1. Background
COVID-19 was first announced in Wuhan, China, in December 2019, with rapid blowout worldwide (1). Medical education faced a new challenge during the COVID-19 pandemic, which necessitated electronic education with limited workplace encounters in several countries (2). In Iran, like in other countries such as Italy, Ireland, and the United Kingdom, medical students are regarded as medical personnel responsible for caring for patients with COVID-19 (3). Medical students will be the first responders in future pandemics, yet they lack some skills necessary to practice safely and effectively (4).
On the other hand, practicing and teaching in an environment where lethal diseases happen in patients and healthcare personnel impose tremendous psychological pressure on healthcare workers and medical students (5). Stress, anxiety, and depression decrease the quality of medical care (6, 7). On the other hand, the impact of perceived empathy from healthcare workers is so significant that it even affects the mental status of discharged patients (8).
Empathy is a social skill in which a person can understand the inner emotions of their counterparts (9). This capacity is a factor associated with attenuating compassion, fatigue, and burnout among healthcare workers. Hence, this variable is essential to professional quality of life (10-12).
Fear, on logical levels, can be used as an initiative to practice preventive measures and, at excessive levels, can have detrimental effects on the healthcare workers’ personal life and social and professional skills (13, 14). The COVID-19 pandemic has caused widespread; panic, fear, and mental health problems in the community and among healthcare workers (15-19). Therefore, all nations implement public health measures to stopover the spread of COVID-19, including quarantines and social isolation (20-22). Kannampallil et al. indicated that as a result of being exposed to COVID-19 patients, physician trainees experienced higher stress and burnout, raising the psychological and physical strain on medical students (23). Researchers discovered that trainees exposed to COVID-19 patients underwent more pressure and were more susceptible to burnout (23).
This pandemic has sped up a trend toward tension in healthcare professionals, highlighting that burnout is particularly likable when delivering care is not only anxiety-inducing and depressing but also emotionally upsetting. In these circumstances, healthcare professionals lack the mental capacity to feel clinical empathy. During the pandemic, they must deal not only with the prejudice and social stigma associated with working with COVID-19 patients but also with the potential risk of contamination (24, 25). Compared to other physicians, empathic physicians have a high degree of satisfaction and are less prone to weariness and sadness (26). It is highly beneficial to investigate the characteristics of further empathetic medical students and support the development of empathy throughout medical education (27).
2. Objectives
This study aimed to evaluate the empathy with COVID-19 patients and fear of COVID-19 among medical students at Shiraz University of Medical Sciences as important role players in the Iranian healthcare system and to correlate the empathy and fear scores with demographic features to implement appropriate social support for this population.
3. Methods
This cross-sectional study was done at Shiraz University of Medical Sciences in 2020. The study population was the last-year medical students exposed to patients with COVID-19 in all clinical workplaces in Shiraz.
3.1. Participants and Setting
The sample size was determined based on a study performed by Ahorsu et al. (30) and considering α = 0.05 (level of significance), a margin of error of 0.22, the Z1 - α/2 value of 1.96, a mean of 3.48, and a standard deviation of 1.14. Based on a sample attrition of 10%, the number of participants was 107 students. Then, students willing to participate in the study were randomly selected to fill out the questionnaires. All clinical medical students could enter the study, and those who did not want to participate were excluded.
A Persian version of the Jefferson Scale of Physician Empathy (JSPE) was used to assess the participants’ compassion and empathy toward COVID-19 patients. The reliability and validity of the questionnaire have been approved in prior research by Shariat et al. (31). The internal validity of the Persian version of JSPE was 0.78, and its test-retest reliability after 14 days was 0.92 (32). The reliability coefficient (Cronbach’s alpha of 0.83) of the JSPE-HP was excellent. The test-retest reliability measured by intraclass correlation coefficient (ICC) was 0.82 (95% CI: 0.80 - 0.87) (32).
The JSPE questionnaire includes 20 items on a seven‑point Likert scale ranging from “strongly disagree” to “strongly agree.” The range of possible scores goes from 20 to 140. The highest score shows the greatest degree of empathy. In this research, the obtained empathy score resulted from the total score of the JSPE questionnaire. The results of JSPE were used to assess the participants’ empathy toward patients (31, 33).
The participants were also asked to fill out the Fear of COVID-19 Scale (FCV‐19S), previously established by Ahorsu et al., to assess their fear of affliction with COVID-19 (30). Reliability measures such as internal consistency (α = 0.82) and test-retest reliability (ICC = 0.72) were suitable. Wakashima et al. indicated the factor structure of the Japanese FCV-19S with seven items and one factor equivalent to the original FCV-19S (34). The scale showed adequate internal reliability (α = 0.87; ω = 0.92) and concurrent validity (34). This Likert scale consists of seven items, with the score for each item ranging from one to five. The range of possible scores goes from 7 to 35 points. The highest score shows the greatest degree of fear (30, 35).
