1. Context
Staphylococcus aureus is one of the common causes of nosocomial and community-acquired infections. These bacteria commonly exist on the skin and in the nasal cavity of human (1), and may lead to a wide range of diseases including blood stream infection (BSI), wound and skin infections, endocarditis, chronic bone infections, surgical site infections, and devastating septicemia (2, 3).
In 1961, methicillin-resistant Staphylococcus aureus (MRSA) was reported for the first time in England (4). The emergence of MRSA made vancomycin as the first-line treatment for these strains (2, 3). Due to excessive use of vancomycin, decreased susceptibility and increased resistance to this antibiotic are reported in various parts of the world.
In 1997, the first vancomycin-intermediate Staphylococcus aureus (VISA) (Mu 50, MIC = 8 mg/L) and the hetero-VISA (hVISA) isolates (Mu 3, MIC = 2 mg/L) were reported in Japan, leading to the serious concern regarding the efficacy of vancomycin (3, 5). The first vancomycin-resistant S. aureus with minimum inhibitory concentration (MIC) of ≥ 32 mg/L was reported from U.S (Michigan) (6).
VRSA strains are a major health problem and the circulating increase of such strains is a global threat due to the lack of antibiotic choices.
According to the recent studies, at the end of 2012 33 VRSA strains were reported, including 13 strains from the USA, 16 from India, 1 from Pakistan, and 3 from Iran (7, 8).
The current traditional review aimed at reporting the total number of VRSA strains reported from the Middle-East, defined based on the clinical and laboratory standards institute (CLSI) guidelines, up to the end of 2016.
2. Methods
Related phrases and keywords including Staphylococcus aureus, S. aureus, vancomycin, vancomycin resistance, vancomycin-resistant S. aureus, and VRSA were used to search through Google, Google Scholar, PubMed, ScienceDirect, as well as a Persian scientific database of “Scientific Information Database” (www.sid.ir). Due to the high importance of VRSA strains, the original articles published in journals with high impact factor and indexed by PubMed or the other databases have overlapping data.
2.1. Data Exclusion Criteria
In 2006, the vancomycin cutoff points for S. aureus were reduced with CLSI from 4, 8 - 16, and 32 mg/mL to 2, 4 - 8, and 16 mg/mL referring to susceptible, intermediate, and resistant species, respectively (3, 9).
According to CLSI guidelines, the disc diffusion method is recommended to identify VRSA strains (CLSI, 2007).
In 2012, the CLSI defined the vancomycin MIC ≥ 16 mg/mL for VRSA, based on the broth microdilution method (CLSI, 2012).
Based on the above explanations, the results of all articles evaluating vancomycin MIC and performing polymerase chain reaction (PCR) for vanA (vancomycin resistance gene) were included in the current review.
Due to lack of laboratory facilities in the Middle-East, the broth microdilution method is rarely used; therefore, data from articles using other methods including broth macrodilution, agar dilution, and E-test were preliminary included. However, these methods are generally affected by plenty of factors including incubation conditions, quality of commercial discs and media, PH of the media, and also personnel’s proficiency.
Therefore, due to lower sensitivity of phenotypic findings, the detection of vanA gene in the isolates using PCR was considered the representative of VRSA strains.
In addition, due to changes of standards for the phenotypic evaluation over the time, interpretation of the results of phenotypic investigations might be confounding.
Accordingly, all articles were evaluated and the articles with definite standards for VRSA based on CLSI guidelines were selected, the data were gathered, classified, and finally summarized.
3. Results
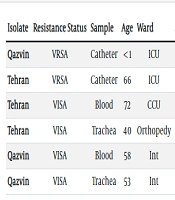
Approximately, 5500 related articles/abstracts were extracted in the initial searches from PubMed, of which 100 were conducted in the Middle-East. Next, reviewing all articles/abstracts revealed 26 initial reports for VRSA isolates in the Middle-East that were finally enrolled in the further analysis (Table 1).
