1. Background
Healthcare-associated bloodstream infections (HCA-BSI) rated in neonatal intensive care units (NICUs) between 1.8% and 74.3% in several reports are a major cause of morbidity and mortality in NICUs and affect the cost of medical care by increasing resource consumption and duration of hospitalization (1-3). The most common type of neonatal healthcare-associated infection (HC-AI) is bloodstream infection (BSI). A neonate may be at risk of infection through one or many intrinsic and extrinsic factors, such as gestational age and presence of a single or multiple invasive devices (4). In developed and developing countries, most nosocomial infections (NIs) in NICUs are related to a longer duration of hospitalization, low birth weight and gestational age, respiratory diseases, invasive interventions, and medical treatments (5). HCA-BSIs, device-associated HC-AI in particular, are generally common in newborns because of their insufficient immune system and mechanical barriers as well as the lack of protective flora (6). Therefore, among hospitalized patients, neonates belong to those at the highest risk of HCA-BSIs. In addition, neonatal HCA-BSIs not only have high mortality but also increased risk of subsequent adverse outcomes, including white matter injury to the preterm brain and attendant neurodisability (7).
2. Objectives
The purpose of the present study was to identify the risk factors associated with the development of HCA-BSIs and the most frequent causative agents of the same in NICUs. Knowledge of the modifiable risk factors for HCA-BSIs would enable developing countries to implement interventions, thereby decreasing HCA-BSIs and the associated complications.
3. Methods
This retrospective study was conducted in the clinic of neonatology in Dicle university between January 2011 and December 2014. The neonatal unit has 34 incubators, 20 mechanical ventilators, and 2 open intensive care cods. This study included 126 patients (infected group) with positive blood cultures and 126 randomly selected patients (uninfected control group) with negative blood cultures after four days of hospitalization. Infection control doctors and nurses conducted hospital infection surveillance actively and prospectively. During the period of hospitalization, the infection control committees recorded patient information every day using the patients’ follow-up forms. The diagnosis of HCA-BSIs was made according to the criteria of the US center for disease control and prevention (10).
Healthcare-associated bloodstream infection (HCA-BSI): Patients with no sepsis on admission and who had microorganisms isolated from blood cultures taken 48 - 72 hours after birth on suspicion of sepsis according to the clinical signs and/or laboratory findings were diagnosed as HCA-BSI. Clinical findings, including apnea, bradycardia, hypothermia, hyperthermia, circulatory disorder, lethargy, hypotonia, and feeding difficulty, and laboratory findings, including leukocytosis, leucopenia, thrombocytopenia, a ratio of immature/mature neutrophils > 0.25, and a C-reactive protein value of > 0,05 mg/dL, were considered significant. Patients with signs of sepsis and showed no growth in culture and patients with duration of hospitalization of less than 48 - 72 hours were excluded from the study.
Strains of Staphylococcus epidermidis were considered involved in the infection if they represented the only microorganisms isolated from the blood specimen in the presence of clinical signs or symptoms of infection. Most authorities recommend obtaining two independent cultures to fulfill two workups of an episode of suspected bloodstream infection (11).
The blood samples taken from patients with suspected bacteremia and/or sepsis were inoculated into blood culture bottles and incubated in BACTEC 9120 and 9240 (Becton Dickinson, MD, USA) blood culture systems for 7 - 10 days at 37°C. The blood samples in which bacterial growth was detected were inoculated into 5% sheep blood agar, EMB agar, and chocolate agar media. These media were incubated at 35 ± 2°C for 20 - 24 hours. Wound swabs and other clinical specimens were directly inoculated into 5% sheep blood agar, EMB agar, and chocolate agar and incubated at 35 ± 2°C for 20 - 24 hours. All the strains isolated from the clinical specimens were identified using conventional methods and BD Phoenix™ 100 (Becton Dickinson, MD, USA).
Data were obtained from the database of the hospital infection control committee and patients’ medical records. Gender, gestational age, birth weight, birth presentation, type of delivery, length of hospitalization, results of blood cultures, surgical operation, ventriculoperitoneal shunt, tracheostomy procedure, diagnosis with intracranial hemorrhage, phototherapy, tracheostomy procedure, exchange transfusion, (four days of mechanical ventilation and neonatologist’s prediction of prolonged ventilation were the common indication), Apgar score point (fifth minute), use of umbilical catheter, nasogastric or orogastric tube, urinary catheter, mechanical ventilation, use of surfactant, erythrocyte transfusion, plasma transfusion, thrombocyte transfusion, intravenous immunoglobulin, and total parenteral nutrition infusion were recorded prospectively.
