Materials and Methods
Study subjects
This parallel design, triple-blind, randomized and placebo controlled clinical trial was conducted on premenopausal women (19-52 years old) with benign breast tumor, whose disease was diagnosed by ultra-sonography imaging results, recruited from Nour-Nejat private hospital, Tabriz, Eastern Azerbaijan, between July 2013 and October 2014. The BBT patients did not have any surgical procedure or mastectomy prior to inclusion in the trial. Eligibility criteria included: being diagnosed with fibrocystic changes (n = 69), fibroadenoma (n = 11), written and oral informed consent, being at the interval of at least 2 years from diagnosis of BBD and no former history of malignancy in any part of the body. We excluded patients with smoking habits in previous years (ever and former smokers); pregnancy and lactating statue during the treatment; afflicted with acute and chronic illness including: cardiovascular disease, renal or liver malfunctions; other malignancies; hyperthyroidism and other hormone-related disorder (type 1 diabetes, adrenal gland disorders, polycystic ovary syndrome and hypoglycemia); gastrointestinal inflammatory illnesses (peptic ulcer, gastritis and inflammatory bowel syndrome); history of other benign lesions; any sign of bleeding and trauma reported by patients or physician; intolerance to the content of
BV juice; consumption of medications like anticoagulants (such as aspirin); omega-3 (> 2000 mg/d); glucocorticoids; methotrexate; alpha-tocopherol(> 400 IU/d) supplements, epilepsy-related drugs and any medical history related to chemo-, radio-, and hormone-therapy. The sample size was calculated based on information outlined by Gu
et al. (
16) and estimated as 30 patients with BBT at each group, but after considering the attenuated power of analysis for stratified random sequence generation, 30% further enrolment was planned in the study protocol (
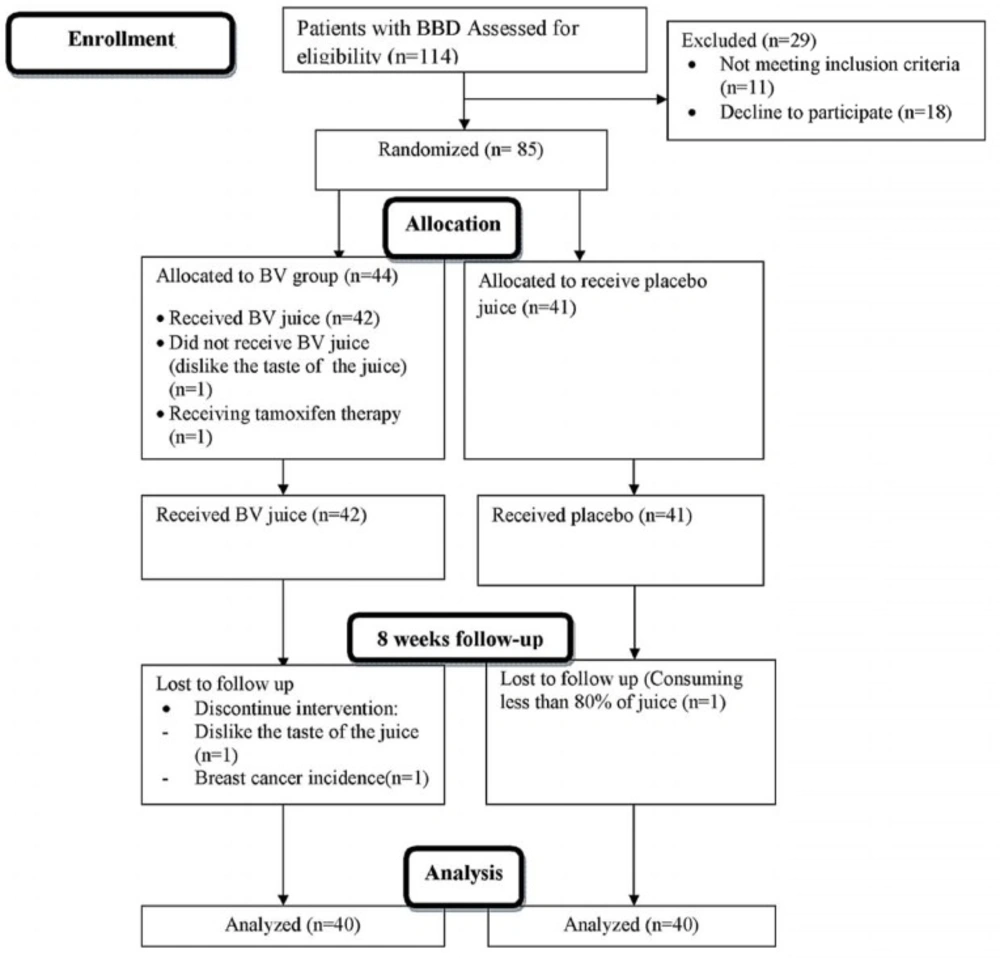
Figure 1). At last, 85 women diagnosed with BBD were included and randomly assigned into two groups via stratified random allocation. All participants received written informed consent form prior to enrolment, which is completed by each participant. The study was conducted due to the revised guidelines released in the Declaration of Helsinki. The study design was approved by Ethics Committee Center at Tabriz University of Medical Sciences (Ethics no: 9233). IRCT registration number is IRCT2012110511335N2.