Table 1.Data of VRSA Isolates Reported in the Middle-East
| Reference | Patients’ Age, y/Gender | Isolated From | Place of Isolation | Date of Isolation/Publication | MICa Value | vanA/B Detection Based on PCR Results |
|---|---|---|---|---|---|---|
| (10) | ND | Various clinical specimens | Tehran, Iran | 2005 | 128b,c | Unknown |
| (10) | ND | Various clinical specimens | Tehran, Iran | 2005 | > 256b,c | Unknown |
| (11) | ND | Various clinical specimens | Jordan | 2006 | 128b,c | Unknown |
| (11) | ND | Various clinical specimens | Jordan | 2006 | > 256b,c | Unknown |
| (12) | 67/M | Wound infected after cardiac surgery | Tehran, Iran | 2008 | 512d | vanA, (+) |
| (13) | ND | Various clinical specimens | Tehran, Iran | 2008 | 256c | Unknown |
| (14) | ND | (Children admitted to hospital) | Egypt | 2008 | 33/50d | vanA, (+) |
| (15) | Mean age 52.4 ± 20.7 /M and FM | Patients on hemodialysis | Sari, Iran | 2010 | > 8d | Unknown |
| (16) | 63/M | Pus | Pakistan | 2010 | 32b | mecA, (+) |
| (17) | ND /M and FM | ND | Khorramabad, Iran | 2011 | 16c | Unknown |
| (18) | 48 ± 15/ M and FM | Patients with underwent surgery | Algeria | 2011 | 16c | Unknown |
| (18) | 48 ± 15/ M and FM | Patients underwent surgery | Algeria | 2011 | 64c | Unknown |
| (18) | 48 ± 15/ M and FM | Patients underwent surgery | Algeria | 2011 | 128c | Unknown |
| (19) | ND | Blood | Pakistan | 2011 | 16 | vanA, (+) |
| (20) | 51/FM | Abscess | Tehran, Iran | 2012 | 512d | vanA, (+) |
| (21) | 26/M | Bronchial aspirate | Mashhad, Iran | 2012 | 512b | vanA, (+) |
| (22) | ND | Blood, pus, urine | Egypt | 2012 | 32e | vanA, (+) |
| (23) | ND | Children | Saudi Arabia | 2012 | > 8f | Unknown |
| (24) | 12-Month-old/M | Surgery wound | Tehran, Iran | 2013 | ND | vanA, (+) |
| (24) | ND | Children | Tehran, Iran | 2013 | ND | vanB, (+) |
| (24) | ND | Children | Tehran, Iran | 2013 | ND | vanA, vanB,(+) |
| (7) | 33/FM | Nasal cavity | Shiraz, Iran | 2013 | ND | vanA, (+) |
| (6) | ND | Skin swab | Egypt | 2014 | ≥ 16c | vanA, (+) |
| (25) | ND | ND | Saudi Arabia and Egypt | 2015 | NDf | Unknown |
| (26) | ND | Blood | Mashhad, Iran | 2015 | NDf | Unknown |
| (27) | 33/FM | Children | Tabriz, Iran | 2015 | NDf | Unknown |
| (28) | ND /M and FM | Surgical and septic wounds | Pakistan | 2015 | Differentd | Unknown |
| (29) | ND | ND | Egypt | 2015 | Differentc | vanA, (+) |
| (30) | ND | Various clinical specimens | Mashhad, Iran | 2015 | NDf | Unknown |
| (31) | ND | Various clinical specimens | Tehran, Iran | 2016 | > 16b | Unknown |
| (32) | ND / M and FM | Various clinical specimens | Kerman, Iran | 2016 | NDb,f | Unknown |
| (33) | ND | Adult nephrology ward | Shiraz, Iran | 2016 | NDf | Unknown |
Abbreviations: F, Female; M, Male; ND, Not Defined.
aMIC is expressed as mg/L.
bE-test.
cAgar dilution method.
dBroth microdilution method.
eBroth macrodilution method.
fDisk diffusion method.
From the first reported VRSA (2002) until 2012, four VRSA strains were from Iran, 7 from Egypt, and 1 from Pakistan. From 2012 to 2016, seven VRSA isolates were reported from the Middle East (1 from Iran and 6 from Egypt).
4. Discussion
The current report described the VRSA prevalence in the Middle-East from 2002 to 2016. The reported number of VRSA in the Middle-East seems to be more than the exact number of resistant strains. Failure to utilize the global guidelines and standards (CLSI) for laboratory procedures and lack of a definitive molecular approach to detect vancomycin-resistant species resulted in many indefinite reports. Such strains could not be considered as definite VRSA species from international perspectives. Although the VRSA global trend is increasing, some reports might be misleading.
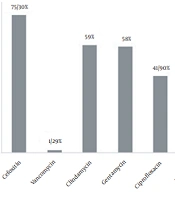
Most of the VRSA indicated in the recent reports had 2 common characteristics. 1, most of them were also MRSA and showed resistance to other antimicrobial agents; in other words, they were multidrug resistant (MDR) VRSAs (Table 2).
