1. Introduction
Anemia is one of the public health challenges in developing countries. Half of all the cases of anemia can be attributed to iron deficiency (1).World Health Organization has reported that iron deficiency is the most prevalent nutritional problem globally, affecting more than 700 million people (2). The severity of the problem is more among women of reproductive age, especially among pregnant women. It is estimated that half of the pregnant women suffer from iron deficiency anemia. During pregnancy, iron absorption increases, however the increased absorption is not enough to compensate for the increasing demand for iron (3). Favorable pregnancy outcomes occur 30-45% less often in anemic mothers, and their infants have less than one-half of normal iron reserves (2). Anemia, depends on its severity, can have multiple adverse effects on pregnancy outcome for the mother and the fetus including increased risk of hemorrhage, sepsis, maternal mortality, perinatal mortality, and low birthweight (2, 4), 10-15% of maternal mortality is attributed to anemia (5).
Helicobacter pylori (H. pylori) is one of the most common bacterial infection worldwide, almost half of people in developed countries and 80% of people in developing countries suffer from this infection (6). Since identification of the effects of H. pylori on the digestive system, many researchers paid attention to extra-gastric effects of this infection. One of these effects is iron deficiency anemia. Different biological possibility for this association has been reported, including competition for iron between gastric cells and H. pylori, and bleeding through peptic ulcers and other gastric lesions associated with H. pylori.(7, 8). Also it has been suggested that the H pylori-infected antrum may act as a sequestering focus for serum iron, due to the outer membrane receptors of the bacterium (9). A high percentage of H. pylori-positive with iron deficiency anemia demonstrated atrophic changes in the gastric body. H. pylori infection has even been a cause of failure with oral iron treatment. Most dietary iron is in the non-hemic ferric form, and a low gastric pH is needed to reduce it to the ferrous form for absorption. Patients with H pylori gastritis showed an increase in gastric pH
(a median of > 3), that is known to be critical in the process of iron absorption (10).
In spite of common diagnostic tool of Helicobacter pylori through directly in vivo using magnification endoscopy, recently many attempts were made to use less invasive methods (11). Among different proposed methods, we can refer to Rapid Urease Test, a urease test based on an immunological detection of urease, which was proposed for the first time in Japan (12). Another technique is Urea Breath Test, which use 13C-urea breath test (13C-UBT), this technique is considered as a very accurate test, as well as robust, because the specimens can be transported without special conditions, and the result is independent of human interpretation (13). Stool Antigen Testis a valuable non invasive diagnose techniques when UBT is not available. Antibody Detection which is the detection of multiple antibodies in serum by protein array is another non-invasive technique. This array is comprised of three recombinant H. pylori antigens namely UreB, VacA and CagA. These three recombinant H. pylori antigens are immobilized on nitrocellulose membranes. Bound IgG are detected using staphylococcus protein A, which is labeled with colloidal gold (14). Molecular methods, are another widely used techniques for the diagnosis of H. pylori infection (11).
The present study aimed to investigate the association between iron deficiency anemia and H. pylori infections among pregnant women referring to antenatal care center of Shahid Akbarabadi hospital, , .
2. Materials and Methods
This study was a cross-sectional study, conducted among pregnant women referring to antenatal care center in Shahid Akbarabadi Hospital during the year 2010.
2.1. Participants
Out of all pregnant women referring to the antenatal care center, 180 women considering the inclusion and exclusion criteria were identified as eligible by an interviewer (CONVENIENCE & NONRANDOM SEQUENTIAL SAMPLING). However 12 were lost due to not having enough blood samples for ferritin test, or refusing to give the blood sample, even after giving consent for participation in the study, therefore 168 pregnant women participated in the study. The inclusion criteria was the gestational age less than 14 weeks, singleton pregnancy, and giving written consent to participate in the study. The exclusion criteria was underlying disease or severe organ failure, history of drug abuse, antibiotic medication in the prior 4 weeks, history of hemorrhage during pregnancy, long-term use of Aspirin or other anti-inflammatory steroid, history of peptic ulcer or active peptic bleeding, history of malignancy, history of gastric surgery, history diagnosis and treatment of H. Pylori, those with vegetarian diet and any diagnosed infections.
