1. Background
Osteoarthritis (OA) is one of the most common musculoskeletal diseases that could cause pain, joint swelling, impaired muscular stability, functional disability, and reduced quality of life (QOL). In severe cases, there is a loss of articular cartilage, subchondral bone, and all intra-articular synovial tissues (1). Knee is the most common joint that is affected by osteoarthritis (2). Knee OA is the most common articular disease that leads to an impaired QOL (3).
The progressive nature of the disease and its associated pain and disability significantly influences the ability of the individual to carry out daily activities (4, 5). These conditions cause pain, reduced function and mobility in the patient, hence, leads to limitation in activities, such as walking, climbing stairs, and sitting, bending or lifting; this results in restrictions in social activities and consequently inevitable impaired QOL (3, 6).
The treatment is usually focused on reducing pain and improving physical function with multiple drugs, non-drug, and surgical approaches. Pharmacologic therapies for pain control in knee OA include topical or oral NSAIDs, intra-articular injections of corticosteroids, hyaluronate, and opioids, and modulators of osteoarthritis, including glucosamine compounds (7). The proper treatment with minimal side effects and acceptable efficacy is still not defined.
Magnetic resonance imaging (MRI) studies have shown that synovitis is very common in knee OA and is associated with the related pain and its severity (8-11). Methotrexate (MTX) is an effective and commonly used disease-modifying agent for inflammatory arthritis with favorable long-term results (12). A few studies have addressed low-dose MTX in OA (13-15), each with different outcomes. Considering the effects of MTX in the treatment of inflammatory arthritis and the role of inflammation in OA, it seems that MTX use in the treatment would be beneficial.
2. Objectives
This study aimed at evaluating the effects of MTX on the control of pain and improvement of QOL in patients with moderate to severe knee OA.
3. Methods
In this randomized placebo-controlled clinical trial, 100 patients with moderate to severe OA visiting rheumatology clinics were recruited. Patients between 45 and 75 years of age with moderate to severe knee OA with non-inflammatory joint effusions according to fluid analysis, who were able to walk with peripheral knee pain and who scored more than five by numerical rating scale (NRS) or more than 48 by WOMAC were included in the study. The patients had radiographic evidence of OA with Kellgren-Lawrence score of III to IV (moderate to severe) on x-ray. Exclusion criteria were having other rheumatologic disease, other knee or periarticular disease, lower limbs fracture with knee joint involvement, OA of the hip and ankle, history of knee surgery or trauma, radicular pain, intraarticular corticosteroid injection or physiotherapy in the previous three months and hyaluronic injection in the previous six months, psychiatric disorders, balance, neurologic sensory and/or neurologic deficit, and patients with any type of malignancy. This research also excluded patients with underlying systemic disease, such as renal, hepatic or heart failure, uncontrolled blood pressure, diabetes mellitus, and severe asthma in need of corticosteroids use. Patients with corticosteroids use in the last six weeks prior to the study and those with allergic reactions to MTX or its derivatives were also excluded. The ethics committee of Ardabil University of Medical Sciences approved the study protocol (approval number: IR.ARUMS.REC.1396.150) and registered at the Iranian Registry of Clinical Trials under the code of IRCT20170716035126N1; informed consent was obtained from all of the individuals.
The study sample size for each group was calculated as 44 cases considering an effect size of d ≥ 0.60 as statistically significant in a two-tailed test with α = 0.05 and power of 0.90. As there was possibility that some patients do not complete the study, the researchers included 50 patients in each group. Using random number blocks and sealed envelopes, patients were enrolled in the study according to the sample size (Figure 1). All patients completed the study period yet nine patients in the MTX group were excluded from the final analysis as all of them in the last visit reported corticosteroid use during the study period.

Figure 1.
