




1. Background
The concept of physical literacy was first introduced by Margaret Whitehead (1993). This concept includes motivation, confidence, physical competency, knowledge, and understanding the value of and taking responsibility for physical activities during life (1). Physical literacy is a comprehensive concept that applies to anyone at any age or physical ability and is related to the whole life of a person (2). Physical literacy is defined as a person’s capacity to live a healthy life and allows a person to conquer a wide range of physical activities with motivation and self-confidence and respond appropriately to existing environmental conditions based on his/her perception (3).
According to the results of studies, the average physical literacy score of adolescents is 63% for boys and 62% for girls, showing a moderate score for physical literacy and indicating that girls usually have a lower average physical literacy score than boys (4, 5). Adolescents with lower physical literacy are less likely to be involved in physical activities, increasing the risk of diseases associated with a sedentary lifestyle, such as obesity and diabetes (6, 7). Many health-related behaviors that usually begin before or during adolescence, such as obesity and lack of physical activity, seem to contribute to the spread of non-contagious diseases in adulthood, for example, in people over 60 years of age. Hypertension, cholesterol and glucose disorders (29%), smoking (10%), lack of physical activity (7%), and overweight or obesity (7%) are responsible for years of lost life due to predisposing people to serious diseases and disabilities. However, adequate and regular physical activities reduce the risk of developing these diseases during adulthood (8, 9). School-age is one of the most important periods of life to ensure a healthy life in adulthood (10). Adherence to proper physical activities during the growth years helps secure health during forthcoming years, so there is a need to encourage healthy behaviors among adolescents (11, 12). The content analysis method can be used to clarify the concept of physical literacy for adolescents. One of the best methods to develop new tools or refine existing tools is quality content analysis. Using this method, all the main dimensions and structures of a tool can be identified (13). Since there is no local definition and appropriate tool in this field in Iran, in this study, we employed the content analysis method to develop and validate a tool for assessing physical literacy among Iranian adolescents.
Most studies in the world on physical literacy have been conducted on 8 - 12-year-old children. Most of these studies have used the Canadian Assessment of Physical Literacy (CAPL) for 8 - 12-year-old children, a standard questionnaire that addresses four dimensions, including knowledge and understanding, motivation and self-confidence, physical fitness, and daily behavior (5). In another study, only the dimension of physical literacy knowledge was investigated using the Physical Literacy Knowledge Questionnaire (PLKQ) (14), leaving other dimensions of physical literacy uninvestigated. In another study, the perceived physical literacy of 12 - 18-year-old adolescents was assessed using the Perceived Physical Literacy Instrument (PPLI) (15). Yet, no special tool has been developed to measure the physical literacy of 16 - 18-year-old Iranian adolescents, and only a physical literacy knowledge questionnaire for the age group of 8 to 12 years has been psychometrically validated in Iran (16).
2. Objectives
After defining the concept of physical literacy of adolescents aged 16 to 18 years according to the experiences of Iranian adolescents and specialists, we designed a questionnaire to measure physical literacy based on Iran’s social culture and attitudes and then assessed the psychometric features of the instrument.
3. Methods
3.1. Study Design
The present study was a methodological two-step experiment. In the first step, a qualitative study was conducted to divulge the concept of physical literacy. In the second stage, the content, face, and construct validity and reliability (internal consistency and reliability) of the tool were determined to validate the psychometrics of the questionnaire developed in the qualitative analysis section.
3.2. Participants
The research environment included 2 high schools for girls and 2 high schools for boys from the educational districts 1 and 4 of Tehran. The research environment for specialists (in the qualitative section of the study) included Shahid Beheshti University of Medical Sciences, the Health Department of Shahid Beheshti University of Medical Sciences, Iran’s Ministry of Education, and the Physical Education Research Institute of Iran. All interviews were conducted by the main researcher in schools’ counseling rooms and the specialists’ workplaces at pre-arranged times. In the qualitative part, convenient sampling was employed to recruit interviewees, and the enrollment of the subjects continued until reaching data saturation. For construct validity, out of 19 educational districts, 4 districts (1, 2, 4, and 6) were selected as clusters. After referring to the education department of each district, 2 schools for girls and 2 schools for boys were randomly selected from the list of high schools. In order to determine the number of samples required for each item, 15 people, including adolescents, were randomly selected. Inclusion criteria for adolescents were (1) employment while studying; and (2) providing informed consent to participate in the research. Entry criteria for specialists included having work or research experience in the field.