Study design
The selected eligible participants were asked to follow a 7 days run-in period prior to the beginning of the interventions. Run-in period was performed in order to obtain a situation to reduce the possible interaction of other dietary resources containing isoquinoline alkaloid to reach a better adherence in 8 weeks. Generally, participants was also asked not to change their common life style, particularly their usual (i.e., habitual) diet. At first interview of run-in period, dietitian instructed the participants to fill 3 days collection of 24-h dietary record (two weekdays and one on a nearest weekend), by describing portion size of food servings through the food model guideline. A dietitian carried out questioning through a face-to-face interview. The eligible participants were randomly assigned to either intervention or placebo group. Randomization was applied using a list taken out from computer-generated randomization software.
All subjects were randomized to receive 8-weeks treatment with 480 mL doses of either BV juice or placebo daily both in lunch and dinner meals (a glass in each meal equal to 240 mL). Intervention for the duration of 8 weeks was planned for this trial. All tetra pack BV juice (240 mL) was prepared by Takdaneh Agro-Industrial Company (Takdaneh, Co. Ltd., Marand, East-Azerbayjan, Iran). Each serving of BV juice contained carbohydrates: 55 gr/500 mL; protein: 600 mg/500 mL; fat: 10 mg/500mL; calcium: 50 mg/500 mL; sodium: 100 mg/500 ML and vitamin C: 80 mg/500 mL.
| Characteristics | Placebo (n = 40)
| Intervention (n = 40)
| P-value* |
|---|
| Mean ± S.D. | Median | Mean ± S.D. | Median |
|---|
| Demographic data | | | | | |
| Age at diagnosis (years) | 38.45 ± 6.9 | 40.0 | 36.17 ± 7.6 | 40.0 | 0.16 |
| Age at firs delivery (years) | 21.4 ± 3.9 | 20.5 | 21.0 ± 3.8 | 19.5 | 0.66 |
| Age at first menses (years) | 13.4 ± 1.6 | 13.0 | 13.0 ± 1.5 | 13.0 | 0.75 |
| Dietary intake data | | | | | |
| Total calorie intake (kcal/day) | 10.26 ± 4.07 | 9.07 | 11.99 ± 6.19 | 10.68 | 0.49 |
| Protein intake (g/day) | 52.49 ± 19.20 | 47.24 | 56.41 ± 22.49 | 51.49 | 0.41 |
| Carbohydrate intake (g/day) | 1359 ± 457 | 1298 | 1407 ± 483 | 1272 | 0.21 |
| Fat intake (g/day) | 5.10 ± 3.05 | 4.60 | 4.28 ± 1.93 | 4.20 | 0.25 |
| Saturated fatty acids(g/day) | 32.89 ± 12.20 | 32.49 | 37.15 ± 13.96 | 35.05 | 0.04 |
| Mono saturated fatty acids(g/day) | 9.61 ± 4.19 | 9.18 | 10.65 ± 5.09 | 9.70 | 0.16 |
| Poly saturated fatty acids(g/day) | 10.47 ± 9.52 | 10.24 | 11.20 ± 10.34 | 10.36 | 0.25 |
| Dietary fiber (g/day) | 0.83 ± 1.16 | 0.76 | 0.69 ± 0.91 | 0.41 | 0.13 |
| Soluble fiber (g/day) | 113 ± 182 | 76 | 120 ± 99 | 84 | 0.64 |
| Insoluble fiber (g/day) | 13.31 ± 6.73 | 11.74 | 14.93 ± 5.66 | 13.48 | 0.61 |
Independent sample t-test was used to compare data. All data were expressed as mean±standard deviation (S.D.) and related median.