CONSORT flow diagram of the study
In both groups, glucosamine sulfate 1500 mg daily was administered; as well as, MTX 7.5 mg (three pills) weekly with subsequent increase to 15 mg weekly after the first month in the intervention group or placebo, three pills weekly in the control group with subsequent increase to six pills after the first month. All patients in both groups also received folic acid 1 mg daily. The total treatment period was six months. Participants and the physician assessing the outcome of the study were blinded to the allocated groups.
Before the study, after the first month, and then every three months, blood samples were obtained from all patients to measure complete blood cell count, liver function tests, blood urea nitrogen, and creatinine for possible change in their values and any contraindication for MTX use or its dosage adjustment. The researchers measured common side effects of MTX as decrease in blood counts, gastrointestinal complications (nausea, vomiting, diarrhea, and mouth ulcers) and increase in liver enzyme and hepatitis.
Patients were allowed to use NSAIDS only in the first three months until the MTX effect occurred and were prohibited to use corticosteroids at any time during the study period.
The study outcome was measured before, at three months, and six months after the intervention. During these periods, pain severity, functional status, and quality of life were measured using the NRS, WOMAC, and SF-12 questionnaire, respectively. The NRS is the simplest and most commonly used numeric scale, in which the patient rates pain from 0 (no pain) to 10 (worst pain).
The WOMAC questionnaire includes 24 questions that measure the three dimensions of pain (five items), stiffness (two items), and physical function (17 items). Each question is based on a five-point Likert scale resulting in total number range of 0 to 96. With increase in the severity of the disease, the points are increased (16). The Persian format of the WOMAC questionnaire was validated previously (17).
The SF-12 questionnaire is the short form of SF-36 Quality of Life (QOL) questionnaire, which is widely used to measure QOL in different diseases. Due to the small number of items, the overall score is often used. The questionnaire examines the QOL in terms of overall understanding of their health, physical functioning, physical health, emotional problems, physical pain, social function, vitality, and mental health. Montazeri et al. (18) evaluated validity and reliability of the Persian version of SF-12 among the Iranian population.
3.1. Statistical Analysis
All data were analyzed using SPSS 20 (version 22; SPSS Inc., Chicago, IL). The results are expressed as mean ± standard deviation or percentage. Kolmogorov-Smirnov test was used to assess the normal distribution of data. Chi square test, Fisher’s exact test, independent t-test or Mann-Whitney U test were used to compare data between groups. Repeated measure analysis of variance (ANOVA) was used to compare serial changes in parameters during the study period in each and between groups. P values of less than 0.05 were considered statistically significant.
4. Results
Both groups were comparable regarding demographic and baseline clinical data (Table 1).
Table 1.Demographic and Baseline Clinical Data Od Study Groupsa
| Methotrexate, (N = 41) | Placebo, (N = 50) | P Value | |
|---|---|---|---|
| Age, y | 53.75 ± 6.59 | 52.42 ± 7.19 | 0.31 |
| Gender | 0.89 | ||
| Male | 15 (36.6) | 19 (38) | |
| Female | 26 (63.4) | 31 (62) | |
| Disease duration, y | 8.34 ± 3.63 | 7.16 ± 4.11 | 0.15 |
| Kellgren-Lawrence score | 0.31 | ||
| III | 21 (51.2) | 31 (62) | |
| IV | 20 (48.8) | 19 (38) |
aValues are expressed as mean ± SD or No. (%).
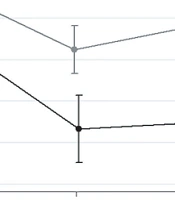
The two groups were also comparable regarding pain score according to NRS before the intervention (7.65 ± 1.21 in MTX versus 7.46 ± 1.38 in placebo, P = 0.47). After the intervention, there was a significant serial reduction in NRS score (Figure 2) with no difference in NRS after three months between groups (P = 0.052) and with final NRS of 4.09 ± 1.24 versus 5.30 ± 1.56 in MTX and placebo groups, respectively. The MTX group had significantly greater reduction in NRS than the placebo group (P < 0.001).

Figure 2.
