1. Background
Acquired immune deficiency syndrome (AIDS), as the fourth leading cause of death in the world, has a tremendous impact on the mortality rate of women of childbearing age (1). According to the United Nations Statistics, by 2013, 35.3 million people were infected with AIDS worldwide, more than half of whom were females (2). Accordingly, every minute, a young woman gets infected with human immunodeficiency viruse (HIV) through sexual contact. The incidence of HIV in women with unstable sexual partners is 13.5 times greater than that in other females. Moreover, this rate is 50% higher in the females injecting drugs (3).
Social inequities, such as poverty and economic dependence, violence and threats, high-risk sexual relationships, limited power and discretion, and lack of influence on decision making reduce women's ability to protect themselves against AIDS (4, 5). Meanwhile, women who are in charge of family due to reasons like divorce or husband's death, addiction, disability, neglect, and abandonment are more vulnerable to such harms (6).
Poverty, improper economic condition, and heavy burden of responsibilities because of performing a dual role (both as a mother and a father) are considered as serious threats to the health of the female householders (7). Family breakdown and spouse's addiction or unemployment set the ground for high-risk sexual behaviors, whether with the spouse or with multiple sexual partners (8).
Statistical data in Iran are indicative of the increasing trend of female-headed households in the last decade. Accordingly, the rate of female-headed households in Iran increased from 9.5% in 2006 to 12.1% in 2011 (6). On the one hand, based on the electronic registration system, the pattern of AIDS infection in males and females has undergone a change in recent years. In this regard, the incidence of AIDS has increased by 10% and reached to 29.2% (9).
Based on the scientific resources, the implementation of health education and enhancement of knowledge are the only effective ways to fight against AIDS before the outbreak of this disease. As stated by the World Health Organization, such trainings are effective as they can cause behavioral change in these groups (10).
According to the behaviorist theory, the development of a model-based educational program can play a significant role in the promotion of people's knowledge and beliefs about health behaviors, which is the prerequisite for changing unhealthy behaviors or adopting preventive behaviors (11). Health belief model (HBM) is a comprehensive model for disease prevention. Based on this model, an individual’s decision to perform a health behavior is affected by his/her perception of a threat, sensitivity and severity of an illness, as well as the health value of the behavior (12). This model consists of six components, including perceived sensitivity, perceived severity, perceived benefits, perceived barriers, self-efficacy, and cues to action (11).
The literature review showed numerous studies investigating the application of HBM in AIDS preventive behaviors in Iran. However, during the search, we did not find an article similar to the present one. The growing trend of HIV infection among females can expose a larger population to this threat through its transmission to newborns or multiple sex partners. The increasing number of female householders that are considered as a vulnerable group due to being in dire economic and social situations highlights the need to perform a study investigating HBM as an effective model for preventing AIDS. With this background in mind.
2. Objectives
The present study was conducted to determine the effect of an HBM-based educational intervention on the adoption of HIV preventive behaviors among female householders in Zahedan, Iran.
3. Methods
This quasi-experimental study was carried out among 70 female householder under the support of Imam Khomeini Relief Foundation of Zahedan from October to March of 2011. The study was approved by the Research Committee of Shahid Beheshti University of Medial Sciences Tehran, Iran (code number: IR-SBMU.PHNM 1395, 497). The sample size was estimated as 70 cases using the formula below, considering a confidence level of 95% and a test power of 80% and based on a study performed by Ebrahimipour et al. (13).
For sampling, two regions were randomly selected from the four areas covered by the Zahedan Relief Foundation. Then, out of the two selected regions, a list of 150 female householders who were eligible and willing to enroll in the study was prepared. In the next step, 70 subjects were randomly selected from the given list using SPSS software (version 21). The participants were then assigned into the two groups of control (n = 35) and intervention (n = 35) by means of Excel software.
The inclusion criteria were Iranian nationality and being head of household for a minimum of one year. The exclusion criteria included non-cooperation, affliction with a specific physical or mental illness, and absence from the training sessions. The data were collected through a researcher-made questionnaire consisting of three sections, demographic information (15 items), HIV knowledge (21 items), and HBM components (48 items). The scoring of HIV knowledge questionnaire was performed by assigning the scores of one and zero to the items responded as “yes” (i.e., proper level of awareness) and “no/not sure”, respectively. Furthermore, regarding the HBM construct section, all the six components of this model were rated on a five-point Likert scale (i.e., completely agree = 5, agree = 4, no idea = 3, disagree = 2, and completely disagree = 1).