Content validity index (CVI) and content validity ratio (CVR) were calculated for both questionnaires. The questionnaires were distributed to 15 faculty members. To obtain CVR, the experts were requested to mention their views regarding the necessity and appropriateness of each question on the Likert scale (necessary, useful but not necessary, not necessary). To obtain CVI, the relevancy and clarity of each question were determined. The CVI was above 0.79, and the CVR was at least 0.59 for both questionnaires, which were acceptable (36).
3.2. Data Collection
Data were collected from participants using questionnaires. The students were contacted via email and social media, namely, WhatsApp and Instagram. Last-year medical students in various clinical rotations were asked to collaborate with the researchers. They were asked to fill out an online questionnaire assessing their fear and empathy toward COVID-19 patients during the COVID-19 pandemic.
3.3. Statistical Analysis
A systematic random sampling method was used to choose the participants. The data were entered into IBM SPSS version 24.0. Since the normality of data distribution was not approved, we used nonparametric tests, namely, the Mann-Whitney U test and the Spearman correlation coefficient. All statistical tests were applied at the 0.05 significance level.
3.4. Ethical Considerations
The Ethics Committee of Shiraz University of Medical Sciences assessed and approved the study by the code IR.SUMS.MED.REC.1400.546. Students voluntarily participated in the survey and completed the questionnaires. Also, the anonymity of the participants was granted.
4. Results
This study recruited 107 medical students at Shiraz University of Medical Sciences. The mean age of the participants was 24.37 ± 1.04 years ranging from 24 to 26 years, with median and IQR of 23 and 1, respectively. The students’ mean grade point average (GPA) was 15.4 ± 0.96 out of 20, ranging from 13 to 18, with median and IQR of 15.36 and 1.13, respectively. Other demographic data of the participants are summarized in Table 1.
Table 1.
Demographic Information of the Participants
| Variables | No. (%) |
|---|---|
| Sex | |
| Male | 45 (42.1) |
| Female | 62 (57.9) |
| Place of residence | |
| In dormitories | 47 (43.9) |
| Out of dormitories | 60 (56.1) |
| History of COVID-19 | |
| Yes | 81 (75.7) |
| No | 26 (24.3) |
The results of the fear of COVID-19 are shown in Table 2.
Table 2.
Fear Scores of Medical Students Concerning Exposure to COVID-19
| Items of the Questionnaire | Mean ± SD |
|---|---|
| COVID-19 is what I fear the most. | 3.29 ± 1.07 |
| The thought of COVID-19 makes me uneasy. | 3.44 ± 1.16 |
| The thought of COVID-19 makes my palms sweat. | 3.74 ± 0.98 |
| I worry that COVID-19 will cause me to pass away. | 3.27 ± 1.31 |
| I feel uneasy or worried when I read news and articles regarding COVID-19 on social media. | 3.37 ± 1.10 |
| I’m afraid of acquiring COVID-19, so I can’t sleep. | 4.01 ± 1.05 |
| When I consider contracting COVID-19, my heart may race or palpate. | 3.81 ± 1.04 |
As can be seen, this table indicates the mean scores of fear questions among medical students who were exposed to patients with COVID-19. Each part’s score is out of 5. Generally, the mean fear score was 24.93 ± 6.16 out of 35, in the range of 10 to 35. The scores of JSPE are shown in Table 3.
Table 3.