| Characteristics | Intervention(n = 40) | Placebo(n = 40) | p-value* |
|---|
| Histopathological characteristics |
| Fibrocystic | 34(85.0) ** | 35(87.5) | < 0.001 |
| Fibroadenoma | 6(15.0) | 5(12.5) | |
| Others | | | |
| Family history of BC |
| No | 35(87.5) | 30(75.0) | < 0.001 |
| Positive | 5(12.5) | 10(25.0) | |
| Family history of BBD |
| No | 40(100.0) | 39(97.5) | < 0.001 |
| Positive | 0 | 1(2.5) | |
| Smoker |
| Never | 40(100) | 40(100) | N/A |
| Ever | 0 | 0 | |
| Current | 0 | 0 | |
| Multivitamin use |
| No | 38(95.0) | 35(87.5) | < 0.001 |
| Yes | 2(5.0) | 5(12.5) | |
| Duration of multivitamin use (months) |
| ≤2 | 1(50.0) | 3(60.0) | 0.680 |
| >2 | 1(50.0) | 2(40.0) | |
| Vitamin E capsule use |
| No | 22(55) | 25(62.5) | 0.11 |
| Yes | 18(45) | 15(37.5) | |
| Omega3 capsule use |
| No | 33(82.5) | 28(70) | < 0.001 |
| Yes | 7(17.5) | 12(30) | |
Chi-square test was performed.
Data was expressed in the form of number of participants (relative frequency, %).
| Variable | Baseline (n = 40)
| 8-weeks follow-up (n = 40)
| Absolute treatment effect
| Relative treatment effect |
|---|
| n | Mean | S.D. | P | n | Mean | S.D. | P | Mean | 95%CI | Pc |
|---|
| Insulin (U/mL) |
|---|
| Control | 39 | 0.38 | 0.33 | N/A | 39 | 0.50* | 0.17 | N/A | N/A | N/A | N/A | 1.00 |
| BV | 35 | 0.49 | 0.43 | 0.09 | 35 | 0.51* | 0.22 | 0.72 | 0.10 | (-0.08-0.28) | 0.26 | 0.81 |
| C-peptide (ng/mL) |
| Control | 40 | 2.27 | 1.06 | N/A | 40 | 2.97* | 1.13 | N/A | N/A | N/A | N/A | 1.00 |
| BV | 40 | 2.56 | 1.12 | 0.23 | 40 | 3.42* | 1.44 | 0.16 | -0.15 | (-0.62-0.32) | 0.13 | 0.92 |
| FBS (mg/dL) d |
| Control | 40 | 92.22 | 14.73 | N/A | 40 | 87.85 | 12.14 | N/A | N/A | N/A | N/A | 1.00 |
| BV | 40 | 89.25 | 9.33 | 0.28 | 40 | 91.00 | 10.85 | 0.22 | -6.12 | (-12.7-0.50) | 0.97 | 1.06 |
| HOMA-IRe |
| Control | 39 | 0.09 | 0.09 | N/A | 40 | 0.11 | 0.04 | N/A | N/A | N/A | N/A | 1.00 |
| BV | 39 | 0.10 | 0.09 | 0.34 | 37 | 0.11 | 0.06 | 0.19 | 0.01 | (-0.03-0.06) | 0.44 | 0.84 |
| HOMB f |
| Control | 39 | 13.30 | 49.87 | N/A | 39 | 9.69* | 6.54 | N/A | N/A | N/A | N/A | 1.00 |
| BV | 36 | 10.26 | 15.86 | 0.05 | 36 | 9.80* | 9.49 | 0.05 | 375 | (21-730) | 0.86 | 1.44 |
| QUIKI g |
| Control | 39 | 0.72 | 0.15 | N/A | 40 | 0.62* | 0.06 | N/A | N/A | N/A | N/A | 1.00 |
| BV | 38 | 0.67 | 0.13 | 0.15 | 37 | 0.62* | 0.07 | 0.94 | -0.04 | (-0.11-0.02) | 0.29 | 0.94 |
| G:I ratio h |
| Control | 39 | 345.08 | 219 | N/A | 39 | 186.01* | 49.14 | N/A | N/A | N/A | N/A | 1.00 |
| BV | 36 | 271 | 194 | 0.11 | 36 | 185.23* | 79.07 | 0.92 | 0.15 | (-0.05-0.35) | 0.28 | 0.78 |
Paired t-test was performed to compare within changes in intervention group during the study.
Independent sample t-test was performed between group.
Repeated measure of ANOVA was carried out in the main effect of model.
Homeostatic model assessment.
Assessment of B-cell functionality.
quantitative insulin sensitivity check index glucose to insulin ratio.
