headquarters of University of Medical Sciences | Emergency Departments | Internal medicine |
| Main office of provincial health center | Urban texture and suburban health posts | Intensive care units (ICU) |
| Head of hospital wards | Comprehensive health centers | Pre-hospital emergency medical service |
| Management of hospital wards | Pharmacy | - |
| Administrative affairs | Radiology | - |
| Financial affairs | Laboratory | - |
| Budget office | kitchen | - |
| Service office | Laundry | - |
| Facilities office | Other diagnostic centers | - |
| Vehicle office | - | - |
| Guard office | - | - |
| Hospitals warehouse | - | - |
| Admission | - | - |
| Discharge | - | - |
| Medical records department | - | - |
| Main office of food & drug administration | - | - |
| Main office of emergency | - | - |
| Others | - | - |
Table 2.
The Criteria for Allocating Inputs to Cost Centers (Overhead and Intermediate) for the Treatment of Patients with COVID-19 in the Hospitals
| Cost Centers | The Criteria For Allocating Inputs |
|---|---|
| Overhead Service Departments | |
| The headquarters of University of Medical Sciences | Portion of each center of the direct costs |
| Main office of Provincial Health center | Portion of each center of the direct costs |
| Head of Hospital Wards | Portion of each center of the direct costs |
| Management of Hospital Wards | Portion of each center of the direct costs |
| Administrative Affairs | Portion of each center of the direct costs |
| Financial Affairs | Portion of each center of the direct costs |
| Budget Office | Portion of each center of the direct costs |
| Service Office | Area/(m2) |
| Facilities Office | Area/(m2) |
| Vehicle Office | Number of staffs |
| Guard Office | Portion of each center of the direct costs |
| Hospitals warehouse | Portion of each center of the direct costs |
| Admission | Portion of each center of the direct costs |
| Discharge | Portion of each center of the direct costs |
| Medical Records Department | Portion of each center of the direct costs |
| Intermediate service departments | |
| Main office of food & drug administration | Portion of each center of the direct costs |
| Main office of emergency | Portion of each center of the direct costs |
| Others | Portion of each center of the direct costs |
| Emergency Departments | Number of missions |
| Urban texture and suburban health posts | Number of clients |
| Comprehensive health centers | Number of clients |
| Pharmacy | Portion of each section in the prescriptions |
| Radiology | Number of admissions |
| Laboratory | Number of admissions |
| Kitchen | Number of patients and staffs |
| Laundry | Number of patients |
| Other diagnostic centers | Number of patients |
In Table 2, to identify the criteria and calculate them, different criteria are adopted to allocate overhead and intermediate costs to the final center. A portion of overhead costs was first allocated to the intermediate and then to the final center, and another portion was directly allocated to the final center. If the metrics of the performance of overhead and intermediate activities were quantifiable, such as radiology films and the number of cooked foods, the metrics of overhead sector were directly calculated from HIS and the university’s performance accounting software, and the Rial-based performance was allocated to the final center. Moreover, issues related to management, chairmanship, etc. were determined by interviews, work assessment, and the analysis of conducted performances regarding COVID-19 management, treatment, and prevention. Afterward, their costs were calculated out of the overall direct costs and were directly allocated to the final center or, if related to the intermediate center, were first allocated to the intermediate center and then to the final center.
In addition, in another section of the study, the opportunity costs were also calculated in the study period. The opportunity costs equal the income that has been lost due to the change of income-generating beds to the new coronavirus diseases beds in Qom University of Medical Sciences in the study period. The change of income-generating beds mainly included the limited surgical, orthopedic, cardiac wars of hospitals (16). To have an international currency base, each dollar was considered equal to 250,000 Rials at the time of data collection in Iran.
4. Results
The incidence of COVID-19 infection was 518 per 100,000 populations in Qom Province from February 19, 2020 to June 19, 2020 (6,696 cases/1,292,283 populations). Also, 29.25% of the patients were hospitalized (1,959/6,696).
The total government costs for the treatment of patients with COVID-19 in the hospitals of Qom Province in this period were calculated to be 2,229,216,930,370 Rials (8,916,867 $) (Table 3). Among the major governmental cost groups, personnel and urban amenities accounted for the highest and lowest of total expenditures, respectively (Table 4). In addition, the results indicated that the out-of-pocket costs of patients and their families were 30,038,013,060 Rials (Table 5). Based on the SDCA method, the costs of the final service department, including internal medicine, ICU, and pre-hospital emergency medical service wards dealing with COVID-19 patients, accounted for more than 56% of the total cost (Table 4).
Table 3.
