1. Background
A variety of paraneoplastic syndromes, the majority of neurological complications, are occurring in timely association with neuroblastoma. Opsoclonus-myoclonus syndrome (OMS), and cerebellar ataxia are the most common paraneoplastic syndromes considered to be paraneoplastic neurologic disorders (PNDs) (1). Kerner-Morrison syndrome is another typical paraneoplastic syndrome. However, clinical presentations of paraneoplastic syndromes may be multiple. Early diagnosis of these syndromes maximizes likelihood of the treatment of the tumor along with the absence of the neurologic manifestations. Within the last 5 years, 68 children were diagnosed with neuroblastoma in our institution. 9 of them presented exclusively with paraneoplastic syndromes involving various organs or systems, some of which were recognized as rare paraneoplastic syndromes. Initially, these patients were misdiagnosed with other diseases and they were treated inappropriately.
2. Objectives
In order to make more accurate diagnosis, we reviewed the clinical data and the literature on this syndrome.
3. Patients and Methods
Between April 2007 and April 2012, 68 children were diagnosed with neuroblastoma or ganglioneuroblastoma in our institution, 9 of which presented exclusively with paraneoplastic syndromes and had not received chemotherapy before diagnosis. After collecting the patients’ clinical records and having reviewed the literature on pediatric neuroblastoma cases that coincided with paraneoplastic syndrome, further understanding of the phenomena was reached. Following diagnosis, all patients received chemotherapy and operation on NB97 protocol.
4. Results
At the time of diagnosis, among 68 pediatric patients with neuroblastoma or ganglioneuroblastoma, 4 (5.9%) patients suffered from neurological complications at diagnosis, 2 (2.9%) patients had digestive tract disorders, 2 (2.9%) patients had immune diseases, and 1 (1.5%) suffered hematological disorder (without bone marrow involvement). Neurological complications were the most common ones, which were followed by digestive and immune diseases. Six patients experienced misdiagnosis and received treatments including gammaglobulin and/or prednisone/dexamethasone. After chemotherapy and operation, 5 patients achieved complete remission and all 4 patients with PNDs achieved partial response after a median time of 4 months on paraneoplastic syndrome. All patients achieved complete remission of paraneoplastic syndrome before completion of chemotherapy. Among the 9 patients, one (11.1%) patient died during treatment. Eight (89.9%) patients continued living for 24 to 39 months. The median follow up duration for these patients was 2.08 ± 0.929 (95% CI, 1.95-3.12) years. The two years event free survival was 77.8%, the two years overall survival was 88.9%. The characteristics of the 9 patients are shown in Table 1.
Table 1.Characteristics of 9 Neuroblastoma Patients With Paraneoplstic Syndromes a
| No | Age, y | Gender | Presentations | Initial Diagnosis | Initial Treatment | Time, m | Anti-Hu | Pathology Type and Clinic Classifications (INSS) | Primary Tumor Site | Treatment | Follow-up, y | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| G | P/D | |||||||||||
| 1.6 | M | myalgia | polyneuropathy | + | + | 8 | - | neuroblastoma II | adrenal glands | Chemo | 2.5 | |
| 3 | M | motor dysfunction of both lower extremities | Guillain-Barre snydrome | + | + | 2 | - | neuroblastoma III | thoracic vertebra | Chemo + radio | (0.8) relapse | |
| 5.2 | F | cerebellar ataxia | cerebellitis | + | + | 6 | + | neuroblastoma IV | adrenal glands | Chemo + radio | 3 | |
| 1.7 | M | monoplegia of the lower extremity | neurologic damage | + | + | 8 | + | neuroblastoma IV | adrenal glands | Chemo + radio | 2.5 | |
| 5.6 | M | constipation | not clear | - | - | 2 | + | ganglioneuroblastoma IV | adrenal glands | Chemo + radio | 2.1 | |
| 1.5 | F | diarrhea | Chronic diarrhea | - | - | 3 | + | ganglioneuroblastoma IV | adrenal glands | Chemo + radio | 3.3 | |
| 8.5 | F | erythema of both lower extremities | anaphylactoid purpura | - | + | 0.5 | - | ganglioneuroblastoma III | adrenal glands | Chemo | 2 | |
| 1.9 | M | Kawasaki disease | Kawasaki disease | + | - | 2 | - | neuroblastoma III | adrenal glands | Chemo + radio | 2 | |
| 2.3 | M | thrombocytopenic purpura | thrombocytolytc purpura | + | + | 2 | - | neuroblastoma III | adrenal glands | Chemo + radio | (0.5) dead | |
a Abbreviations: Chemo, chemotherapy; F, female; G, gammaglobulin; INSS, international neuroblastoma staging system; M, male; P/D, prednisone/dexamethasone; Radio, radiotherapy; Time, time from onset of paraneoplstic syndrome to diagnosis of neuroblastoma.