NRS changes during the study in both groups
The total WOMAC and its subscales before, at three months, and six months after the intervention are shown in Table 2. Before the intervention, there was no significant difference between groups, while during the three months and six months evaluations, total and its subscales scores were significantly lower in the MTX group as compared to the placebo group. Evaluating the serial changes between groups also showed significant improvement in the total WOMAC and its subscales in the MTX group as compared to the placebo.
Table 2.WOMAC Total Score and its Subscales Before, Three Months, and Six Months After the Intervention Between the Groupsa
| Methotrexate Group, (N = 41) | Placebo Group, (N = 50) | P Value | |
|---|---|---|---|
| WOMAC total | |||
| Before | 64.46 ± 4.60 | 66.16 ± 5.64 | 0.12 |
| 3 months after | 57.56 ± 6.12 | 65.60 ± 8.29 | < 0.001b |
| 6 months after | 38.46 ± 4.24 | 57.82 ± 7.12 | < 0.001b |
| WOMAC Subscales | |||
| Pain | |||
| Before | 13.19 ± 1.52 | 13.88 ± 2.00 | 0.07 |
| 3 months after | 11.65 ± 1.40 | 13.76 ± 2.21 | < 0.001b |
| 6 months after | 8.00 ± 2.56 | 12.84 ± 1.96 | < 0.001b |
| Stiffness | |||
| Before | 5.51 ± 0.92 | 5.66 ± 1.11 | 0.50 |
| 3 months after | 4.63 ± 1.44 | 5.38 ± 0.98 | 0.004b |
| 6 months after | 4.63 ± 1.44 | 5.40 ± 0.96 | 0.004b |
| Physical function | |||
| Before | 45.75 ± 3.91 | 46.62 ± 5.62 | 0.4 |
| 3 months after | 41.26 ± 5.03 | 46.44 ± 6.56 | < 0.001b |
| 6 months after | 27.02 ± 3.45 | 39.90 ± 5.80 | < 0.001b |
Abbreviation: WOMAC, western ontario and mcmaster universities arthritis index.
aValues are expressed as mean ± SD.
bP is two-sided significant.
The two groups had similar SF-12 score before the intervention, yet there was significantly higher SF-12 score indicative of better QOL at six months, yet not three months after the intervention in the MTX group (Table 3). The serial changes were also significantly better in the MTX group (P < 0.001).
Table 3.SF-12 Score Before, Three Months and Six Months After the Intervention Between Groupsa
| SF-12 Score | Methotrexate Group, (N = 41) | Placebo Group, (N = 41) | P Value |
|---|---|---|---|
| Before intervention | 19.48 ± 1.58 | 19.06 ± 1.82 | 0.24 |
| Three months after | 24.17 ± 2.50 | 23.28 ± 2.17 | 0.07 |
| Six months after | 29.24 ± 2.77 | 24.96 ± 4.38 | < 0.001b |
aValues are expressed as mean ± SD.
bP is two-sided significant.
During the study period, nine patients (22%) from MTX group and 18 patients (36%) from placebo group used NSAIDS and analgesics for pain reduction with no significant difference between the groups (P = 0.14).
No patients reported MTX side effects.
5. Discussion
This study examined the efficacy of MTX in controlling pain and QOL in patients with moderate to severe knee OA. The results of this study showed a significant reduction in pain intensity in patients based on NRS and pain subscales of WOMAC, along with improved QOL following treatment with MTX for six months.
Pavleka et al. (14) in their study on the treatment of erosive hand OA showed a marked decrease in pain intensity following treatment with 10 mg MTX, weekly. Wenham et al. (15) in their study on 30 patients with knee OA treated with an initial dose of weekly MTX 7.5 mg and subsequent increase up to 20 mg weekly for 24 weeks, showed a significant pain reduction in almost 60% of the patients, while in 13% of the patients, the symptoms were worsened. Unlike these studies, Holanda et al. (13) found no statistically significant difference in pain intensity based on VAS between patients treated with 7.5 mg MTX weekly or placebo.