Glucose to insulin ratio.
| Variable | Placebo group | BV group | P-value b |
|---|
| Insulin (U/mL) | | | |
|---|
| Model 1c | 0.54 ± 0.02a | 0.55 ± 0.02 | 0.783 |
| Model 2 d | 0.54 ± 0.02 | 0.55 ± 0.2 | 0.669 |
| C-peptide (ng/mL) | | | |
| Model 1 | 2.97 ± 0.07 | 3.33 ± 0.12 | 0.029 |
| Model 2 | 2.96 ± 0.07 | 3.35 ± 0.13 | 0.018 |
| FBS (mg/dL) | | | |
| Model 1 | 87.64 ± 0.40 | 94.70 ± 1.24 | < 0.001 |
| Model 2 | 87.70 ± 0.41 | 94.20 ± 1.44 | < 0.001 |
| HOMA-IR e | | | |
| Model 1 | 0.13 ± 0.01 | 0.14 ± 0.01 | 0.183 |
| Model 2 | 0.13 ± 0.01 | 0.13 ± 0.01 | 0.633 |
| HOMB f | | | |
| Model 1 | 666 ± 78 | 973 ± 147 | 0.114 |
| Model 2 | 664 ± 76 | 977 ± 142 | 0.048 |
| QUIKI g | | | |
| Model 1 | 0.66 ± 0.01 | 0.65 ± 0.01 | 0.447 |
| Model 2 | 0.66 ± 0.01 | 0.65 ± 0.01 | 0.359 |
| G:I ratio h | | | |
| Model 1 | 0.62 ± 0.02 | 0.63 ± 0.02 | 0.697 |
| Model 2 | 0.62 ± 0.01 | 0.63 ± 0.01 | 0.252 |
All data are expressed in geometric mean ± S.E..
This p-value obtained from performing ANCOVA.
Weighted least square was performed in ANOVA with adjustment for baseline variable (model 1).
Model 2 obtained from performing ANCOVA after adjustment for the frequency of lactation (n) and BMI (kg/m2) at baseline in addition to baseline variable.
Homeostatic model assessment.
Assessment of B-cell functionality.
quantitative insulin sensitivity check index.
Glucose to insulin ratio.
CONSORT flow diagram of the progress through different time compartments of a parallel randomized trial of BV and BV placebo received groups during 8 weeks of intervention. BBD, breast benign tumor disorder; BV, Berberis vulgaris
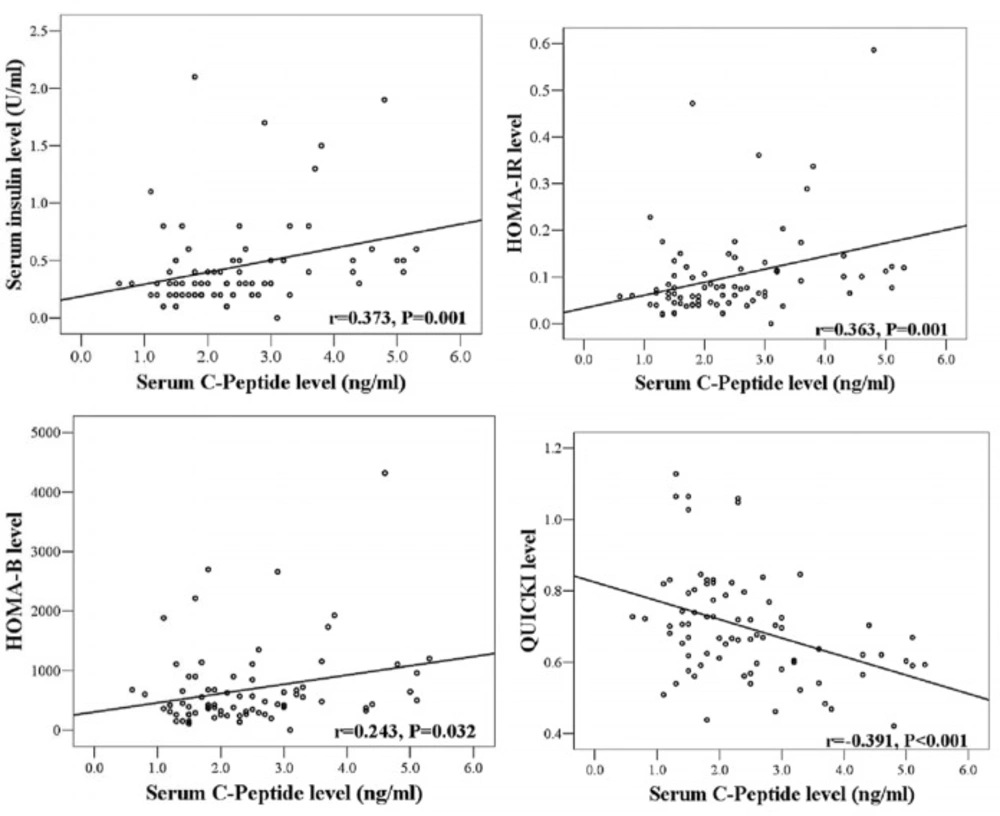
Pearson correlation coefficient value obtained to show the validity of insulin-related indices (dependent variable) in association with serum C-peptide concentration (independent variable) at baseline compartment of the study (n = 80
Spectrophotometric method measured absorbance of berberine at 418 nm in
BV juice (
17). After measuring five different samples of
BV juices, the average berberine content was determined 2.03 ± 0.03 μM/mL. The company declares no addition of any preservatives in
BV juice tetra-pack.
