Selection of formulation compositions
As shown in
Table 1, Labrafil M 1944CS was showed comparatively higher ibuprofen solubility (29.3 ± 3.13 mg/mL) than other screened oils and was selected as oil phase for this study. But, Tween 80 with HLB value 15.0 and relatively less drug solubility (11.29 ± 2.66 mg/mL) than other screened surfactants, was selected as surfactant (
Table 1).
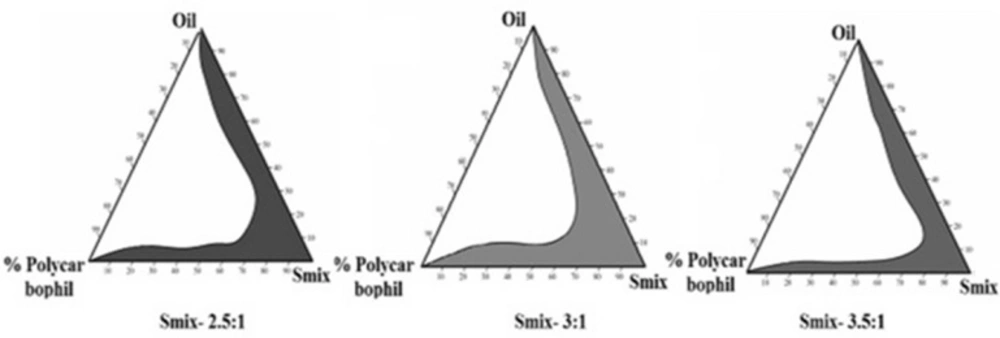
Since drug solubility was more in selected oil than that of surfactant, more control over the drug release was observed due to the reservoir nature of the oil phase and less amount of oil was required to accommodate drug for nasal delivery. So, relatively less surfactant and cosurfactant will be required to stabilize the oil to develop a more suitable microemulsion system. Pseudo-ternary phase diagrams as shown in
Figure 1 showed relatively more microemulsion zone was observed with Smix (3:1). More microemulsion zone indicated more stability with less bi-continuous phase and was thus used to develop microemulsion formulation (
21).
Formulation development
In order to assess the effect of independent variables on the responses like average globule size, viscosity, flux, mucoadhesive potential and % drug release, three independent variables (X1, X2, and X3) were statistically analyzed based on the response surface method (RSM) using Design-Expert
® software and the results of multiple regression analysis are summarized in
Table 2.
It was also observedas shown in
Table 3, average globule size, viscosity, flux, mucoadhesive potential and % drug release of ibuprofen was noticeably influenced by the independent variables and their interaction effect which were illustrated in the polynomial Equations 1 to 5.
Analysis for all responses indicated the suitability of quadratic model (p < 0.05). By running ANOVA, the final equations for all responses i.e., average globule size, viscosity, flux, mucoadhesive potential and % drug release in their respective coded value were obtained as follows.
Globule Size = + 66.87 + 1.89 × A – 3.98 × B + 5.71 × C – 0.58 × (A × B) + 0.89 × (B × C) + 2.54 × (A × C) + 1.66 × A2 – 1.54 × B2 + 3.88 × C2 (1)
Equation 1 showed average globule size of MMEI was mainly influenced by Labrafil M 1944CS, Tween 80 - Transcutol P concentration ratio and polycarbophil with their interactions. For development of an effective intranasal drug delivery system, globule size plays vital role as it influences the
in-vivo absorption of drug from the formulations (
36). The globule size is a crucial characteristic of microemulsion formulation because it influences drug release rate and hence the
in-vivo profile of the drug. Consequently, optimizing microemulsion with smaller globule size to ensure rapid penetration through the nasomucosal layers was one of the aims of this study. The observed globule size of the formulations ranged from 42 nm to 88 nm (
Table 2).
The influence of the screened variables on the average globule size of MMEI is presented in Equation 1.
The obtained results in this design indicated that oil concentration (X1) and mucoadhesive polymer concentration (X3) has significant effect on the mean globule size i.e., p = 0.0003. As depicted, increasing oil concentration from 0.1 mL to 0.5 mL and mucoadhesive polymer concentration from 0.25% to 0.75% caused a significant increase in average globule size.
