Hepatitis B virus infection is still an important public health issue in the world (
2,
27). Since chronic HBV patients with liver fibrosis account for a significant proportion of HCC cases, previous studies have confirmed that liver cirrhosis (F4 stage) is associated with the increased risk of developing HCC, unlike other liver fibrosis stages (
11,
28-
30). While the existing literature has mostly focused on the adverse effects and costs of current antiviral therapies, little is known about the degree of liver fibrosis to make more informed treatment decisions. Therefore, the precise evaluation of liver fibrosis seems essential to identify susceptible cases to severe diseases and make appropriate therapeutic decisions for CHB-infected patients (
31).
Liver biopsy is still the reference standard for the diagnosis of cirrhosis and staging of liver fibrosis in CHB patients; however, it has certain limitations as an invasive test with some serious health risks (
8). Therefore, extensive studies have considered evaluating non-invasive techniques regarding liver fibrosis, including blood biomarkers, such as APRI and FIB-4, and imaging techniques, such as TE via ultrasound, optical digital analysis of CT images, and magnetic resonance (MR)-based techniques (
32). On the other hand, the limitations of non-invasive techniques include body mass index, steatosis, sampling variability, high cost, low sensitivity or specificity, and lack of standardized cutoff points for the assessment of fibrosis stage, as mentioned in previous studies. To overcome the limitations of these methods, we developed a diagnostic algorithm for the prediction of liver fibrosis, using HBI-based HAPS with Tc-99m MDP as a potential alternative.
In this study, a comparison was made between the diagnostic value of HBI and other non-invasive methods, such as APRI, FIB-4, and LSM, in the assessment of liver fibrosis in 87 CHB patients. We established a new algorithm to assess liver fibrosis, which was more effective than other ones. Spearman’s rank correlation coefficient and Eta value of HBI versus the degree of liver fibrosis, according to the METAVIR scoring system, were 0.672 and 0.763 (P < 0.001), respectively, which confirmed HBI changes associated with fibrosis stage. There is an association between the degree of liver fibrosis and portal pressure, evidenced by comparing histological alterations in liver biopsy and HAPS (
9,
33). In physiological conditions, the portal vein and hepatic artery provide two-thirds and one-third of the blood flow for the liver, respectively. Nonetheless, in liver fibrosis and cirrhosis, the liver counterbalances this event through an increase in the hepatic arterial blood flow for maintaining the same total perfusion. Increased hepatic arterial blood flow is correlated with elevated elastometry in cirrhotic cases in response to meal ingestion (
17,
32-
34), which can explain a remarkable increase in HBI with liver fibrosis and a moderate reduction in total perfusion with fibrosis grades.
The performance of non-invasive diagnostic methods can be evaluated by the calculation of AUROC, with liver biopsy as the reference standard. The AUROC has been measured in all selected studies, and the standard error can be calculated or estimated based on the existing information, particularly at a 95% confidence interval (CI). The random-effects model indicated the dissimilarity of the studies to analyze the overall efficacy of non-invasive tests for liver fibrosis in different studies (
11,
35).
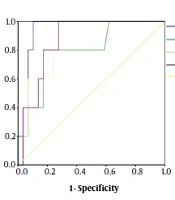
In the present study, HBI showed better performance in differentiating liver fibrosis stages, with AUROC of 0.848 (95% CI: 0.748 - 0.948) for fibrosis stage ≥ F1, 0.884 (95% CI: 0.806 - 0.961) for fibrosis stage ≥ F2, 0.924 (95% CI: 0.856 - 0.993) for fibrosis stage ≥ F3, and 0.938 (95% CI: 0.880 - 0.995) for fibrosis stage F4. With significant fibrosis defined as ≥ F2, the AUROC of HBI (0.884; 95% CI: 0.806 - 0.961; P = 0.000) was greater than that of LSM (0.807; 95% CI: 0.703 - 0.912; P = 0.000), APRI (0.684; 95% CI: 0.556 - 0.812; P = 0.009), and FIB-4 (0.757; 95% CI: 0.641 - 0.873; P = 0.000) regarding the diagnostic performance of liver fibrosis. Overall, the AUROC values of 100%, over 90%, and more than 80% indicate the perfect, excellent, and good diagnostic tool, respectively (
11). Accordingly, HBI is an excellent tool to confirm liver fibrosis when other clinical signs and evaluations are non-decisive.
Non-invasive methods of liver fibrosis can be divided into two categories: The physical approach based on LSM and the biological approach according to the quantification of biomarkers in blood specimens, involved in the molecular pathogenesis of fibrosis (e.g., APRI and FIB-4). The physical approach is related to a genuine and intrinsic physical feature of liver parenchyma, while the biological approach indicates different, not strictly liver-specific clinical and serum factors, correlated with fibrosis grade (
35,
36). However, these two categories are limited by the inherent characteristics of liver fibrosis. In clinical practice, TE is not accurate (specificity < 60%) to identify cases with esophageal varices and non-alcoholic fatty liver disease. Furthermore, a recent report suggested that the performance of blood biomarkers, including APRI and FIB-4, to identify and exclude advanced fibrosis may be different during life, as young adults are found with lower accuracy and older adults with a lower specificity.
According to direct comparisons based on the AUROC in CHB patients (
Figure 3), HBI performed substantially better than APRI and FIB-4 in the diagnosis of fibrosis and cirrhosis and moderately better than LSM to diagnose fibrosis. Differences between HBI and other blood tests or LSM were relatively small, particularly in the significant fibrosis stage. Based on these results, by using optimal cutoff points as standards, the sensitivity and specificity of HBI were found to be similar in predicting similar stages of fibrosis, whereas those of LSM, APRI, and FIB-4 were slightly irregular to predict similar stages of fibrosis; thus, HBI was significantly associated with the degree of liver fibrosis CHB patients.
Some limitations of this study should be acknowledged. First, this retrospective study was validated in a relatively small sample size of CHB patients. Second, using liver biopsy as a reference standard to evaluate liver stages has methodological flaws, which may influence the performance of the conducted tests. Third, other clinical confounding factors, such as splenomegaly and esophageal varices, may affect liver fibrosis, and these factors need to be considered in future studies.
5.1. Conclusion
We applied the HAPS method, followed by AUROC measurement, to evaluate the association of HBI with the degree of liver fibrosis in CHB patients. The results suggested the potential application of HBI as an accurate and inexpensive alternative for the diagnosis of liver fibrosis stage and guiding therapy in CHB patients. The current study was the first to report using HBI for the detection of liver fibrosis stage in CHB patients. This study not only confirmed earlier findings, showing that scintigraphic evaluation of hepatic blood flow is possible through determining HBI (ratio of hepatic artery flow to total hepatic flow), but also provided new information about a novel, reliable, and non-invasive technique to assess liver fibrosis to facilitate further in-depth clinical applications. The proposed method also is possibly a promising nuclear medicine method to predict liver fibrosis in CHB patients regarding preliminary results.







, LSM (B), APRI (C), and FIB-4 (D) according to liver fibrosis stage in the 87 patients’ cohort.")
 ROC curve for liver fibrosis ≥ F1 stage. (B) ROC curve for significant liver fibrosis (≥ F2). (C) ROC curve for advanced liver fibrosis (≥ F3). (D) ROC curve for liver cirrhosis (F4). AUROC: area under the receiver's operating characteristic curve; 95% CI: 95% confidence interval.")