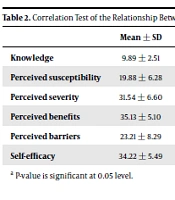
The validity of the questionnaire was confirmed by a panel of 10 professors of Reproductive Health Education in Shahid Beheshti University of Medical Sciences, Tehran, Iran. To determine the reliability of this instrument, it was filled out through interview by 30 women who were not included in the study, and then Cronbach's alpha coefficient was calculated. In this regard, knowledge, perceived sensitivity, perceived severity, perceived benefits, perceived barriers, self-efficacy, and guidance for action had the Cronbach's alpha coefficients of 0.74, 0.75, 0.90, 0.81, 0.81, 0.78, and 0.77, respectively.
The control group was subjected to no interventions. On the other hand, the intervention group was divided into two groups of 12 and 11 cases, receiving two 90-minute training sessions held at the center of Imam Khomeini Relief Foundation. The educational intervention was implemented using the lecture method entailing group discussion, question and answer, educational pamphlet, as well as video and photo presentation in two weeks.
In order to improve the sustainability of the contents, they were gathered in a pamphlet and submitted to the intervention group after the end of the program. Prior to the intervention, the intervention and control groups filled out the questionnaire. The two groups again completed the awareness and HBM sections one month after the end of the intervention.
In line with the ethical considerations, informed consent was obtained from all the participants, and the questionnaires were filled out anonymously. In addition, after the completion of the study, the educational pamphlets were provided to the participants in the control group. The present study was approved by the Iranian Registry of Clinical Trials with the code of IRCT20161126031105N2. The data were analyzed in SPSS software (version 21) using descriptive and inferential statistics, including chi-square test, independent t-test, paired samples t-test, and univariate analysis of variance (UNIANOVA). Additionally, the Kolmogorov-Smirnov test was used to test normality of the data.
4. Results
According to the results, the mean ages of the intervention and control groups were 34.65 ± 5.74 and 32.57 ± 5.42 years, respectively. The mean age at marriage and the number of children were 18.34 ± 3.18 and 4.28 ± 2.23 in the intervention group and 17.22 ± 1.76 and 4.54 ± 2.47 in the control group, respectively. In addition, the mean duration of heading the household in the intervention and control groups was 4.40 ± 1.80 and 4.62 ± 1.61 years, respectively. The results of the independent t-test revealed no significant difference between the two groups in terms of age, age at marriage, number of children, and heading duration (P > 0.05).
Regarding educational level, 71.4% (n = 25) and 57.1% (n = 20) of the subjects in the intervention and control groups had less than 6 years of education, respectively. In terms of the income status, 65.7% (n = 23) and 80% (n = 28) of the intervention and control groups had an income level of less than 500000 tomans. In the intervention and control groups, 51.4 (n = 18) and 54.3% (n = 19) of the participants were widows, and 91.4% (n = 32) and 97.1% (n = 34) of them were housewives, respectively.
Based on the chi-square test, no significant difference was observed between the two groups regarding education, income, employment, and marital status (P > 0.05). Furthermore, the results of the independent t-test indicated no significant difference between the intervention and control groups in terms of the mean scores of knowledge and HBM components at the pre-intervention stage (P > 0.05). However, these variables were significantly different between the two groups after the intervention.
Moreover, according to the paired samples t-test, the mean scores of knowledge and HBM components were significantly different in the intervention group at the post-intervention stage (8.65 ± 2.30), compared to those at the pre-intervention stage (2.54 ± 1.80). Nonetheless, this difference in mean scores was not statistically significant in the control group at the post-intervention stage compared to the pre-intervention stage (2.97 ± 1.45 vs. 2.42 ± 1.89; Table 1).
Table 1.