The cases not appropriate for hospital acquired infections (HAIs) because of clinical and laboratory findings and those who had a single blood culture with isolated central nervous system considered as contamination were excluded from the study.
The study protocol was approved by the Dicle university faculty of medicine ethic committee.
3.1. Statistical Analysis
The two-sided statistical tests were performed using SPSS for Windows (version 18.0; SPSS, Inc., Chicago, IL). A P value of < 0.05 was considered statistically significant. For the comparative analysis between groups (case vs. control), the χ2 test was used for categorical variables, and either the student t test or the Mann-Whitney test was used for the continuous variables. In the univariate analysis, differences were considered significant at P < 0.05. For the identification of independent factors of NI that could influence disposition, multivariable logistic regression analyses (polytomous responses) were performed to calculate the odds ratio and the corresponding 95% confidence intervals.
4. Results
A total of 126 positive blood cultures that were proven HCA-BSI attacks were found in 268 cases of suspected HCA-BSI. The study included 126 neonates (47.6% females and 52.4% males) with positive blood cultures and 126 neonates (44.4% females and 55.6% males) with negative blood cultures. Incidence of low gestational age, low birth weight, vaginal birth type, and length of hospitalization were higher in the infected neonates than in the uninfected neonates (Table 1).
Table 1.Demographic Features of the Infected and Uninfected Groups
| Infected Group, No. (%) | Uninfected Group, No. (%) | P Value | |
|---|---|---|---|
| Gender | 0.352 | ||
| Female | 60 (47.6) | 56 (44.4) | |
| Male | 66 (52.4) | 70 (55.6) | |
| Gestational age, wk | < 0.001 | ||
| ≤ 32 | 48 (38.1) | 26 (20.7) | |
| 33 - 37 | 22 (17.5) | 54 (42.9) | |
| ≥ 38 | 56 (44.4) | 46 (36.4) | |
| Birth weight, g | < 0.001 | ||
| < 1000 | 24 (19) | 0 (0) | |
| 1001 - 1500 | 17 (13.5) | 18 (14.3) | |
| 15001 - 2000 | 16 (12.7) | 38 (30.2) | |
| 2001 - 2500 | 12 (9.5) | 22 (17.5) | |
| > 2500 | 57 (45.2) | 48 (38.1) | |
| Delivery presentation | 0.184 | ||
| Head Presentation | 121 (96) | 124 (98.4 | |
| Breech Presentation | 5 (4) | 2 (1.6) | |
| Type of delivery | 0.005 | ||
| Vaginal birth type | 33 (26.2) | 16 (12.7) | |
| Caesarean section | 93 (73.8) | 110 (87.3) | |
| Length of hospitalization, d | < 0.001 | ||
| ≤ 15 | 20 (15.9) | 79 (62.7) | |
| 16 - 30 | 28 (22.2) | 37 (29.4) | |
| 31 - 60 | 52 (41.3) | 6 (4.8) | |
| ≥ 61 | 26 (20.6) | 4 (3.2) |
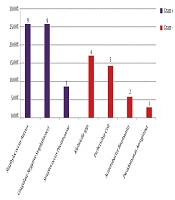
A total of 135 pathogens were isolated from 126 blood cultures. The most common organisms isolated from blood culture were S. epidermidis (20.7%), Klebsiella spp. (26.7%), and Acinetobacter spp. (13.3%) (Table 2).
Table 2.Distribution of Nosocomial Pathogensa
| Microorganism | No. (%) |
|---|---|
| Gram-Positive Organisms | |
| Staphylococcus epidermidis | 28 (20.7) |
| Staphylococcus hominis | 5 (3.7) |
| Staphylococcus haemolyticus | 5 (3.7) |
| Staphylococcus aureus | 3 (2.2) |
| Other coagulase-negative staphylococci | 8 (5.9) |
| Enterococcus spp. | 3 (2.2) |
| Other gram-positive organisms | 11 (8.1) |
| Gram-negative organisms | |
| Klebsiella spp. | 36 (26.7) |
| Acinetobacter spp. | 18 (13.3) |
| Pseudomonas aeruginosa | 7 (5.2) |
| Other gram-negative organisms | 2 (1.5) |
| Candida | 9 (6.7) |
| Total number of isolates | 135 (100) |
aNo. = 135 isolates in 126 neonates.
The results of the univariate analysis of the risk factors for HAIs in neonates are shown in Table 3.