Major Cost Groups of Governmental Costs Associated with COVID-19 Cases in Qom Province, Central Iran, from February 19, 2020, to June 19, 2020
| Major Cost Groups | Total Cost; Rials ($) a | % Out of Total Costs |
|---|---|---|
| Personnel costs | 1,470,783,420,482 (5,883,133.68) | 65.97 |
| The cost of medicine and medical supplies | 297,813,684,888 (1,191,254.73) | 13.36 |
| Administrative, health and treatment facilities costs | 312,112,985,000 (1,248,451.94) | 14.00 |
| Urban amenities costs | 28,218,450,000 (112,873.8) | 1.27 |
| Building depreciation and physical spaces costs | 120,288,570,000 (481,154.28) | 5.40 |
| Total | 2,229,216,930,370 (8,916,867) | 100 |
a One dollar = 250,000 Rials.
Table 4.
Major Cost Groups of Governmental Costs Associated with COVID-19 Cases Based on Cost Departments in Qom Province, Central Iran, from February 19, 2020, to June 19, 2020
| Cost Departments | Major Cost Groups; Rials ($) a | |||||
|---|---|---|---|---|---|---|
| Personnel | Medicine and Medical Supplies | Administrative, Health, and Treatment Facilities | Urban Amenities | Building Depreciation and Physical Spaces | Total [%] | |
| Overhead service | 235,617,513,073 (942,470) | 48,056,605,044 (192,226) | 87,391,635,800 (349566) | 8,747,580,000 (34,990) | 34,601,869,800 (138,407) | 414,415,203,717 (1,657,660.81) [19] |
| Intermediate service | 371,695,855,121 (1,486,783) | 77,466,983,199 (309,868) | 74,907,116,400 (299,628) | 7,336,680,000 (29,347) | 26,745,580,200 (106,982) | 558,152,214,920 (2,232,608.86) [25] |
| Final service | 863,470,052,288 (3,453,880) | 172,290,096,645 (689,160) | 149,814,232,800 (599,257) | 12,134,010,000 (48,536) | 58,941,120,000 (235764) | 1,256,649,511,733 (5,026,598) [56] |
| Total costs [%] | 1,470,783,420,482 (5,883,134) | 297,813,684,888 (1,191,255) | 312,112,985,000 (1,248,452) | 28,218,270,000 (112,873) | 120,288,570,000 (481154) | 2,229,216,930,370 (8,916,867)[100] |
a One dollar = 250,000 Rials.
Table 5.
The Total Costs Associated with COVID-19 Cases in Qom Province, Central Iran, from February 19, 2020 to June 19, 2020
| Cost Groups | Costs; Rials ($) a | % of Total Costs |
|---|---|---|
| Governmental | 2,229,216,930,370 (8,916,867) | 83.20 |
| Opportunity | 420,000,000,000 (1,680,000) | 15.68 |
| Out of pocket | 30,038,013,060 (120,152) | 1.12 |
| Total | 2,679,254,943,430 (10,717,019) | 100 |
a One dollar = 250,000 Rials.
In this study, the opportunity costs were found to equal 420 billion Rials (15.68% of total costs) for COVID-19 patients in the hospitals (Table 5).
The total amount of governmental, opportunity, and out-of-pocket costs associated with patients hospitalized COVID-19 patients in Qom Province were found to be 2,679,254,943,430 Rials (Table 5). Besides, the total expenditure per capita of a patient with COVID-19 hospitalized for the government and the patients’ families was estimated as 1,367,664,596 Rials (5,470.65.5$) (Table 6).
Table 6.
The Total Costs Associated with Patients Hospitalized with COVID-19 in Qom Province, Central Iran, from February 19, 2020 to June 19, 2020
| Major Costs Groups | Treatment Care Costs | ||
|---|---|---|---|
| Total Costs of Cases; Rials ($) a | % Out of Total Costs | Expenditure per Capita; Rials ($) | |
| Governmental costs | 2,649,216,930,370 (10,596,867) | 98.88 | 1,352,331,256 (5,409.32) |
| Out of pocket | 30,038,013,060 (120,152) | 1.12 | 15,333,340 (61.34) |
| Total costs | 2,679,254,943,430 (10,717,019) | 100 | 1,367,664,596 (5,470.65) |
a One dollar = 250,000 Rials.
Finally, the costs per capita groups, including the mean cost per inpatient case, mean cost per case, and provincial per capita costs, were also evaluated (Table 7).
Table 7.
The per Capita Total Costs Associated with COVID-19 Patients in Qom Province, Central Iran, from February 19, 2020, to June 19, 2020
| Costs per Capita Groups | Costs Rials ($) a |
|---|---|
| Mean cost per inpatient case | 1,367,664,596 (5,470.65) |
| Mean cost per case | 395,641,716 (1,582.56) |
| Provincial per capita costs | 2,050,029 (8.20) |
a One dollar = 250,000 Rials.