Comparison of the Mean Knowledge and Health Belief Construct Scores Between the Control and Intervention Groups and Between the Pre-and Post-Intervention Stagesa
| Variable | Pre-Intervention | One Month Post-Intervention | P Valueb |
|---|---|---|---|
| Knowledge | |||
| Intervention | 2.54 ± 1.80 | 8.65 ± 2.30 | < 0.001 |
| Control | 2.42 ± 1.89 | 2.97 ± 1.45 | 0.341 |
| P valuec | 0.726 | < 0.001 | - |
| Perceived sensitivity | |||
| Intervention | 26.31 ± 4.52 | 30.91 ± 4.24 | 0.008 |
| Control | 26.48 ± 3.79 | 25.40 ± 3.94 | 0.097 |
| P valuec | 0.058 | < 0.001 | - |
| Perceived severity | |||
| Intervention | 27.88 ± 11.88 | 32.22 ± 4.75 | 0.001 |
| Control | 28.71 ± 7.17 | 29.74 ± 4.95 | 0.068 |
| P valuec | 0.115 | < 0.002 | - |
| Perceived benefits | |||
| Intervention | 25.28 ± 6.61 | 31.71 ± 3.66 | < 0.001 |
| Control | 28.11 ± 6.10 | 29.37 ± 5.96 | 0.142 |
| P valuec | 0.062 | < 0.001 | - |
| Perceived barriers | |||
| Intervention | 33.14 ± 5.69 | 23 ± 5.26 | < 0.001 |
| Control | 35.31 ± 3.41 | 35.40 ± 2.93 | 0.098 |
| P valuec | 0.068 | < 0.001 | - |
| Self-efficacy | |||
| Intervention | 25.31 ± 6.79 | 31.25 ± 5.29 | < 0.001 |
| Control | 26.48 ± 3.79 | 28.34 ± 6.42 | 0.324 |
| P valuec | 0.690 | < 0.001 | - |
| Guidance for action | |||
| Intervention | 27.11 ± 4.72 | 31.74 ± 4.83 | < 0.001 |
| Control | 28.71 ± 5.17 | 4.66 ± 28.14 | 0.613 |
| P valuec | 0.431 | < 0.001 | - |
aValues are expressed as mean ± SD.
bPaired samples t-test.
cMann-Whitney U test.
To perform UNIANOVA, first, the normality of the knowledge and HBM components scores were investigated through Levene’s test. Given that the significance levels were greater than 0.05 for all the cases, the heterogeneity of variances was rejected. As a result, UNIANOVA was used to determine the effect of the variables of training, marital status, educational level, heading duration, and income status on the mean scores of knowledge and HBM components in the two groups.
Based on the F value, there was a significant difference in the knowledge (P = 0.001, F = 84.18), perceived sensitivity (P < 0.001, F = 21.75), perceived severity (F = 9.77, P < 0.003), perceived benefits (P < 0.001, F = 61.06), perceived barriers (P < 0.001, F = 401.88), self-efficacy (P < 0.001, F = 49.02), and guidance for action (F = 35.42, P < 0.001) scores between the two groups. According to Table 1, it can be concluded that training could increase the knowledge and HBM components scores in the intervention group. However, none of the demographic variables significantly affected the knowledge and HBM components scores in the two groups (P > 0.05).
5. Discussion
The present study was conducted to determine the impact of an educational intervention based on HBM on adopting HIV preventive behaviors in the female heads of households in Zahedan. To the best of our knowledge, this is the first attempt to investigate the impact of training on AIDS prevention behaviors based on the HBM in the female householders; therefore, the results were compared with those of other studies investigating this model among other populations.
In the present study, the educational intervention had a positive effect on the enhancement of knowledge mean score in the intervention group. Likewise, in a study conducted by Zhao et al., HBM-based education was reported to have a positive impact on increasing awareness about the role of continuous condom use in preventing AIDS among female prostitutes (14).
In another study evaluating the effect of an educational intervention based on the self-efficacy theory on adopting HIV preventive behaviors in high-risk women, Ebrahimipour et al. introduced education to vulnerable women as the most effective strategy to raise awareness and improve performance of these women (13). The results of the aforementioned studies were in line with those of the present study regarding the effect of education on awareness.
In the current study, the HBM-based educational intervention was effective in perceived sensitivity among the female heads of households. In other words, after the educational intervention, the majority of the female householders were more sensitive toward AIDS and considered this illness as a serious risk that could affect everyone in case of lack of care. Our results are in congruence with those obtained by Kellam et al. (15) and Downing-Matibag and Geisinger (16).
However, our findings are inconsistent with the results reported by Kharazi and Peyman evaluating AIDS preventive behaviors based on the HBM among high school girls (17). The discrepancy in results can be due to the difference in the target population. In this regard, adolescents have lower probability of high-risk behaviors, such as drug injection; therefore, the creation of sensitivity in this age group requires a more extensive education . The creation of a high level of perceived sensitivity promotes the individuals’ motivation to adopt preventive behaviors. Consequently, a part of AIDS education should be centered on this concept.