3.3. Data Collection
In the first stage, semi-structured face-to-face interviews were conducted with 11 students and 15 specialists. The duration of each interview was between 15 and 80 minutes, with an average duration of 33 minutes. Data were collected from May to August 2020. All interviews were digitally recorded with the permission of the participants. At the end of each interview, information was immediately entered into MAXQDA 10 software. Data analysis was conducted simultaneously with data collection. After reaching information saturation, data collection continued for two more interviews.
In the second stage, quantitative and qualitative methods were used to confirm the content validity of the tool based on the judgments of 12 specialists, including 7 health education and health promotion specialists and 5 physical education specialists) who had knowledge and experience in the field of tool design. The opinions of these experts were applied to the questionnaire after holding a group discussion session with the participation of the members of the research team. In order to confirm face validity qualitatively, the questionnaire was given to 10 male and female students, and they were asked to comment on the difficulty or simplicity of the questionnaire’s items, their meaning, and any ambiguity in wording. In a cross-sectional study, the construct validity was tested on 510 adolescents. Regarding the students, the objectives of the study were initially explained to them, and after obtaining their informed consent, the questionnaires were completed by self-reporting.
3.4. Data Analysis
The conventional content analysis method described by Granheim and Landman was used for qualitative data analysis (17). In order to confirm quantitative content validity, the content validity ratio (CVR) and content validity index (CVI) were used. For CVR, specialists were asked to review each phrase of the tool based on a 3-point scale (necessary, useful but not necessary, and not necessary). According to the Lawshe table (18), to determine the minimum value of CVR, phrases whose CVR numerical values were at least (0.56) were retained in the questionnaire. For CVI, according to Waltz and Bausell (19), the relevance, transparency, and simplicity of each of the questionnaire’s phrases were determined, where the specialists were requested to provide the necessary feedback on the validity of the qualitative content of the questionnaire regarding grammar, appropriate wording, necessity, and proper positioning. The face validity of the questionnaire was confirmed by both quantitative and qualitative methods. In order to determine the importance of each question, the item impact method was used. At this point, 16 - 18-year-old boy and girl students were asked to score each phrase on a 5-point Likert scale from “absolutely important" to “not important at all". If the impact score of the question was equal to or greater than 1.5, that question was considered appropriate and retained for subsequent analysis (20).
Exploratory factor analysis with varimax rotation was used to confirm the construct validity of the tool. In order to reach the most desired number of factors, the following items were considered: (1) contribution to the total variance; (2) factor eigenvalue; and (3) scree plot (21). The appropriateness of the data for exploratory factor analysis was measured by the two tests of sampling quality of Kaiser-Mayer-Olkin (KMO) and Bartlett sphericity. The result of the KMO test varies between zero and one, and the higher the value, the more appropriate the factor analysis will be. Values above 0.80 are considered appropriate (22). The Bartlett sphericity test was then used to ensure that the correlation matrix underlying factor analysis was not zero in the population. In order to determine the number of factors, the factor eigenvalue was higher than one, and it was higher than 0.4 for the factor load.
In order to determine the instrument’s internal consistency, the correlation between the questions in each dimension and the questionnaire was calculated using Cronbach’s alpha. Cronbach’s alpha above 0.7 usually indicates the acceptable reliability of a tool. In order to confirm the reliability of the tool developed here, the test-retest method was used by the participation of 30 adolescent boys and girls (n = 30 is usually considered for measuring reliability) over an interval of two weeks. Then, the scores obtained from these two steps were compared using the intra-class correlation coefficient (23). SPSS version 24 was used for statistical analysis.
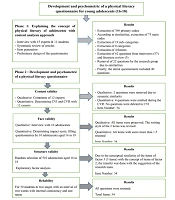
A summary of the process of the development and psychometric analysis of the physical literacy questionnaire has been presented in Figure 1.

Development and psychometric analysis of the physical literacy questionnaire
4. Results
The results were based on 26 interviews, and four themes were obtained for measuring the physical literacy of 16 - 18-year-old adolescents following content analysis (Figure 2). The content analysis of the interviews and reviewing of existing literature on physical literacy led to the development of an initial tool with 62 phrases, reducing to 40 phrases after the initial review by the research team. These phrases were designed in different dimensions, including information acquisition, comprehension, and assessment skills, as well as self-care skills, and each phrase had a range from never to always on a 5-point Likert scale. In order to confirm the qualitative content validity of the 40-item tool, after applying the opinions of 12 specialists, due to semantic similarity, 2 questions related to information acquisition skills and 2 questions related to information assessment skills were merged (i.e., 2 questions were excluded from the questionnaire). Also, 4 questions with CVR less than 0.56 were excluded from the questionnaire, and the total number of questions in the questionnaire was reduced to 34 questions. The CVI of the tool was 0.96. For face validity, according to the opinions of 10 students, the writing style of 2 questions was corrected, and since the impact score of all questions was higher than 1.5, no question was excluded, and a questionnaire with 34 questions was used for construct validity assessment.