Table 3.Comparison of Risk Factors Between the Infected and Uninfected Groupsa
| Risk Factors | Infected group | Uninfected group | P Valueb |
|---|---|---|---|
| Surgical operation | 46 (36.5) | 2 (1.6) | < 0.001 |
| Ventriculoperitoneal shunt | 21 (16.7) | 2 (1.6) | < 0.001 |
| Umbilical catheter | 49 (38.9) | 20 (15.9) | < 0.001 |
| Nasogastri or orogastric tube | 122 (96.8) | 113 (89.7) | 0.021 |
| Tracheostomy | 3 (2.4) | 0 (0) | 0.124 |
| Urinary catheter | 5 (4) | 0 (0) | 0.030 |
| Mechanical ventilation | 97 (77) | 32 (25.4) | < 0.001 |
| Use of surfactant | 40 (31.7) | 20 (15.9) | 0.002 |
| Phototherapy | 11 (8.7) | 10 (7.9) | 0.500 |
| Exchange transfusion | 3 (2.4) | 4 (3.2) | 0.491 |
| Erythrocyte transfusion | 102 (81) | 19 (15.1) | < 0.001 |
| Plasma transfusion | 49 (38.9) | 9 (7.1) | < 0.001 |
| Thrombocyte transfusion | 24 (19) | 2 (1.6) | < 0.001 |
| Intravenous immunoglobulin | 1 (0.8) | 3 (2.4) | 0.311 |
| Total parenteral nutrition infusion | 105 (83.3) | 44 (34.9) | < 0.001 |
| Intracranial hemorrhage | 15 (11.9) | 4 (3.2) | 0.008 |
| Length of hospitalization, d, mean ± SD | 43.9 ± 28.9 | 16.9 ± 14.3 | < 0.001 |
| Apgar score (5th minute), mean ± SD | 6.7 ± 1.5 | 7.9 ± 1.3 | < 0.001 |
| Total parenteral nutrition, d, mean ± SD | 18.5 ± 18.5 | 2.7 ± 5.8 | < 0.001 |
aValues are expressed as No. (%) unless otherwise indicated.
bχ2 and t distribution.
We selected 10 variables with a P value < 0.05 for the logistic regression model. In the multiple logistic regression analysis, fifth-minute Apgar score, use of erythrocyte transfusion, and surgical operation were found to be the independent risk factors for NIs in patients with a diagnosis of hospital infection (Table 4).
Table 4.Multivariate Logistic Regression Analysis of the Prediction of Independent Risk Factors for Nosocomial Infections
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| OR (95% CI) | P Value | OR (95% CI) | P Value | |
| Apgar score, 5th minute | 1.16 (0.79 - 1.53) | < 0.001 | 1.42 (1.03 - 1.96) | 0.030 |
| Mechanical ventilation | 0.10 (0.05 - 0.18) | < 0.001 | 0.42 (0.14 - 1.24) | 0.119 |
| Erythrocyte transfusion | 0.04 (0.02 - 0.08) | < 0.001 | 0.07 (0.31 - 0.19) | < 0.001 |
| Plasma transfusion | 0.12 (0.05 - 0.26) | < 0.001 | 1.50 (0.47 - 4.71) | 0.487 |
| Thrombocyte transfusion | 0.06 (0.01 - 0.29) | < 0.001 | 0.17 (0.02 - 1.00) | 0.050 |
| Use of surfactant | 0.40 (0.22 - 0.74) | 0.003 | 2.84 (0.66 - 12.0) | 0.157 |
| Ventriculoperitoneal shunt | 0.08 (0.18 - 0.35) | < 0.001 | 4.79 (0.50 - 45.7) | 0.173 |
| Umbilical catheter | 0.29 (0.16 - 0.53) | < 0.001 | 0.40 (0.11 - 1.47) | 0.173 |
| Surgical operation | 0.02 (0.00 - 0.11) | < 0.001 | 0.01 (0.02 - 0.07) | < 0.001 |
| Nasogastric or orogastric tube | 0.28 (0.09 - 0.90) | 0.024 | 1.31 (0.22 - 7.72) | 0.760 |
5. Discussion
The development of new treatment options and life support techniques in neonatology over the last few decades has increased the survival rate of neonates with low birth weight and preterm infants. However, NIs have become a major problem in the NICUs because of the prolonged length of hospitalization (12-14). The hospitalization of infants in NICUs has been reported in the literature as being longer, and the susceptibility to infection has been greater than in other pediatric intensive care units (15, 16). Unsurprisingly, we found that low gestational age and lower birth weight placed infants at a higher risk of developing bacterial BSIs. As indicated in other studies, this finding could be due to the patients’ immature immune system, long duration of hospitalization, and use of invasive procedures (17-19).
