This study extensively examined the effect of RTX on infectious complications and the survival of children with malignancy. The findings highlight the significant clinical impact of RTX treatment on the incidence of FN events, which are often associated with more severe infectious outcomes (
19). Our research supports the notion that the risk of bacterial and fungal infections escalates alongside the risk of FN. Thus, additional preventive measures are recommended for patients not traditionally viewed as being at high risk for fungal infections, such as children with CD20+ lymphoma (
19,
20). Notably, Cox proportional hazards models revealed that fungal infections posed the highest adjusted hazard risk, nearly 2.7 times greater than the adjusted risk for bacterial BSI (4.3 vs. 1.6). Later in this section, we will delve into existing research on the influence of RTX treatment on bacterial BSI risk, noting the scarcity of information regarding its effect on IFIs.
The data on the impact of RTX on infectious complications and the survival of patients receiving immunosuppressive therapy are mixed. While some studies align with our findings, others remain inconclusive, suggesting that our study could contribute additional insights for managing cancer patients undergoing RTX treatment concurrently. Lee McAtee et al. reported that among pediatric patients treated with RTX, there was an increased risk of infections associated with the simultaneous use of chemotherapy (adjusted hazard ratio [aHR], 2.35; 95% CI, 1.33 - 4.04; P < 0.001). Infections were observed in 47.9% (224/468) of cases; severe infections occurred in 17.9% (84/468), and death in 0.6% (3/468). They noted that B-cell recovery (CD19+ or CD20+ cell count normalization) typically took about 9.0 months (interquartile range, 5.9 - 14.4 months) after RTX treatment (
17).
Lanini et al. found that RTX significantly elevated the risk of both infection and neutropenia in patients with lymphoma or other hematological malignancies (
21). A prospective randomized trial by Van Oers et al. indicated a higher frequency of infections and neutropenia among RTX-treated patients compared to those not exposed to RTX, offering more comprehensive data on the subject (
22). Additionally, a study by Nissen et al. showed a notably higher incidence of infectious complications in patients receiving a combination of RTX and chemotherapy versus those on RTX monotherapy. They reported no significant differences in the number of RTX courses or cumulative RTX doses between treatment episodes with and without infections (
14).
In contrast, a meta-analysis indicated that incorporating RTX into standard chemotherapy protocols did not alter the overall risk of severe infections or survival (
13). Similarly, a systematic review of 9 randomized controlled trials (RCTs) by Rafailidis et al. found no significant increase in the incidence of infections among those treated with RTX for B-cell non-Hodgkin lymphoma (NHL) (
23). These divergent findings could stem from the absence of an unexposed control group, a limited follow-up period, or a small sample size. Additionally, we identified two other studies, one by Witzens-Harig et al. focusing on adult patients with follicular lymphoma (
24) and another by de Souza et al. examining adults with NHL (
25). Witzens-Harig et al.'s study highlighted that RTX did not lead to severe or uncommon infections in adult follicular lymphoma patients. Conversely, de Souza et al. reported an increased vulnerability to respiratory infections in adults treated with RTX for NHL.
Research on the clinical effects of RTX on the risk of infectious outcomes in patients with immune thrombocytopenic purpura (ITP) is limited. A systematic review by Arnold et al. reported that 2.3% of patients developed severe infections, but it's important to note that many of these patients were also taking other immunosuppressants concurrently, making it difficult to attribute these outcomes solely to RTX (
26). Stabler et al. found an increased risk of infectious events following RTX treatment in patients with autoimmune diseases, including autoimmune cytopenias, with ITP patients comprising 18% (40/221) of the study population. However, no specific analysis focused on pediatric ITP patients was conducted. Infectious complications occurred in 19% (42/221) of the cases, with bacterial infections being the most common, followed by fungal infections (55% and 12%, respectively). Identified risk factors for severe infectious events included age, a history of diabetes, a history of cancer, concurrent steroid treatment, and a low CD4 lymphocyte count at the start of RTX treatment (
27).
Our study stands out as one of the few comprehensive investigations into the effects of RTX in pediatric patients with cancer and hematologic disorders, particularly focusing on various independent variables, notably the characteristics of immunosuppressive medications used.
This study faced several limitations. Firstly, a larger sample size would bolster our findings, as our study's sample size was relatively small. Our cohort also included a limited number of ITP patients, potentially skewing the results and necessitating cautious interpretation of these patients' outcomes. Secondly, the potential for selection bias must be considered, as the study predominantly included patients with CD20-positive B-cell non-Hodgkin lymphoma in the exposed group, not fully representing the target population. However, we sought to mitigate this bias by using adjusted statistical models that included underlying diseases as a covariate. Thirdly, as with other cohort studies, there may be unknown background risks or residual confounders affecting both the exposed and unexposed groups.
The majority of knowledge about RTX clinical effects on patients undergoing immunosuppressive chemotherapy comes from studies on adults. Additionally, the impact of simultaneous RTX treatment alongside other anticancer medications in children remains largely unexplored. Consequently, the findings of this study shed light on the specific and quantifiable effects of RTX on pediatric cancer patients. Our analyses offer a nuanced understanding of how the intensity and duration of RTX treatment influence both patient survival and the incidence of infection complications.
5.1. Conclusions
The addition of RTX to the treatment regimen of children receiving immunosuppressive chemotherapy for hematologic malignancies, especially CD20-positive B-cell lymphoma, has shown both additive and dose-dependent effects on clinical outcomes. However, due to potential uncontrolled biases and unrecognized background risks, these results should be approached with caution.










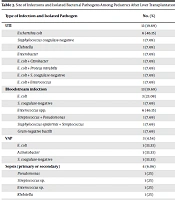
 administered prior to the onset of the first infectious events, including bloodstream infections (BSIs), febrile neutropenia (FN), and invasive fungal infections (IFIs). Differences were not statistically significant as determined by a one-way ANOVA.")
 between the RTX-treated group and the unexposed group.")
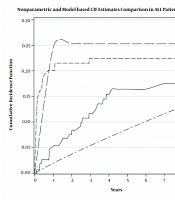
 of RTX treatment on bloodstream infections, according to the results from the Cox proportional hazards model.")
 of RTX treatment on febrile neutropenic events, as derived from the Cox proportional hazards model")
 of RTX treatment on invasive fungal infections, based on the Cox proportional hazards model")
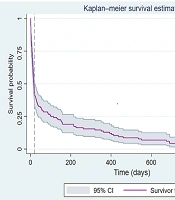
 of RTX treatment on patient survival, as determined by the Cox proportional hazards model")
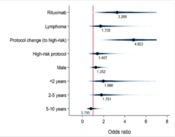
, according to multivariable logistic regression models adjusted for patient covariates. BSI: Bloodstream infection, FN: Febrile neutropenia, IFI: Invasive fungal infection.")
, based on multivariable logistic regression models adjusted for patient covariates")
 of RTX for mortality, according to the logistic regression model")