Themes and categories regarding the physical literacy of adolescents aged 16 - 18 years
Construct validity assessment on 510 16 - 18-year-old boy and girl students (50.2% girls) revealed that 58.6% of adolescents were members of sports clubs, and 42.4% of them selected the Internet as the first source of information on physical activities (Table 1).
| Variables | No. (%) |
|---|---|
| Gender | |
| Male | 254 (49.8) |
| Female | 256 (50.2) |
| Age (y) | |
| 16 | 134 (26.3) |
| 17 | 207 (40.6) |
| 18 | 169 (33.1) |
| Academic grade | |
| 10 | 157 (30.8) |
| 11 | 155 (30.4) |
| 12 | 198 (38.8) |
| Field of study | |
| Vocational training | 103 (20.2) |
| Technical training | 96 (18.8) |
| Humanities | 108 (21.2) |
| Experimental sciences | 111 (21.8) |
| Mathematics & physics | 92 (18) |
| Sports club membership | |
| No | 211 (41.4) |
| Yes | 299 (58.6) |
| The initial source of information | |
| Physical education teacher | 60 (11.8) |
| Sports club’s coach | 116 (22.7) |
| Parents | 80 (15.7) |
| Friends | 38 (7.5) |
| Internet | 216 (42.4) |
In order to confirm the construct validity after ensuring the adequacy of sampling based on the KMO and Bartlett sphericity tests (P = 0.001, χ2 = 10421.8, KMO = 0.946), the initial factor analysis revealed that the questionnaire’s questions with 5 factors and eigenvalues above 1 explained a total of 61.60% of the variance (Table 2).
| Component | Initial Eigenvalues | Rotation Sums of Squared Loadings | |
|---|---|---|---|
| Total | % of Variance | Cumulative% | |
| 1 | 12.51 | 16.176 | 16.176 |
| 2 | 4.06 | 15.973 | 32.150 |
| 3 | 2.04 | 13.121 | 45.271 |
| 4 | 1.28 | 10.003 | 55.274 |
| 5 | 1.04 | 6.332 | 61.606 |
For investigating the results of factor analysis, items with a load of 0.4 or higher were considered appropriate. Factor analysis was performed several times based on different factors. As a result, the researcher found that the 5-factor solution was the best result of a clear pattern of factor loads. In this study, the first 5 factors explained the factor structure of the Physical Literacy Questionnaire for 16 - 18-year-old adolescents. Of course, according to the opinion of the research team and due to conceptual similarity, Factor 5’s items (3 items) were transferred to Factor 2, and the questionnaire was finally considered to include 4 factors. In addition, no question was excluded from the questionnaire after exploratory factor analysis, and all 34 items of 16 - 18-year-old adolescents’ physical literacy questionnaire were retained after factor analysis (Table 3).
| Items | Component | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| I can acquire information about the duration of the required physical activity from various sources (the Internet, physical education specialists, friends, and family). | 0.819 | 0.254 | 0.078 | 0.089 | 0.086 |
| I can acquire information about physical activity from various sources (the Internet, physical education specialists, friends, and family). | 0.787 | 0.216 | 0.073 | 0.008 | 0.054 |
| I can acquire information about the benefits of physical activity from various sources (the Internet, physical education specialists, friends, and family). | 0.778 | 0.279 | 0.067 | 0.126 | 0.138 |
| I can acquire information about my favorite physical activities from various sources (the Internet, physical education specialists, friends, and family). | 0.768 | 0.264 | 0.083 | 0.083 | 0.099 |
| I can acquire information about diseases caused by insufficient physical activity from various sources (the Internet, physical education specialists, friends, and family). | 0.675 | 0.304 | 0.055 | 0.240 | 0.101 |
| I can acquire information about the functioning of different organs in my body from different sources (the internet, physical education specialists, friends, and family). | 0.668 | 0.267 | 0.029 | 0.212 | 0.158 |
| I can acquire information about sports equipment from various sources (the Internet, physical education specialists, friends, and family). | 0.641 | 0.372 | 0.074 | 0.136 | 0.152 |
| I can acquire information about how to prevent injuries during physical activity from various sources (the internet, physical education specialists, friends, and family). | 0.614 | 0.364 | 0.084 | 0.196 | 0.120 |
| I can comprehend the information about how to do physical activity movements acquired from various sources (the internet, physical education specialists, friends, and family). | 0.321 | 0.740 | 0.098 | 0.126 | 0.098 |