5. Discussion
Paraneoplastic syndrome is defined as a dysfunction of organ systems caused by the remote humoral effects of a tumor and not by local effects or metastases (2). Neurological disorders are known as the most common paraneoplastic syndromes in patients with neuroblastoma. The highest frequency is opsoclpnus-myoclonus syndrome (OMS) (3). OMS has been observed in up to 4% of patients with neuroblastoma (1). Until now, various clinical cohort studies have shown different rates of neurological paraneoplastic syndromes. One such study claims that it could reach up to 40% (3), while it was reported 68% by Chu et al. (4). In our study, the rate of neurological complications was 5.9%. Apart from OMS, pediatric patients with neuroblastoma have presented with other paraneoplastic neurologic disorders, which include Lambert-Eaton myasthenic syndrome (5), encephalomyelitis (6), cerebellar ataxia (7), and hypothalamic syndrome (1). Among the 9 patients who presented with paraneoplastic syndromes in our study, 4 (5.9%) had neurological complications, the typical paraneoplastic syndrome was cerebellar ataxia, besides that, myalgia, motor dysfunction of lower extremities and monoplegia of the lower extremity were also seen. Why are paraneoplastic syndromes coinciding with neuroblastoma directly affecting the neurologic system? A variety of autoantibodies have been reported, particularly anti-Hu antibody, in neuroblastoma patients with paraneoplastic syndromes. Histochemically, it has been identified that the anti-Hu antibody reacts with nuclei of neurons throughout the central nervous system (8). OMS was first recognized as a possible remote effect of neuroblastoma by Solomon and Chutorian in 1968 (9). Since then, other neurological signs and syndromes, such as seizures, choreoathetosis, and peripheral neuropathies, have also been described as remote effects of neuroblastoma (10, 11).
In our cases, the presence of serum and cerebrospinal fluid (CSF) anti-Hu antibody was associated with complications including cerebellar ataxia, monoplegia of the lower extremity, constipation, and diarrhea. Even though, the initial presentation, in patient 2 was motor dysfunction of lower extremities. The spinal magnetic resonance imaging removed the possibility of spinal nerves compression by tumor mass. Based on Fathallah opinion, PNDs are subdivided into three categories: 1) those whose pathogenesis is understood, 2) those that are linked to the tumor by biologic data but whose pathogenesis is not yet elucidated, and 3) those that could not be linked to the malignancy by biologic data (12). Depending on specific damage of anti-Hu antibody to neural system and characteristics of sympathetic innervation, the presenting features of neuroblastoma may be various.
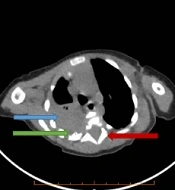
Honnorat et al. has reported a child with neuroblastoma who had localized myoclonus, progressive hemiplegia and high titers of anti-Hu antibodies in the serum and cerebrospinal fluid (13), indicating that due to the widespread presence of the sympathetic nervous tissue in various body organs and apparatuses, the presenting features of neuroblastoma may be variable. We believe that these complications in our patients are paraneoplastic syndromes. Diarrhea is another well-known symptom of paraneoplastic syndrome of neuroblastoma. There is evidence that this symptom is related to vasoactive intestinal polypeptide (VIP) production in tumor cells stimulating intestinal aberrant secretions (2). This phenomenon is known as a classic endocrine tumor effect. However, constipation in association with a ganglioneurobalstoma is rare. In our study, patient 5 presented with chronic constipation which had lasted for about 6 months. In general investigation, the abdominal image revealed a tumor in his left adrenal gland. Ganglioneuroblastoma was confirmed by fine-needle biopsy. Wildhaber et al. firstly described a patient presenting with intestinal pseudoobstruction as a paraneoplastic syndrome of ganglioneurobalstoma (14). Thus, in clinical experiences, although rare, diarrhea and constipation may initially present together in cases of neuroblastoma or ganglioneuroblastoma, easily missing the diagnosis of tumor. Interestingly, we observed that patients with ganglioneuroblastoma were mostly presenting with digestive system diseases. The relationship between tumor pathology and this paraneoplastic syndrome needs further study.
Manifestations of the remaining three patients in our study were rather unusual. To our knowledge, there was no report of paraneoplastic syndrome presenting with erythema, Kawasaki disease and immune thrombocytopenic purpura, associated with immune disorders. Even though immune injury is known as the major etiology for paraneoplastic syndromes, there are no established procedures to identify it in patients with neuroblastoma prior to tumor diagnosis. These manifestations may represent new kinds of paraneoplastic syndromes. Paraneoplastic syndromes will relieve after receiving immune therapy or chemotherapy, or be cured following surgical and/or chemotherapy interventions. Currently, the exact mechanisms of immune-mediated dysfunction and endocrine tumor effect with paraneoplastic syndromes in patients are unknown. It is postulated that autoimmune disorders are the major reason, but the precise pathophyiology is unclear.
Neuroblastoma may present with a range of nonspecific neurologic symptoms in addition to the well-known OMS and cerebellar ataxia. In our series, we identified 9 out of 68 patients different kinds of paraneoplastic syndromes prior to the diagnosis of neuroblastoma. All 9 patients had an episode of misdiagnosis. To date, however, there is no identifiable common denominator among the various paraneoplastic syndromes of neuroblastoma. But in any case, the presence of unexplained neurologic manifestations and other common clinical presentations such as erythema, constipation, diarrhea, especially immune disorders in an otherwise healthy child should raise the suspicion of a possible paraneoplastic syndrome because of the presence of an undiagnosed tumor.