Weekly checklist of BV consumption was handed in to the eligible patients for assessing the probable intolerance to interventions, detailing undefined events, doubt or accidental consumption, and other medical events. If weighted amount of remaining juice in bottle was more than 20% of total amount of juice, the subject was considered to be none respondent to the intervention. In addition, bottles were collected in every two weeks. During the intervention, data on 3-day 24 h dietary and physical activity records were collected once in every two weeks. Physical examinations at these visits were done by physician in order to determine any clinical changes during the study, including malignancy, diabetes, hepatic complications and pregnancy after enrolment and during the interventions, which were considered as exclusion criteria. Intervention follow up continued until December 2014.
Participants in placebo group consumed 480 mL of placebo juice had a content which was normalized to become identical in calorie, vitamin content, taste, size and color to the
BV juice. To meet the allocation concealment criteria, white opaque plastic was used to cover juice pack similarly. Juice packs were provided in every two weeks (
18). Subjects were asked to store juices in refrigerator at 4ºC. Sequence generation and allocation concealment were listed and marked by designer of study and implemented by clinic personnel who were unaware of allocation at the time of enrolment. Participants, clinic care givers who had been responsible to hand in plastic bags and also laboratory personnel were blinded. The average of nutrients intake level for each participant obtained from 24 h dietary records at baseline were analyzed by Nutritionist IV software (version 3.5.2; 1994, N-Squared Computing, San Bruno, CA). To assess the concurrence of dietary data, a validated food frequency questionnaire with 136 food items (
19) was used.
Biochemical analyses
Serum samples of 80 patients were collected by considering overnight 12 h fasting. Blood sampling process had not being performed in duration of 3rd till 5th days of menstruation (follicular phase) both at baseline and after the 8-week follow-up period. Blood were transferred centrifuged (Gallenkamp centrifuge) at 3000 × g at 20 °C for 10 minutes to separate serum supernatant. Sera samples transferred into 1.5mL microtubes and stored at -70 °C until sample analysis. Outcomes of the study consist of serum levels of C-peptide, fasting blood sugar (FBS) and insulin. They were assessed using a specific enzyme linked immunosorbent assay (ELISA) kits for fasting blood sugar (FBS) (Pars-Azmoon, Cat. No: 5825; Tehran, Iran), insulin by Monobind (Cat No: 5825-300; California, USA), and C-peptide using Monobind kit (Cat No: 2725-300; California, USA). The internal coefficient variations of biomarkers were reported about 92%. The measurements were carried out following instruction provided by manufacturer. The HOMA related indices were calculated using the HOMA-IR= [FBS (mg/dL) × insulin (IU)/405] and HOMA-B= [(360 × insulin (IU)]/ [(FBS (mg/dL)-63] × 100. The quantitative insulin sensitivity check index (QUICKI) was estimated using 1/[(logarithm of insulin+ logarithm of FBS)]. To attenuate systematic errors for each biomarker, measures were done at the same time in a laboratory run and random order. A numeric label code was used instead of each patient’s name, to attain blinding at laboratory analysis.
Statistical analysis
Statistical analysis was carried out using SPSS software package (version 13.0; SPSS Inc.). Paired samples t-test was used to compare mean values of a variable from baseline to the endpoint of study within each group. Independent sample t-test was used to compare a variable between BV and placebo groups at certain time point. The mean change in the variable from baseline to the 8 weeks of follow-up between the two arms of intervention was calculated by absolute treatment effect and tested by a repeated-measures linear mixed model. The relative effect is a term used to define probability of an outcome in one treatment group relative to that in the placebo group and likewise. The odds ratio (OR) can interpret the proportional change in the treatment group relative to placebo group. Dependent variable was adjusted for baseline data and estimated through a weighted least squares (WLS) regression model. Subsequently, linear mixed model was used to consider covariates including frequency of lactation (n), and body mass index (BMI, kg/m2) at baseline. P values less than 0.05 has been reported as statistically significant.