Empathy Scores Among Medical Students
| Items of the Questionnaire | Mean ± SD |
|---|---|
| Only medical or surgical treatment can heal patients’ ailments; thus, my patients’ emotional connections to me don’t significantly affect how well those procedures go. | 3.68 ± 0.96 |
| It is not beneficial to comprehend patients’ health symptoms to inquire about their personal lives. | 2.66 ± 1.14 |
| I firmly believe that treating medical conditions with emotion is inappropriate. | 3.87 ± 0.91 |
| My patients admire my capacity to empathize with them, which is therapeutic in and of itself. | 4.17 ± 0.64 |
| Paying attention to the unique experiences of my patients has no bearing on how well they respond to treatment. | 3.56 ± 1.02 |
| When taking their history or inquiring about their physical condition, I try not to pay attention to their emotions. | 3.56 ± 1.14 |
| When I recognize my patients’ emotions, they feel better. | 3.94 ± 1.08 |
| In the interaction between a caregiver and a patient, I believe reading body language is just as crucial as verbal communication. | 3.77 ± 1.14 |
| I believe my good sense of humor helps provide better therapeutic results. | 3.68 ± 1.04 |
| My awareness of my patients’ and their families’ emotional states is crucial to our interaction. | 3.91 ± 1.08 |
| In my opinion, a key therapeutic component of any medical or surgical procedure is empathy. | 3.88 ± 1.07 |
| I attempt to think like my patients to provide them with better care. | 3.67 ± 1.09 |
| By observing nonverbal clues and body language, I attempt to decipher what is going on in my patients’ heads. | 3.63 ± 0.99 |
| When giving patient care, I attempt to put myself in their position. | 3.62 ± 1.17 |
| Without the therapeutic skill of empathy, therapy success is constrained. | 3.39 ± 1.11 |
| I find it challenging to see things from my patients’ viewpoints. | 2.97 ± 1.08 |
| It is challenging for me to understand my patients’ opinions because people differ from one another. | 3.05 ± 1.13 |
| My perception of how my patients and their family feel has no bearing on their medical or surgical care. | 3.39 ± 0.96 |
| I don’t let the close relationships between my patients’ families and myself affect how I treat them. | 3.75 ± 0.90 |
| I would not say I like reading non-medical books or works of art. | 3.77 ± 1.14 |
The table shows the mean scores of empathy questions among medical students. Each part’s score is out of 7. Generally, the mean empathy score was 71.94 ± 12.83 out of 140, in the range of 38 to 89. Of 81 participants with a history of COVID-19, 10 participants showed very severe symptoms, 16 participants had severe symptoms, 35 were afflicted with the moderate form of the disease, and 27 participants had mild COVID-19. The Mann-Whitney U test was used to evaluate the association of empathy and fear of COVID-19 with sex, history of COVID-19, and place of residence (Table 4).
Table 4.
Relationship of Demographic Information with Empathy and Fear
| Variables | n | Median | IQR | Mann-Whitney | P-Value |
|---|---|---|---|---|---|
| Empathy | |||||
| Gender | 1108.5 | 0.037 | |||
| Male | 45 | 68 | 14 | ||
| Female | 62 | 72.5 | 14.75 | ||
| Place of residence | 1307 | 0.04 | |||
| In dormitories | 47 | 69 | 15.5 | ||
| Out of dormitories | 60 | 71 | 13 | ||
| History of COVID-19 | 836 | 0.11 | |||
| Yes | 81 | 71 | 13 | ||
| No | 26 | 65 | 20.5 | ||
| Fear | |||||
| Gender | 1364 | 0.84 | |||
| Male | 45 | 28 | 9 | ||
| Female | 62 | 28 | 10 | ||
| Place of residence | 1318.5 | 0.03 | |||
| In dormitories | 47 | 24 | 13 | ||
| Out of dormitories | 60 | 28 | 6.75 | ||
| History of COVID-19 | 902 | 0.27 | |||
| Yes | 81 | 26.5 | 10.5 | ||
| No | 26 | 28 | 8.5 | ||
Consequently, sex and place of residence were significantly associated with empathy with COVID-19 patients in a way that male students and those who resided in dormitories showed more empathy with COVID-19 patients, and there was no significant association between empathy and history of COVID-19. Fear of COVID-19 was significantly associated with place of residence in a way that students residing out of dormitories were afraid of COVID-19 more than the students living in dormitories. There was no significant association between fear and a history of COVID-19.
The Spearman correlation coefficient test was used to assess age correlation with fear of COVID-19 and empathy toward COVID-19 patients. The analysis showed that empathy toward COVID-19 patients and fear of COVID-19 were not correlated with age (Table 5).
Table 5.
Correlation of Age with Fear and Empathy
| Variables | n | Spearman Correlation Coefficient | P-Value |
|---|---|---|---|
| Empathy * age | 107 | 0.026 | 0.78 |
| Fear * age | 107 | 0.023 | 0.81 |
The Spearman correlation coefficient test showed an association between fear and empathy in medical students with a history of COVID-19 (r = -0.249). The more empathy, the less fear, and vice versa, and this association was statistically significant (P-value = 0.02). In comparison, students without a history of COVID-19 did not show a statistically significant association between fear and empathy (P-value = 0.64). In general, the Spearman correlation coefficient test showed no statistically significant association between fear and empathy (P-value = 0.83).
5. Discussion
This cross-sectional study highlighted the pandemic’s impact on medical students’ fear and empathy toward COVID-19 patients. The mean empathy score of our participants was higher for male students and those who resided in dormitories. Participants living out of the dormitories feared COVID-19 to a greater extent. No statistically significant correlation was found between the age of the participants and these two parameters. Also, students with a history of COVID-19 were more empathetic to COVID-19 patients. They also felt less fear of coping with COVID-19. However, in students with no history of COVID-19, no correlation was found between fear and patient empathy.
In the pre-COVID era, Rezayat et al. performed a study on medical students of Mashhad, Northeastern Iran, using the JSPE; the mean score of empathy in medical students in the mentioned study was significantly higher than in our study (37). This difference might be because medical students might think that COVID-19 patients endangered the students’ health and well-being and were concerned about infecting themselves and other patients and relatives.