The variety of pathogens most commonly isolated from BSIs may vary from clinic to clinic or region to region (20, 21). Generally, gram-positive organisms are more common than gram-negative organisms in NICUs. The reason may be that gram-positive organisms, such as skin flora, are more likely to colonize the catheter during catheter insertion and use, whereas infections with gram-negative organisms are more commonly associated with the translocation of flora from the gut or respiratory or urinary tract (17). Djordjevic et al. reported that the most common causative agents isolated from NIs were Klebsiella-Enterobacter (39.3%), Escherichia coli (25.0%), coagulase-negative Staphylococci (16.1%), Acinetobacter spp. (10.7%), Candida albicans (5.4%), and Stenotrophomonas maltophilia (3.6%) (22). Pellizzer et al. reported that the most common causative agents isolated from HCA-BSIs were Staphylococcus aureus (17.3%), Pseudomonas aeruginosa (15.5%), Enterococcus spp. (15.2%), E. coli (12.1%), coagulase-negative Staphylococci (10.8%), and Candida spp. (8.5%) (23). Auriti et al. reported that the most common causative agents isolated from HCA-BSIs were coagulase-negative staphylococci (25%), Klebsiella pneumoniae (21.7%), C. albicans (25%), and P. aeruginosa (13%) (24). From Turkey, Tekin et al. found that the most common causative agents isolated from HCA-BSIs were Acinetobacter baumannii (48%), P. aeruginosa (32%), and Klebsiella spp. (6%) (1). We found that the most common causative agents isolated from HCA-BSIs were S. epidermidis (20.7%), Klebsiella spp. (26.7%), and Acinetobacter spp. (13.3%) (Table 2). However, these results indicate that gram-positive organisms, still the most common causative agents isolated from HCA-BSIs, also show that the recently increased incidence of Acinetobacter spp. and resistance of Acinetobacter spp. may cause serious health problems if the necessary measures are not taken (25, 26).
Recent studies have identified several risk factors for NIs in NICUs (9, 27). Pellizzer et al. reported that surgery, antibiotic exposure, antacid medications, leucopaenia, chemotherapy, use of steroids, length of hospitalization (> 5 days), ICU admission, tracheostomy, and exposure to indwelling devices were associated with a significantly increased risk of HCA-BSIs by univariate analysis, and that risk factors such as antibiotic exposure, surgical intervention, trauma, central venous catheter, urinary catheter, intubation, tracheostomy, length of hospitalization (15 days), Charlson index, and McCabe classification were independently associated (P < 0.05) with HCA-BSIs (23). Consistent with our study, Kishk et al. found that HCA-BSI was more frequent among low birth weight infants than high birth infants (28).
Length of hospitalization, gestational age, birth weight, mechanical ventilation, total parenteral nutrition, umbilical catheter, use of antibiotics, and intubation at birth were associated with a significantly increased risk of HCA-BSIs. Some studies (15, 17, 29) reported that surgery, orogastric tube, central venous catheter, and nasal continuous positive airway pressure were not associated with a significantly increased risk of HCA-BSIs. Djordjevic and Aurit found that low birth weight (< 1500 g), low gestational age at birth (< 32 weeks), first-minute Apgar score, endotracheal intubation at birth, mechanical ventilation and assisted ventilation by continuous positive pressure through nasal prongs, central venous catheter, parenteral nutrition, continuous enteral nutrition, premature rupture of membranes, cesarean section, male sex, aspiration, congenital anomalies, intracranial hemorrhage, and surgical intervention were associated with a significantly increased risk of HCA-BSIs; in the multivariate logistic regression analyses, only low gestational age (< 32 weeks) and central venous catheter were independent risk factors for HAIs (22, 24). In the present study we found that surgical operation, ventriculoperitoneal shunt, use of umbilical catheter, use of nasogastric or orogastric tube, use of urinary catheter, use of mechanical ventilation, surfactant, erythrocyte transfusion, plasma transfusion, thrombocyte transfusion, total parenteral nutrition infusion, intracranial hemorrhage, length of stay, fifth-minute Apgar score, and duration of total parenteral nutrition were all associated with a significantly increased risk of HCA-BSIs using univariate analysis. In the multivariate logistic regression analyses, only the fifth-minute Apgar score, use of erythrocyte transfusion, and surgical operation were independent risk factors for HAIs.
The main limitation of our study is the fact that it is a retrospective study with a relatively small sample size. Studies with more comprehensive analyses and a larger number of patients can provide further data on these variables.
5.1. Conclusion
This study identified the risk factors associated with HAIs in our NICUs that are necessary for HCA-BSIs prevention programs and found that infection control is a significant problem in NICUs. We suggest that preventive strategies for BSI in neonates in NICUs should continue to focus on limiting the use of invasive devices to reduce HAIs.