This may be due to the fact that Smix at its increased concentration could able to reduce the interfacial tension between oil and aqueous phase. But at higher amount of oil with same Smix concentration, the hydrophobicity oil was not being masked by Smix, resulting into more interfacial tension and increased globule size. Mucoadhesive polymer also found to increase the globule size which may be due to the fact that it was capable of absorbing water and swell which in turn disturb the hydrophilic-lipophilic balance of the system.
Viscosity = + 34.44 + 0.31 × A + 0.26 × B + 1.87 × C + 0.68 × (A × B) + 2.15 × (A × C) – 0.78 × (B × C) + 0.44 ×A2 – 0.28 × B2 +1.41 × C2 (2)
It (Equation 2) suggested that viscosity was mainly influenced by % polycarbophil. Moreover interaction effect of Labrafil M 1944CS and polycarbophil got positive effect on viscosity of MMEI. Viscosity was mainly influenced by % polycarbophil which may be due to the fact that mucoadhesive polymer (polycarbophil) possesses hydrogen bonding group along with its extensive hydration property. Polycarbophil is capable of imbibing relatively more water and increases the viscosity of formulation hence drug release was controlled as such. This may be due to the influx of more dissolution fluid into the formulation.
Flux = + 31.13 - 0.88 × A +1.52 × B - 1.17 × C + 0.27 × (A×B) - 1.05 × (A × C) – 0.43 × (B × C) – 0.45 × A2 + 0.83 × B2 - 1.55 × C2 (3)
Labrafil M 1944 CS due to its reservoir action and Polycarbophil due to viscosity enhancing property showed negative effect on release rate and hence the flux. The results obtained in this design indicated that oil concentration (X1) and mucoadhesive polymer concentration (X3) has significant effect on the flux through sheep nasal mucosa (p = 0.0001). However, Smix showed positive effect on flux due to the fact that both Tween 80 and Transcutol P capable of altering the permeation behavior of the membrane by changing the fluidization of lipid enabling the drug molecule to permeate through rapidly.
Retention Time = + 4.18 + 1.19 × A - 0.21 × B + 3.55 × C + 0.35 × (A × B) + 2.79 × (A × C) + 0.29 × (B × C) + 0.87 × A2 – 0.76 × B2 + 1.04 × C2 (4)
Labrafil M 1944CS and Polycarbophil showed more positive effect while Smix though non-significant, showed negative effect as shown in Equation 4. Mucoadhesive nature of the polymer may be because of the presence of high density of hydrogen bonding groups which could combine with mucin more strongly as shown in Equation 4 (
p = 0.0021) (
24). Moreover, interaction effect of Labrafil M 1944CS and polycarbophil got positive effect; this may be due to the mucoadhesive and viscosity enhancing property of the polymer.
% Drug Release = + 74.40 – 2.58 × A + 1.87 × B - 2.63 × C + 0.88 × (A × B) – 1.95 × (A × C) – 1.89 × (B × C) + 1.34 × A2 - 0.67 × B2 - 1.34 × C2 (5)
Drug release was heavily negatively influenced by Labrafil M 1944CS and polycarbophil, while mixture of Tween 80 and Transcutol P showed positive effect as shown in the Equation 5. Drug release after 8 h ranged from 79% to 96% as shown in
Table 2. Formulation variables of MMEI influenced the drug release as shown in Equation 5. Drug release was heavily but inversely influenced by Labrafil M 1944 CS and polycarbophil, while mixture of Tween 80 and Transcutol P (3:1) showed positive effect as shown in the Equation 5. Labrafil M 1944 CS decreased the drug release from the formulation due to its reservoir property and polycarbophil because of its viscosity enhancing property. Smix was found to increase ibuprofen release because of the enhanced water solubility of poorly water soluble ibuprofen. This action may be coupled with the water absorption capacity of the screened mucoadhesive polymer
i.e., polycarbophil.