| I can comprehend the meaning of my favorite physical activity based on the information acquired from various sources (the internet, physical education specialists, friends, and family). | 0.360 | 0.731 | 0.063 | 0.083 | 0.185 |
| I understand information about the benefits of physical activity acquired from various sources (the internet, physical education specialists, friends, and family). | 0.297 | 0.719 | 0.105 | 0.206 | 0.244 |
| I can comprehend the information and advice on healthy eating habits acquired from various sources (the internet, physical education specialists, friends, and family). | 0.286 | 0.706 | 0.083 | 0.188 | 0.137 |
| I can comprehend most of what I hear about physical activity from a variety of sources (the internet, physical education specialists, friends, and family). | 0.332 | 0.699 | 0.041 | 0.255 | 0.207 |
| I can comprehend the advice for preventing injuries during physical activity received from various sources (the internet, physical education specialists, friends, and family). | 0.334 | 0.687 | 0.116 | 0.215 | 0.168 |
| I can comprehend information about physical activities suitable for adolescents acquired from various sources (the internet, physical education specialists, friends, and family). | 0.386 | 0.677 | 0.096 | 0.121 | 0.187 |
| I comprehend the meaning of physical activity information acquired from various sources (the internet, physical education specialists, friends, and family). | 0.417 | 0.652 | 0.116 | 0.255 | -0.036 |
| To take care of my health, I usually do physical activity during school exams. | 0.114 | -0.053 | 0.820 | 0.011 | 0.089 |
| I do physical activity regularly on a daily basis to avoid gaining weight. | 0.046 | 0.112 | 0.797 | 0.145 | -0.033 |
| To take care of my health, even in apartment houses, I do proper physical activities at home. | 0.046 | 0.150 | 0.783 | 0.017 | 0.100 |
| To take care of my health, I usually do physical activity in any undesired situation. | 0.041 | 0.018 | 0.767 | 0.154 | -0.023 |
| To take care of my health, even in the case of air pollution, I do proper physical activities at home. | 0.107 | 0.083 | 0.762 | 0.072 | 0.039 |
| To take care of my health, I do 30 - 60 minutes of physical activity daily, including walking, cycling, etc. | 0.019 | 0.162 | 0.699 | 0.130 | 0.077 |
| I follow the physical education teacher’s advice on the appropriate diet for physical activity. | 0.027 | 0.052 | 0.578 | 0.428 | 0.141 |
| I usually use safe equipment when doing physical activities. | 0.150 | 0.056 | 0.511 | 0.293 | 0.285 |
| I use my cell phone pedometer to find out how many calories my body has burned based on the physical activity I did during the day. | 0.042 | -0.023 | 0.462 | 0.448 | -0.232 |
| When I come across new information about physical activity, I can judge its correctness. | 0.110 | 0.330 | 0.147 | 0.714 | 0.039 |
| I compare the information about physical activity that my physical education teacher teaches with the educational videos I watch. | 0.166 | 0.088 | 0.220 | 0.652 | 0.072 |
| Regarding physical activity information from various sources (the internet, physical education specialists, friends, and family), I can assess which source is of higher quality. | 0.198 | 0.340 | 0.080 | 0.563 | 0.159 |
| I can assess the accuracy of the information that friends and family give me about physical activity. | 0.193 | 0.317 | 0.131 | 0.519 | 0.314 |
| When selecting physical activity information, I check if it is appropriate for my age and gender. | 0.046 | 0.206 | 0.051 | 0.505 | 0.419 |
| I can assess the accuracy of the information I receive about physical activity from various sources (the internet, physical education specialists, friends, and family). | 0.239 | 0.407 | 0.089 | 0.497 | 0.249 |
| I comprehend the physical activity information that my family gives me. | 0.189 | 0.269 | 0.014 | 0.199 | 0.725 |
| I comprehend physical activity-related information that a physical education teacher or a sports club coach gives me. | 0.180 | 0.296 | 0.189 | 0.116 | 0.677 |
| I comprehend the physical activity information my friends give me. | 0.279 | 0.134 | -0.013 | 0.363 | 0.527 |
The Scree plot is a graphical representation of the relative sizes of eigenvalues. The horizontal axis represents the number of factors, and the vertical axis represents the eigenvalue (Figure 3). This plot is used to provide a basis for determining the logical point of failure between eigenvalues and helps the researcher determine the number of factors in the data.