Kingsbury et al. (19) previously published a detailed description of a Phase III trial on the effectiveness of MTX on 160 patients with knee OA; although researchers completed the recruitment phase, no research results have been provided yet.
Differences in study sample size, inclusion and exclusion criteria, and MTX dosage used in various studies can somehow justify differences between studies. It can be concluded that MTX at higher doses has the ability to control pain in patients with moderate to severe knee OA. Since the results of the Kingsbury et al. study have not been reported yet, the present study had the highest sample size compared to the other studies, with acceptable results.
This study used the WOMAC questionnaire for better evaluation of the MTX efficacy during the intervention. The results showed a more significant decrease in the overall WOMAC score and its subscales of pain and physical function in the MTX group compared to the placebo group.
Similarly, Wenham et al. (15) found a significant improvement in physical function and a significant reduction in pain severity three months and six months after the treatment, respectively. However, there was no significant improvement in physical function after the third month as compared to six month after treatment. In Holanda et al.’s study (13) there was no significant difference between the two groups in terms of the WOMAC score. In contrast, the researchers observed a significant decrease in overall score and in both pain and physical function subscales following treatment with MTX.
The NRS is a one-dimensional scale, which evaluates the severity of pain from the perspective of the patient at the time of assessment. On the other hand, WOMAC consists of three subscales including pain, stiffness, and physical function with questions covering daily activities. Therefore, the evaluation by the WOMAC scale seems to be more comprehensive. Due to the reduction in the intensity of pain and the improvement of the WOMAC physical function, MTX may be useful in treating moderate to severe knee OA.
The QOL of patients with knee OA is directly related to the severity of their pain and therefore, it is expected that pain relief would improve their QOL. In a study by Manoy et al. (20) a significant decrease in the pain intensity of knee OA patients after treatment with vitamin D was reported, which was accompanied by improved QOL based on the SF-12 questionnaire. In the present study, there was a significant improvement in patients’ QOL based on SF-12 questionnaire at the end of six months in the group treated with MTX.
The researchers found no significant difference in the number of NSAIDs used between the two groups, although there was a lower tendency for consumption in the MTX group. Holand and colleagues (13) also did not report any significant differences between MTX and placebo groups in terms of paracetamol consumption, although there was a tendency to consume more paracetamol in the placebo group.
Furthermore, a relative improvement in the severity of pain and total WOMAC and its subscales score were observed in the placebo group following the treatment, which could be explained by the placebo effect, the role of empathy in treatment, and the effect of concurrent treatment with glucosamine (although controversial), rather than the chance factor.
In addition, although not considered in this study, appropriate health care and preventive measures, such as proper diet, exercise and weight loss, can contribute to the improvement of symptoms in the placebo group.
Several studies have assessed the effect of weight loss and physical function on knee OA patients (21-23). Weight loss using aerobic exercises as well as proper diet are recommended in guidelines for knee OA patients. A review study concluded that weight loss results in pain relief and functional improvement in elderly patients with knee OA (22).
Knee OA is common among elder populations, whom would have comorbidities and the medications used would have more complications and side effects. Therefore, it is important to ensure safety of drugs before administration and choose options with minimum or no side effects and with long-term benefits (24). Furthermore, MTX is well tolerated for long term use and concomitant folic acid use reduces side effects (19). As the researchers observed no significant side effects of MTX use during the study period, along with its efficacy in reducing pain and improving QOL, it seems a suitable medication for knee OA.
The strength of this study can be attributed to its randomized clinical trial design and its prospective nature. However, this study also has some limitations, including but not limited to sample size of the study (although higher than the other studies), the duration of the study, and the lack of patient follow up after the completion of the treatment. Although nine patients from the MTX group were excluded from the study due to corticosteroid use, which can be indicative of a selection bias during sampling process, yet all these nine patients had moderate knee OA and were not those with severe OA.
5.1. Conclusions
Treatment of moderate to severe knee OA with MTX could reduce pain severity and improve functional status and quality of life in such patients.