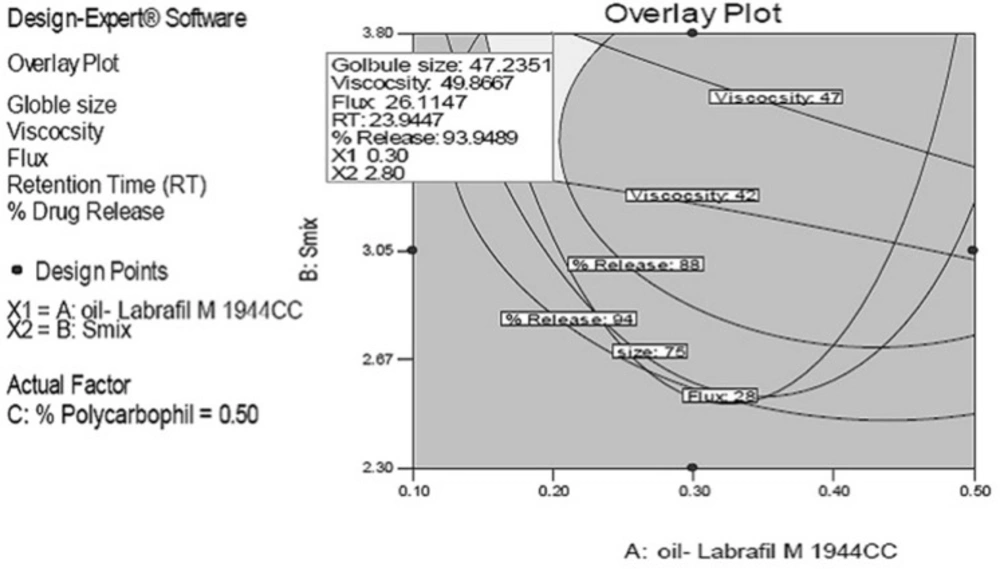
The rationale of optimization through factorial design was to obtain the defined targets for all responses simultaneously with respect to the predefined ones. In this study, globule size, viscosity and retention time (RT indicating the mucoadhesive property) was set to maximum without affecting release while flux and release were set to maximum. Overlay plots of all responses for predicted formulations at three different water contents as the actual factor are depicted in
Figure 2. The grey region stands for formulations with minimum globule size, maximum release and maximum flux.
In order to confirm the desirability of the optimized MMEI, five formulations were prepared experimentally and all responses were evaluated as given in
Table 3. It was observed that experimentally found data were matching with the predicted responses for all five MMEIs and hence, the optimization process was verified.
MMEI characterization
MMEIs with 0.5% w/v of polycarbophil, 0.3 mL Labrafil M 1944 CS, 3.70 mL of Smix (Tween 80 and Transcutol P at 3:1 ratio) showed the lowest globule size, highest flux, optimum viscosity and highest drug release as shown in
Table 4 and hence was considered as optimized formulation.
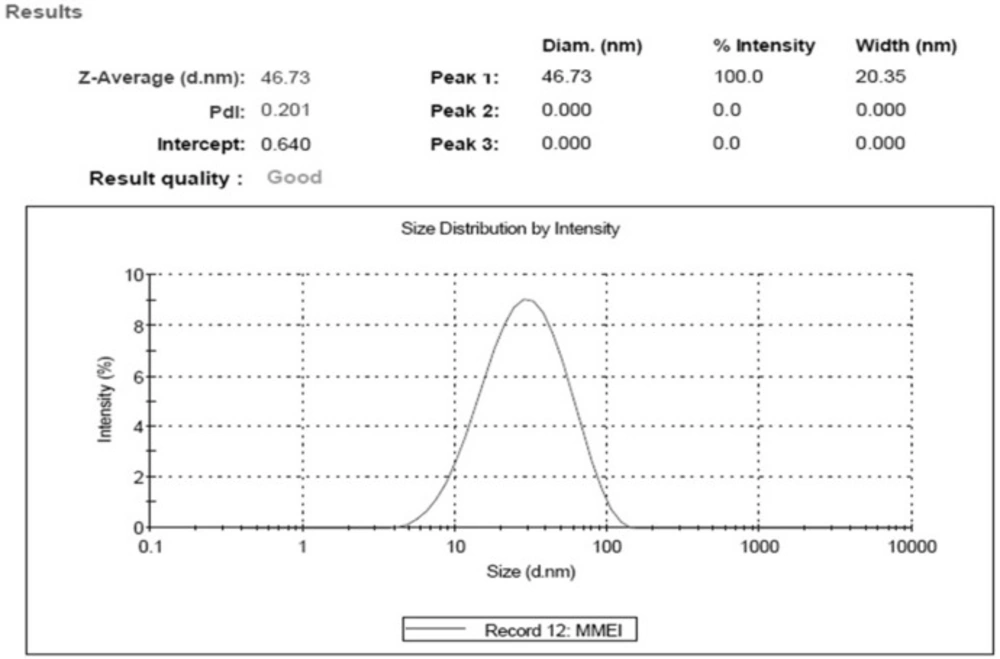
Optimal MMEI was found to be transparent with globule size 46.73 nm ± 3.11 with PdI value (0.201 ± 0.19) as shown in
Figure 3.