5. Discussion
It seems that research on the economic consequences of a disease imposed on patients, families, and society is inevitable. Conducting scientific research in this field is a great help to health policymakers in preventing, treating, and controlling diseases. Recently, in the case of COVID-19 disease, Qom Province in central Iran has been one of the red provinces (17-19). The COVID-19 pandemic has exerted many adverse effects on various aspects of health, economy, and social life in the world, but what is certain is that in addition to human deaths, the disease has also placed a great economic burden on governments and people (20). The total government costs for treating COVID-19 patients in Qom Province hospitals in this period have been calculated to be 8,916,867 $, more than 83% of total costs. In addition, the results of the present study show that nearly 66% of total government costs were consumed as personnel costs for paying salaries. Previous studies have also revealed that the largest portion of the burden of the disease is related to personnel costs. For instance, the personnel expenditure in hospitals in Ghana was evaluated to be 40 - 60% of total costs (21). In the intensive care unit of a hospital in Germany, 42% of total costs belonged to salary payments to the personnel (22). In general, research demonstrates that personnel costs cover almost 60% of total direct costs (23).
Besides, in the majority of studies aiming to estimate the economic burden of diseases in different hospital wards, the costs of medical materials and devices are higher than other major groups of governmental costs (21, 22). Yet, accordingly, the financings of this study regarding the COVID-19 pandemic, to provide better services to patients, personnel from many other hospital wards and health centers were added to the wards of coronavirus patients, leading to an increase in personnel costs in this ward. It also seems necessary to provide more financial support to the personnel of COVID-19 wards to increase their motivation, so high personnel costs in the COVID -19 care wards are expected. Based on the SDCA method, the costs of final service department, including internal medicine, ICU, and pre-hospital emergency medical service wards involved with treating COVID-19 cases accounted for more than half the total costs. The findings of similar studies also indicate that the costs of the final service department are higher than the overhead and intermediate service department costs in hospitals (23, 24). However, in an epidemic situation, the costs of the final ward usually increase as the number of patients admitted to the internal medicine, ICU, and pre-hospital emergency medical wards increases. In the case of the COVID-19 pandemic, the increase in the number of patients referred to hospitals has raised the costs of the final ward. It seems that the observance of health measures, such as social distancing, regular hand washing, wearing masks and gloves, disinfecting fruits and vegetables, disinfecting surfaces, and personal hygiene, has reduced the incidence of the disease and the number of hospitalizations (25). Hence, we can conclude that by reducing the number of referrals to the internal medicine, ICU, and pre-hospital emergency medical wards, the costs incurred by hospitals in the final department are reduced.
It was found in this study that the opportunity costs for COVID-19 patients in the hospitals reached 420 billion Rials (15.68% of total costs). It is equal to the income that has been lost due to the change of income-generating beds to the new coronavirus diseases beds in Qom University of Medical Sciences in the study period. Changing income-generating beds (mainly including the limited surgical, orthopedic, and cardiac wards of hospitals) into COVID-19 patients’ beds has drastically reduced the special incomes of the hospitals. Some previous studies evaluated the opportunity costs of using hospital beds (26, 27). Nevertheless, its impact on the hospital budget is important and should be considered. Moreover, the results of this study revealed that out-of-pocket costs of patients and their families equaled 30,038,013,060 Rials. In addition to opportunity costs, large sums of patients’ income (out-of-pocket) were also spent on COVID-19 disease in the study period. Such costs incurred by patients and their families can adversely affect other aspects of their lives.
The important issue in this study is that the economic burden of the disease has been much higher than the calculated figure, and to calculate it, with the cooperation of the Ministry of Industry, Mine and Trade, as well as the governor's office and other related agencies, damaged jobs and other social losses to be recorded. In this study, only treatment and health costs, opportunity costs related to the lost income of the Qom Province hospitals, and out-of-pocket costs of inpatients were calculated. Besides, the main limitation of the study was that the included cases did not cover all COVID-19 cases in Qom Province; nevertheless, the results seem to partly indicate total costs spent on health care services provided to COVID-19 patients in this area.
5.1. Conclusions
According to the findings, the direct and indirect costs of the treatment of COVID-19 patients can place a heavy economic burden on patients and health systems, including damaged jobs and other social losses, the opportunity costs related to the income loss in Qom Province hospitals, and out-of-pocket costs of inpatients on households and the health care system. Therefore, disease prevention strategies such as observing health protocols are recommended to reduce the economic burden of the disease.