





1. Background
2. Objectives
3. Methods
3.1. Study Setting and Patients
3.2. Eligibility Criteria
3.3. Data Gathering
4. Results
4.1. Clinical Manifestations
4.2. Laboratory Data and Radiologic Findings
4.3. Mycobacterium bovis Evaluations
4.4. Immune System Evaluations
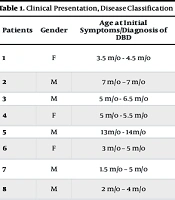
| Patients | Gender | Age at Initial Symptoms/Diagnosis of DBD | Systemic Syndrome (Clinical Presentation) | Mycobacterium Isolation (Site/Method) | DBD Classification | Immunodeficiency Type |
|---|---|---|---|---|---|---|
| 1 | F | 3.5 m/o - 4.5 m/o | Fever, rash, cough, LRTI, HSM, LAP (axillary, para-aortic), diffuse alveolar opacity on CXR | BMA positive (AFB smear) | Possible DBD | SCID |
| 2 | M | 7 m/o - 7 m/o | Fever | GA positive (AFB smear) + NGI in LN biopsy | Possible DBD | Unidentified immunodeficiency |
| 3 | M | 5 m/o - 6.5 m/o | Fever, HSM, LAP (axillary) | BMA positive (AFB smear + NGI) | Possible DBD | SCID |
| 4 | F | 5 m/o - 5.5 m/o | HSM, LAP (axillary, portohepatis, mesenteric) | GA positive (AFB smear) | Possible DBD | Unidentified immunodeficiency |
| 5 | M | 13 m/o - 14 m/o | Fever, HSM, LAP (axillary) | BMA positive (AFB smear + NGI) | Possible DBD | WAS |
| 6 | F | 3 m/o - 5 m/o | HSM, LAP (axillary, para-aortic, portohepatis) | GA & BMA positive (culture & PCR) (BCG isolated) | Definitive DBD | IL-12Rβ1 deficiency |
| 7 | M | 1.5 m/o - 5 m/o | HSM, LAP (axillary, inguinal) | GA positive (PCR) (MTBC is isolated) | Probable DBD | IL-12Rβ1 deficiency |
| 8 | M | 2 m/o - 4 m/o | Fever, WL, cough, chronic diarrhea, LRTI, HSM, lobar consolidation on CXR | BMA positive (AFB smear) | Possible DBD | SCID |
| 9 | F | 4 m/o - 11 m/o | Fever, WL, LRTI, HSM, LAP (axillary, abdominal), ascites, miliary opacification on CXR | GA & BMA positive (culture & PCR) (BCG isolated) | Definitive DBD | IL-12Rβ1 deficiency |
| 10 | M | 5 y/o - 5 y/o | Fever, LAP (axillar, para-aortic, cervical, portohepatic) | GA positive (culture & PCR) (BCG isolated); colon biopsy positive (AFB smear + NGI) | Definitive DBD | IL-12Rβ1 deficiency |
| 11 | M | 18 m/o - 18 m/o | HSM, LAP (axillary, cervical, para-aortic) | GA & BMA positive (PCR) (BCG isolated) | Definitive DBD | Tyk2 deficiency |
| 12 | M | 4 m/o - 9 m/o | Fever, WL, HSM, LAP (axillary, cervical, submandibular), ascites, multiple hypoechoic lesions in spleen | GA positive (AFB smear) | Possible DBD | IL-12Rβ1 deficiency |
| 13 | M | 4 m/o - 4 m/o | Fever, HSM, LAP (axillary), jaundice, ascites, diffuse alveolar opacity on CXR | GA & BMA positive (PCR) (MTBC is isolated) | Possible DBD | IL-12Rβ1 deficiency |
| 14 | F | 3 m/o - 5 m/o | Fever, WL, HSM, LAP (axillary, para-aortic, mesenteric), ascites | GA & BMA positive (PCR) (MTBC is isolated) | Probable DBD | IL-12Rβ1 deficiency |
| 15 | F | 3 m/o - 7 m/o | Fever, HSM, LAP (axillary, cervical, para-aortic) | GA & BMA positive (culture & PCR) (BCG isolated) | Definitive DBD | IL-12Rβ1 deficiency |
| 16 | M | 3 m/o - 4 m/o | Fever, WL, HSM, multiple hypoechoic lesions in spleen | GA & BMA positive (PCR) (MTBC is isolated) | Probable DBD | SCID |
| 17 | M | 3 m/o - 4 m/o | Fever, HSM, LAP (axillary), multiple hypoechoic lesions in spleen | BMA positive (PCR) (MTBC is isolated) | Probable DBD | SCID |
| 18 | M | 4 m/o - 4 m/o | Fever, WL, cough, LRTI, HSM, LAP (axillary) , diffuse alveolar opacity on CXR | BMA positive (PCR) (MTBC is isolated) | Probable DBD | SCID |
| 19 | M | 3 m/o - 3 m/o | Fever, cough, LRTI, HSM, ascites, multiple hypoechoic lesions in liver, bronchopneumonia on CXR | GA positive (AFB smear) | Possible DBD | SCID |
| 20 | F | 2 m/o - 3.5 m/o | Fever, WL, HSM, LAP (axillary) | GA & BMA positive (PCR) (MTBC is isolated) | Probable DBD | IL-12Rβ1 deficiency |
| 21 | M | 2 m/o - 2 m/o | Fever, splenomegaly, LAP (axillary, cervical, inguinal) | GA & BMA positive (AFB smear) | Possible DBD | Unidentified immunodeficiency |
| 22 | M | 3 m/o - 3 m/o | Fever, WL, HSM, LAP (axillary, para-aortic) | GA positive (AFB) BMA positive (AFB smear + NGI) | Possible DBD | IL-12Rβ1 deficiency |
Abbreviations: AFB, acid-fast bacilli; ALRTI, acute lower respiratory tract infection (tachypnea or chest indrawing) (17); BMA, bone marrow aspiration; BCG, Bacille Calmette-Guérin; DBD, disseminated BCG disease; F, female; GA, gastric aspiration; HSM, hepatosplenomegaly; LAP, lymphadenopathy; M, male; m/o, months old; MTBC, M. tuberculosis complex; NGI, necrotizing granulomatous inflammation; PCR, polymerase chain reaction; WL, weight loss; SCID, severe combined immunodeficiency.