Table 2.Multidrug Resistant VRSA
| Reference | VRSA Number | Antibiotic Resistant Pattern |
|---|---|---|
| (12) | 1 | Vancomycin, teicoplanin, cefazolin, clindamycin, ceftriaxone, ceftizoxime, erythromycin |
| (14) | 2,3 | Vancomycin, linezolid, ciprofloxacin, erythromycin |
| (16) | 4 | Vancomycin, Penicillin, cefixime, doxycycline, aztreonam, nalidixic acid |
| (19) | 5 | Vancomycin, oxacillin/methicillin |
| (20) | 6 | Vancomycin, teicoplanin, penicillin, oxacillin, ceftriaxone, erythromycin, clindamycin, amikacin, co-trimoxazole, chloramphenicol, amoxicillin |
| (21) | 7 | Vancomycin, cefazolin, co-trimoxazole, linezolid |
| (27) | 8 | Vancomycin ,oxacillin, levofloxacin, ciprofloxacin, tetracycline, co-trimoxazole, clindamycin, rifampin |
| (22) | 9 - 13 | Vancomycin, clavulanic acid, cefoxitin, cefazolin, oxacillin, tetracycline, cefixime |
| (24) | 14 | Vancomycin, oxacillin, cefoxitin |
| (6) | 15 | Vancomycin, penicillin, amoxicillin\clavulanic acid, ampicillin\sulbactam |
| (29) | 16 - 20 | Vancomycin |
2, the genetic mechanism and background of vancomycin resistance in VRSA strains were not clearly defined in the papers.
Several genes were involved in resistance mechanism of VRSA strains (8, 34). Co-transfer of vancomycin resistance and other resistance genes from Enterococcus faecalis to Staphylococcus aureus were previously demonstrated (35). Namely, patients with VRSA infection might be simultaneously coinfected with VRE (vancomycin-resistant Enterococci). In such cases, resistance gene can be transferred from Enterococcus spp. to S. aureus. MRSA strains are more susceptible to receive the vanA resistance gene (3). Some MRSA strains receive resistance gene (Tn1546) from glycopeptide-resistant enterococci (8). This finding can explain the multidrug resistance mechanism of VRSA strains. Most of the included articles lacked complete information and did not fulfill the CLSI criteria on VRSA identification. Accordingly, the articles 6, 7, 12, 14, 19, 20, 21, 22, 24 and 30 were defined as creditable articles based on CLSI criteria in this region.
The first report of glycopeptide resistance among clinical isolates of Gram‑positive bacteria (enterococci) (36) caused a great concern for the emergence of new VRSA strains due to receiving vanA gene from enterococci.
In 2002, the first completely sequenced VRSA strain was identified in the United States. The detected strain drew great attention of medical community to a new therapeutic problem in the medical settings (37).
Before the first report of VRSA strain, vancomycin was increasingly used to treat MRSA strains, MDR S. aureus, and some other infections such as nosocomial ones and those caused by coagulase-negative staphylococci (CoNS) (38, 39).
Bacterial resistance to vancomycin may result from inadequate antimicrobial treatment of MRSA strains that in turn caused the emergence of VRSA strains over time and ultimately result in increased morbidity and mortality (38).
Multidrug resistant bacteria are a major challenge for medical society to manage the infectious diseases, which may even raise community concern. In addition, this problem can be a considerable burden on healthcare sectors (40).
According to many studies, the factors such as inadequately treated MRSA infection or colonization with VRE strains, and exposure to vancomycin, careless prescription of antibiotics, availability of antibiotics at the drugstores without prescription, lack of monitoring over nursing practices, extensive surgical procedures, prolonged hospitalization, serious underlying disease such as diabetes, malignancy, and renal failure are cited as the main risk factors for the emergence of VRSA (2, 6, 40).
Most articles lacked the main clinical and laboratory information; therefore, the current review did not describe the clinical characteristics of the patients infected with vanA-harboring VRSA isolates.
Only 2 articles reported the isolation of VRSA from 2 patients with diabetes underwent dialysis due to renal complications (12, 20). Patients with diabetes, especially with major complications, are predisposed to VRSA infections due to suppressed immune system and prolonged exposure to sub therapeutic levels of antibiotics including vancomycin.
The development of antimicrobial resistance in the Middle-East seems to be related to the selective pressure of vancomycin, the main antibiotic available to treat MRSA infections in the region, or due to the irrational application of antibiotics (6, 12, 14, 16).
As mentioned before, extensive surgical procedures and prolonged hospitalization for some reasons such as indiscriminate use of antibiotics in hospitals or the presence of other organisms harboring resistance genes such as vre are the main factors for the emergence of VRSA. These risk factors were also noted in the Middle-East reports (6, 20, 22).
Healthcare workers and healthy individuals may carry resistant strains of S. aurous in their nasal cavity. Such resistant bacteria may spread by contact and cause community-acquired infections (20).
To summarize, the emergence and spread of VRSA strains is one of the most important clinical issues in hospitalized patients. The current traditional review investigated and highlighted the increasing risk of VRSA strains in clinical settings in the Middle-East. The lack of standardized criteria to define VRSA is the main problem to evaluate and interpret the literature in this area. However, great attention should be paid to the risk of increasing VRSA. There are some important and serious factors that can affect the increase of VRSA strains. Thus, some strategies such as infection-control practices, appropriate antibiotic prescription, environmental hygiene, and improved knowledge may help to control the spread of antimicrobial-resistant microorganisms, including VRSA. A preliminary abstract of this work has been presented in 15th International & Iranian Congress of Microbiology.