2.2. Data collection method
Demographic data (age, education and number of parity) and clinical data (history of severe pregnancy related vomiting and nausea) was collected by a gynecologist assistant in the center, then 5 ml blood (2 ml for anemia test and 3 ml for helicobacter antibody) was collected from women. If the hemoglobin level was below 11 g/dl, the ferritin level was measured (the level less than 15 mg/dl was considered as iron deficiency anemia). The hemoglobin level was measured with a CBC counter made by sysmex Company in Japan. The H. pylori IgG was detected by Monobind kit made in USA and the Stat fax USA 2010 Eliza reader machine. The serology test of H. pylori IgG was measured by ELIZA test. The IgG antibody titration was determined using the cutoff point of the kit, which was > 20 positive.
2.3. Data analysis
The data were analyzed using SPSS version 17.0. The descriptive statistics along with parametric tests of chi square for qualitative data and t test for quantitative data and non-parametric tests (when the distribution was not normal) was used to assess the relationship between dependent and independent variables. Odd ratio, Pearson correlation test and logistic regression were used to measure the level of association.
2.4. Ethical consideration
The purpose and procedure of the study were explained to the participants. They were ensured that the data are considered confidential and their identity will not be revealed and the data will not be used except for the research purpose. All participants gave written consent to participate in the study. The laboratory tests cost was paid by the researchers and a non-invasive technique was used for data collection.
3. Results
Table 1 shows the socio-demographic data of the participants, the mean age of participants was 27.5 ± 5.7 years (range 15-47 years). 156 participants (93.0%) had educational level of diploma or less than diploma and only 12 (7.1%) had academic education. The pregnancy was first parity for 71 of participants (42.3%) and second parity for 58 (34.5%) participants.
Twenty three of participants (13.7%) reported severe pregnancy related nausea and vomiting (hyperemesis gravidarum) in their first trimester. The mean hemoglobin level of participants was 12.03 ± 1.4 g/dl and the median hemoglobin level was 12.2 g/dl. Fifty two of the participants (31.0%) had a hemoglobin level less than 11 g/dl. Fifty one of the participants (30.4%) had a ferritin level less than 15 mg/dl. There was no association between age, educational level, history of nausea and vomiting of participants and the hemoglobin level.
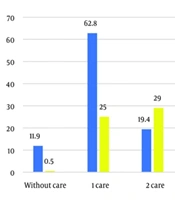
Based on serology IgG test for diagnosis of H. Pylori, 91 participants (54.2%) were positive. There was no significant relation between age and educational level of participants and being serologically positive for H. Pylori, but there was a significant difference in reported history of pregnancy related nausea and vomiting and being serologically positive for H. Pylori (P = 0.003). 20.9% of those being serologically positive for H. Pylori reported suffering from pregnancy related nausea and vomiting while this proportion was 4.8% for those without H. Pylori infection. The risk of having pregnancy related nausea and vomiting among serologically H. Pylori positive was 4.8 times more than those not (95% CI: 1.56-14.8).
two two shows there was a significant and adverse correlation between being serologically H. Pylori positive and hemoglobin level (P = 0.005, r = -0.218).There was a significant and adverse correlation between being serologically H. Pylori positive and ferritin level (P = 0.001, r = -0.263). The t test results, also showed that mean hemoglobin and ferritin level was significantly lower in serologically H. Pylori positive mothers (P = 0.013 and P = 0.001, respectively). The odd ratio of iron deficiency anemia among serologically H. Pylori positive mothers was 3.18 (95% CI: 1.52-6.6).
Table 1.
Demographic Characteristics and Clinical Information of Participants
| Demographic variable | |
|---|---|
| Age (year) | Mean (SD) 27.6 (5.7) |
| Education | Number (%) |
| Illiterate or primary | 25 (14.8) |
| Middle school | 46 (27.4) |
| Diploma | 85 (50.6) |
| Higher education | 12 (7.1) |
| Number of parity | Number (%) |
| First parity | 71 (42.3) |
| Second parity | 58 (34.5) |
| Third parity | 24 (14.3) |
| Forth parity or more | 15 (9.0) |
| Clinical variable | Mean (SD) |
| Hemoglobin level | 12.03 (1.4) |
| Ferritin level | 31.2 (22.9) |
| H. pylori infection | Number (%) |
| Yes | 91 (54.2) |
| No | 77 (45.8) |
Table 2.