Scree plot of differentiated factors through exploratory factor analysis of adolescents’ physical literacy questionnaire
In order to confirm the reliability of the questionnaire, Cronbach’s alpha coefficient of the tool was calculated as 0.93, and the reliability coefficient of the tool was obtained as 0.97 (Table 4).
| Dimension | Number of Items | Cronbach’s Alpha (N = 510) | ICC (N = 30 ) |
|---|---|---|---|
| Information acquisition | 8 | 0.919 | 0.962 |
| Information comprehension | 11 | 0.920 | 0.970 |
| Information assessment | 6 | 0.818 | 0.906 |
| Self-care | 9 | 0.874 | 0.960 |
| Whole questionnaire | 34 | 0.939 | 0.975 |
Finally, adolescents’ physical literacy questionnaire was approved with 34 questions in 4 dimensions, including information acquisition skills (8 questions), information comprehension skills (11 questions), information assessment skills (6 questions), and self-care skills (9 questions).
5. Discussion
The initial questionnaire was designed based on the data obtained from a qualitative study using the opinions of 16 - 18-year-old students, health education and health promotion specialists, and physical education experts, as well as the review of the existing literature on physical literacy. After assessing psychometric features, a 34-item adolescents’ physical literacy questionnaire, including 4 dimensions (information acquisition skills, information comprehension skills, information assessment skills, and self-care skills), was developed. The tool was completed by self-reporting. Most of the participants completed the questionnaire in about 15 minutes, indicating that this tool could be easily used for screening purposes.
So far, physical literacy studies in Iran have mostly used CAPL (6, 16)to investigate physical literacy among 8 - 12-year-olds, and no study has yet addressed physical literacy among 16 - 18-year-old adolescents. In this study, the tool designed for this purpose delivered a comprehensive, specific, valid, and reliable indigenous instrument to measure physical literacy among 16 - 18-year-old Iranian adolescents. The results showed that the content validity index was 0.97 for simplicity, 0.95 for transparency, 0.96 for relevance, and 0.89 for the total content validity ratio. In the present study, the expressed variance index was equal to 62%, which was a desirable and acceptable index. Cronbach’s alpha coefficient for the whole questionnaire was 0.93, indicating the high reliability of the questionnaire. Since no study was found in the field of designing and psychometric assessment of physical literacy measurement tools among 16 - 18-year-old adolescents, we encountered some limitations in comparing this tool with other questionnaires in this area.
The factor structure analysis of the tools designed to measure physical literacy shows different patterns. For example, CAPL used by Longmuir et al. (24) to assess the physical literacy of 8 - 12-year-old children was a four-factor tool investigating the knowledge and understanding, motivation and self-confidence, physical fitness, and daily physical activity behaviors of children. The PLKQ tool used by Longmuir et al. (14) investigated only the dimension of physical literacy among 8-12-year-old children with a reliability of 53%. Another tool, CAMSA, was utilized by Longmuir et al. (25) to assess the dimension of physical fitness among 8 - 12-year-old children, rendering a good reliability of 82%. Caldwell et al. employed PLAY (26) to investigate the physical literacy and motor skills of 8 - 13-year-old children, which showed Cronbach’s alpha of 94%, indicating excellent reliability. Also, PPLI was used by Ma et al. (27) to measure students’ perceived physical literacy with Cronbach’s alpha of 83%, reflecting that the questionnaire had good reliability. Compared to the above-mentioned studies, the tool developed in the present study was more stable and reliable due to containing 4 factors and 34 items and delivering Cronbach’s alpha of 93%. One of the limitations of this tool was that it was a self-reporting scale, making it difficult to compare the differences observed between different individuals or subgroups.
5.1. Conclusions
Based on the themes that emerged in the qualitative study, the physical literacy of adolescents can be defined as a set of information acquisition, comprehension, and assessment skills, as well as self-care skills, allowing them to make the right decisions for maintaining and improving physical activities. The results of this study demonstrated that self-care activities, along with information acquisition, comprehension, and assessment skills, were the original themes of physical literacy among adolescents. The purpose of this study was to design a tool to measure physical literacy among adolescents aged 16 to 18 years. Despite the importance of physical literacy in health education and health promotion, few studies have addressed adolescents’ physical literacy determinants. By explaining the concept of physical literacy and clarifying its dimensions (i.e., information acquisition, comprehension, assessment skills, and self-care skills), more effective interventions can be designed to boost these aspects. Also, the tool designed here was adjusted based on the social and cultural characteristics of Iranian society and can be helpful in determining the status of physical literacy among Iranian adolescents, as well as in designing and implementing interventions related to physical literacy. An enhancement in physical literacy leads to the continuity of adherence to physical activity among adolescents throughout their lifetime, allowing them to maintain their health.