The results of the present study were also indicative of the enhancement of the mean perceived severity score in the intervention group after the educational program in comparison to that in the control group. This finding suggests that the participants considered AIDS as untreatable and fatal with heavy social consequences, even if they did not consider themselves to be at risk of this disease. One of the reasons for using the HBM for AIDS is the unfortunate consequence of this disease that urges people to seek to adopt preventive behaviors. This is in agreement with the findings of a previous study (18).
The enhancement of the mean perceived benefits score after the intervention and lack of such a change in the control group were suggestive of the effect of our educational intervention on the female heads of households. Borawski et al. reported that improved perception of the benefits of AIDS prevention methods would lead to increased self-confidence, proper use of condom, and adoption of more effective preventive behaviors (19).
In another study carried out by Abbaspour et al., improved perceived benefits was reported to reduce the high-risk behaviors associated with AIDS in the vulnerable group (20). It seems that our educational intervention could clearly elucidate the benefits of adopting AIDS preventive behaviors for female heads of household through holding question and answer and group discussions.
In this study, the reduction of the perceived barriers mean score after the intervention indicated the importance of training on AIDS prevention. This finding is consistent with the results reported by Lance Coleman (21) and Baghianimoghaddam et al. (22). However, the results of this study were inconsistent with those of the study by Ghafari (23). Significant differences in perceived barriers, including physical, material, psychological and social barriers, and the different effects of educational interventions on modifying these barriers could have contributed to such inconsistency. In other words, barriers such as cost, lack of access to services, and social stigma, which are external or out of individual’s will were not expected to be moderated by training interventions. The modification of misconceptions and conceptualization of correct behaviors can be helpful in AIDS prevention. Dillard believes that it is difficult to change a behavior until the perceived barriers are overcome (24).
It seems that even with high level of perceived benefits, behavioral change will be difficult as long as the barriers to health behavior adoption are not resolved. Therefore, the alignment of these two constructs can make a huge contribution to the emergence of health behaviors. Some of the main barriers to adopting preventive behaviors include the fear of HIV-positive result, rejection from the family, lack of access to condoms, and misconceptions about reduced sexual pleasure in case of using condoms, which are the results of low knowledge level.
Our findings showed that the educational intervention led to a significant increase in self-efficacy in the intervention group, whereas no such a difference was observed in the control group. Bui et al. reported that the improvement of self-efficacy is effective in the rejection of risky suggestions related to HIV (25). Accordingly, Lance Coleman found a significant relationship between self-efficacy and adoption of preventive behaviors (21). Furthermore, Lance Coleman proposed self-efficacy as one of the key variables in adopting safe behaviors (21). In fact, these studies showed the positive effect of training intervention on self-efficacy, which is consistent with our findings. However, the results were inconsistent with those of the study by McClendon et. al, indicating no significant change in self-efficacy structure (26).
In general, self-efficacy is a mediating factor between learning and health behaviors. In fact, it indicates one’s belief in his/her ability to successfully adopt health behaviors. Since participation in group discussions and the use of others' experiences lead to self-confidence in individuals, they are helpful in promoting the sense of self-efficacy. However, the target population, the type of training and its content, the social, cultural, and even the physical and psychological conditions in which one is located can affect self-efficacy and cause contradictions (27).
Another finding of our study was the significant enhancement of mean guidance for action score in the intervention group, compared to that in the control group. As the findings indicated, the recommendations of the medical staff were the most important guidance for increasing AIDS preventive behaviors. The key role of health professionals in delivering health care services is indicative of the paramount importance of this group in enhancing AIDS preventive behaviors. Therefore, the implementation of educational workshops and programs for the relevant experts with the aim of equipping them with sufficient information seems essential.
One of the strengths of the present study was addressing important issues, such as AIDS and female householders based on the HBM. On the other hand, the most important limitation of this study was the lack of similar studies for comparative purposes. Therefore, considering the importance of these issues, it is suggested that similar studies be conducted using this model and other training models in order to control, monitor, and implement such trainings and compare them with the common educational plans. The implementation of such investigations would facilitate the promotion of preventive behaviors and health status of female householders as a vulnerable group.
5.1. Conclusions
While fighting against the spread of AIDS, information is a powerful tool. According to the findings of this study, the educational program designed based on the HBM has been effective in reducing perceived barriers, increasing the level of awareness, perceived sensitivity, perceived severity, and perceived benefits, and promoting AIDS preventive measures among the female heads of household. Training using this model was effective in improving people's perception and belief, and through behavior modification, it could prevent the spread of the disease and its complications in the community. In addition to this model, planning is also recommended to eliminate the preventive behavior barriers through theories and other behavior change models at individual and organizational levels.