4.5. Patient Outcome
| Patients | Treatment (Duration) | Additional Sign & Symptom (Probably Unrelated to BCG Vaccination) | Outcome | |
|---|---|---|---|---|
| Initiation Phase | Continuation Phase | |||
| 1 | RHEClr | - | - | Died at that hospitalization (4 m/o) |
| 2 | RHEClr/IFN-γ | - | - | Died at 13 m/o |
| 3 | RHAzm | - | Diaper and oral candidiasis | Died at 9 m/o |
| 4 | RHAzm | - | Diaper and oral candidiasis | Unknown |
| 5 | RHEClr/IFN-γ (2 y) | HE IFN-γ (until death) | He developed acute rejection after receiving BMT at age of 6 m/o that recovered but had repeated episodes of recurrent infection | Died at 6 y/o after 2nd BMT |
| 6 | RHEClr/IFN-γ (4 m) | RH IFN-γ (8 m) | Oral candidiasis; palpable erythematous maculopapular skin lesions with arthritis (twice, improved spontaneously) | Alive 9.5 y/o |
| 7 | RHEClr/IFN-γ (4 m) | RH IFN-γ (8 m) | Oral candidiasis; palpable erythematous maculopapular skin lesions with arthritis improved with antibiotics at age of 8 y/o | Alive 8.5 y/o |
| 8 | RHEClr/IFN-γ | - | Oral candidiasis | Died at 6 m/o |
| 9 | RHEClr/IFN-γ (4 m) | RH IFN-γ (8 m) | Oral candidiasis | Alive 9.5 y/o |
| 10 | RHEClrAMK/IFN-γ (6 m) | RH IFN-γ (12 m) | Oral candidiasis | Alive 16 y/o |
| 11 | RHEClr/IFN-γ (3 m) | RH IFN-γ (9 m) | Oral candidiasis; allergic symptoms (rhinitis & Skin) | Alive 5.5 y/o |
| 12 | RHEClr/IFN-γ (2 m) | - | - | Died at 11 m/o |
| 13 | HEClrAMK/IFN-γ | - | - | Died at that hospitalization (4 m/o) |
| 14 | RHEClr/IFN-γ (4 m) | RH IFN-γ (9 m) | Oral candidiasis; repeated episodes of palpable erythematous maculopapular skin lesions with severe arthritis (leukocytoclastic vasculitis on skin biopsy with positive blood culture for salmonella at first presentation and improved with antibiotics), next episodes controlled with oral antibiotics | Alive 5.5 y/o |
| 15 | RHEClr/IFN-γ (3 m) | RH IFN-γ (9 m) | Oral candidiasis; repeated episodes of palpable erythematous maculopapular skin lesions with severe arthritis (leukocytoclastic vasculitis on skin biopsy with negative cultures of blood and stool for salmonella) that improved with antibiotics), next episodes controlled with oral antibiotics | Alive 8.5 y/o |
| 16 | RHEClr/IFN-γ (4 m) | RH (so far) | Disseminated candidiasis | Alive 3 y/o |
| 17 | RHEClr/IFN-γ | - | Diaper candidiasis; sepsis | Died at that hospitalization (4 m/o) |
| 18 | RHEClr | - | Diaper candidiasis; sepsis | Died at that hospitalization (4 m/o) |
| 19 | RHEAzm | - | Oral candidiasis, bilateral nephrocalcinosis | Died at that hospitalization (3 m/o) |
| 20 | RHEClr/IFN-γ (5 m) | RH-IFN-γ (9 m) | Oral candidiasis; bilateral nephrocalcinosis at infancy that improved with conservative treatments | Alive 8 y/o |
| 21 | RHEClr/IFN-γ (3 m) | RH-IFN-γ (9 m) | - | Alive 16 m/o |
| 22 | RHEAm (1 y) | R ± H (so far) | Oral candidiasis; cutaneous leishmaniasis at age 6 years old for 2 years duration resistant to that cured with interferon gamma; repeated episodes of recurrent bacterial infection; developed muscle weakness since 7 years old (positive genetic testing for Duchenne muscular dystrophy) | Alive 15 y/o, bedridden |
Abbreviations: Am, amikacin; Azm, azithromycin; BMT, bone marrow transplantation; Clr, clarithromycin; E, ethambutol; H, isoniazid; IFN-γ, interferon gamma; m/o, months old; R, rifampicin; SCID, severe combined immunodeficiency; WAS, Wiskott-Aldrich syndrome; y/o, years old.