Another study conducted by Khademolhosseini et al. performed on medical students of Shiraz University of Medical Sciences, where we also conducted our study, found that the mean empathy score of the participants was lower than in our research, and they discovered that the empathy score was inversely correlated with age and level of education (38). This apparent difference might be because our participants had a narrow age range and were from the same educational level.
In a study performed by Nasiri et al. on last-year medical students of Shiraz University of Medical Sciences, their participants’ mean empathy score was significantly higher than the empathy score in our study (33). This difference might root in two distinctions. First, in our research, the medical students were assessed regarding their empathy toward COVID-19 patients, not patients in general. As mentioned above, some students might blame COVID-19 patients for afflicting the disease by not following public health protocols. Secondly, they assessed last-year medical students who had had some medical experience before the pandemic. In contrast, our participants did not have such an experience and had no chance of developing empathy for their non-COVID-19 patients.
In previous studies on Iranian medical students, no difference existed between male and female students in empathy, or female students showed higher empathy than male students (33, 37-39). However, in our study, male patients showed higher empathy toward COVID-19 patients. This difference might be consequent to the fact that female medical students were psychologically affected by the COVID-19 pandemic more profoundly than their male counterparts due to their difference in coping mechanisms (40). In the study of Canas-Lerma et al., empathy ranks in professionals (117) and students (170) from numerous healthcare fields in Ecuador throughout the COVID-19 pandemic were analyzed, and gender had a significant impact on empathy (41).
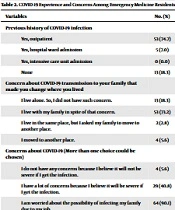
In our study, medical students who lived in dormitories showed more empathy for COVID-19 patients and less fear of COVID-19. The reason for the difference between the two groups could be that medical students residing out of dormitories have more contact with their family members, and they might have concerns about transmitting this disease to their loved ones, who might have a high risk of infection mortality. This relation was confirmed by a study by Welsh et al., who found that one of the most significant concerns of emergency physicians taking care of COVID-19 patients during the pandemic was transmitting the disease to their family members (42).
In a study by Terzic-Supic et al., performed on Serbian medical students, higher fear of COVID-19 was correlated with higher knowledge of COVID-19 and better preventive practices for this disease (43). They found that since medical students were knowledgeable regarding this disease, they could play roles in health promotion teams (43). In our population, however, medical students act as active healthcare workers responsible for patient care; therefore, higher levels of fear could have drastic outcomes in patient care.
Natalia and Syakurah found that a higher level of fear was related to stress, anxiety, and depression (44). Therefore, finding risk factors for higher fear of COVID-19 is of utmost importance in enhancing the mental health of medical students. In our study, the place of residence was related to fear of COVID-19. Consequently, providing safe accommodation for medical students and other healthcare workers could enhance mental health status among medical students. They also found that having family members with comorbidities is a factor associated with a higher level of fear in medical students, confirming our findings.
Campos et al. found that the fear of COVID-19 was higher among female medical students than male medical students; however, our study did not confirm such findings (45). These differences might have been rooted in the cultural differences between Portugal and Iran (45). Yang et al. found that a higher level of fear among healthcare workers, such as medical students in China, was associated with higher levels of career path regret (46). Such association must be considered when approaching medical students elsewhere in the world. For instance, in Iran, since medical students are in direct contact with patients during clinical rounds and shifts, career path regret might end in students’ unwillingness to continue their residency studies. As active personnel in the healthcare system of Iran, medical students might also lose their trust in the national healthcare system. This loss of trust, combined with low faith in the healthcare system by people, could have dire consequences, such as the total collapse of healthcare in Iran (47).
Richins et al. indicated that exposing participants to a dreadful situation was sufficient to reduce empathy (48). These findings are in line with our study; since current infection among students who had experienced COVID-19 previously caused post-infection immunity (49, 50), they had less fear of encountering COVID-19 patients and had more empathy. It is important to mention that student support arrangements for undergraduate medical students throughout the COVID-19 pandemic are needed for more preparation of medical students for future pandemics (49).
As with all studies, this study had limitations. First, because the survey was done online, we could not identify any psychological issues, such as anxiety or depression, in the participants, which could allow us to assess the sensitivity and specificity of the questionnaire’s scale. Second, as the study was done at a single center, it has limited generalizability.
5.1. Conclusions
This study highlights the impact of the pandemic on the interaction between medical students as healthcare professionals and patients by affecting medical students’ fear and empathy. The study indicates ways to improve readiness for future pandemics. Our study showed that living far away from families in dormitories may influence students’ fear and empathy; moreover, empathy, unlike fear, is affected by gender. A reverse correlation exists between fear and empathy in students with a history of COVID-19, indicating that the more they have empathy, the less they experience fear.