Association between H. Pylori Infection and Hemoglobin Level, Ferritin Level and Pregnancy Related Sever Vomiting and Nausea
| H. pylori infection | Yes | No | P value |
|---|---|---|---|
| Hemoglobin level (Mean + SD) | 11.7 ± 1.4 | 12.3 ± 1.2 | 0.013a |
| Ferritin Level (Mean + SD) | 25.6 ± 20.7 | 37.6 ± 23.8 | 0.001 a |
| Sever vomiting and nausea (no, (%)) | 19 (20.9) | 4 (5.2) | 0.003b |
a student t test
b Chi square test
4. Discussion
Recent studies suggested an association between H. Pylori infection and iron deficiency anemia (5, 7-9, 11, 15-17). This study was conducted to test the association between iron deficiency anemia and H. pylori infection among pregnant women referring to antenatal care center of Shahid Akbarabadi hospital, , . The results of this study showed that nearly one third of participants had anemia and iron deficiency anemia. In a study by Weyermann et al.(17) on role the Helicobacter pylori infection in iron, deficiency during pregnancy in Germany, it was shown that 20% of mothers had hemoglobin < 12 g/dl at the beginning of pregnancy, which showed a lower rate of anemia. Higher prevalence of iron deficiency anemia among women in developing countries has been shown before (2). A population-based prenatal care program in China also showed a prevalence of anemia (Hb < 110 g/L) of 22.1% in the first trimester, which is lower than the prevalence of anemia in this study (4).
The study results also showed that based on serology IgG test for diagnosis of H. Pylori, more than half of participants were positive. A community-based cross-sectional study among adults in Southern Brazil using 13C-UBT to diagnose H. pylori, showed that 70.7% (68.0-73.6%) of participants were positive for H. Pylori (15), which shows a higher prevalence rate than that of this study. This difference may represent different diagnosis techniques that were used in these two studies. A study in United State based on National Center for Health Statistics (NHANES) data and using serological diagnosis technique showed that the rate of H. pylori infection was 27.1% percent (95% CI: 24.8, 29.4) in the study population (18), a study in Germany (17) among pregnant women showed that 23% of the 898 mothers had a H. pylori infection, which is similar to the findings in United States, but much lower than the findings of this study.
The results of this study showed that the risk of iron deficiency anemia among pregnant women with H. Pylori infection was 3.18 (95% CI: 1.52-6.6) times more compared to those who were not infected. Another study on this subject in Iran, which was conducted in Mashad city (5), showed that infection with H. pylori increases the chance of iron deficiency anemia by 2.2 times. A meta-analysis of twelve case reports and case series, 19 observational epidemiologic studies and six intervention trials by Muhsenand Kohen (19) showed an increased risk for iron deficiency anemia; pooled odds ratio (OR) 2.8 (95% confidence interval (CI) 1.9, 4.2) and also for iron deficiency; pooled OR 1.38 (95%CI 1.16-1.65) among H. pylori-infected subjects, which is lower than the results of this study. A community-based cross-sectional study among adults
in Southern Brazil showed that H. pylori infection was associated with a reduction in hemoglobin level, however this reduction was not significant (15). A study in United States showed that H. pylori infection was associated with a 40% increase in the prevalence of iron deficiency after controlling for relevant covariates (18). A study in Germany, also showed an inverse association between H. pylori infection and hemoglobin level at the beginning of the pregnancy was observed both among German women and among women with other nationalities (17). It seems that most studies show an association between iron deficiency anemia and H. Pylori infection; however the reported level of this association is different. It seems that geographic and socioeconomic statuse of individuals are factors that influence the effect of H. Pylori on iron deficiency anemia.
This study also showed that H. Pylori infection is associated with an increased risk of pregnancy related severe vomiting and nausea.
A study by Alimi-Khayati on H. pylori sero-positivity and the incidence of hyperemesis gravidarum in Rasht city of Iran, found no correlation between sero-positivity for H. pylori and the time of onset or duration of hyperemesis gravidarum symptoms, although more patients with hyperemesis gravidarum were seropositive for H. pylori infection than controls (20). Another study in Iran by Kazerooni et al. showed that there was a significant association between H. pylori infection and hyperemesis gravidarum in hyperemetic pregnant patients (21).
Golberget al. in a systematic review of fourteen case-control studies, involving 1,732 participants and controls tested for H pylori infection, concluded that there is an association between hyperemesis gravidarum and H pylori infection (22). Another systematic review and meta-analysis of case-control studies by Sandven et al. showedsimilar results (23).
In conclusion this study showed that infection with H.Pylori increases the risk of iron deficiency anemia among pregnant women. There was a reverse linear correlation between IgG of H. Pylori and hemoglobin and ferritin level. (Although we should emphasis that results may not beapplicable and expanded to general population).
Also this study showed that the risk of severe vomiting and nausea in the first trimester increases significantly among those who are infected with H. Pylori.