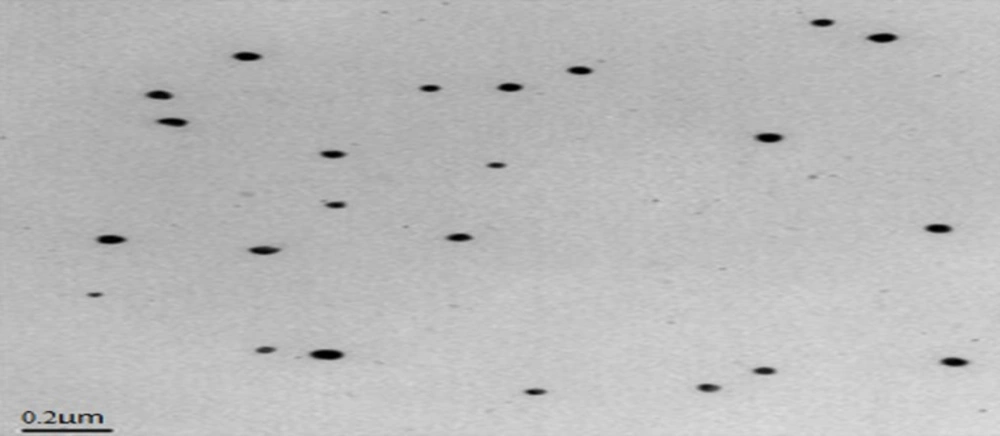
PdI value and TEM results as shown in
Figure 4 indicated the mono-dispersity of the developed MMEI with nano globule size range. Intranasal permeation of drug is believed to be influenced by monodispered nano formulations (
36).
Zeta potential of the formulation was -24.4 mV ± 3.27. Zeta potential indicated stability of formulation as globules did not show intense aggregation or repulsion (
37) and hence monodispersity and the shelf life of the formulation will be maintained. Viscosity of MMEI was found to be ranging from 42.37 Ps to 48.37 Ps at 25 °C. Mucoadhesive potential of MMEI in terms of retention time of formulation was found to be 23.1 min ± 1.2 which was adequate enough to get adhere on the nasal mucosa.
Moreover, the obtained result indicated that physical properties of MMEIs were profoundly influenced by independent variables and their combinations. Developed MMEI through its viscosity data showed to have adequate adhesion property which enhanced the adhesion property of formulation on the nasal mucosa. This again can be considered as a contributing factor for enhancement in the efficacy of MMEI by minimizing the nasal clearance.
The percentage of drug release showed that 94.77% ± 4.25 of drug was sustained released for 8 h from MMEI. From the data, it was observed that the release rate was decreased with increase amount of independent variables like oil and mucoadhesive polymer while surfactant-cosurfactant mixture was increased the drug release.
The flux was found to be of 25.82 [µg/(cm
2 h)] The effect of oil, mixture of surfactant and co-surfactant and polycarbophil on different properties of microemulsion and drug penetration capacity was evaluated by RSM with Box-Behnken design and the results indicated that MMEI system had a significant permeation enhancement effect for intranasal delivery of ibuprofen. This can be attributed to factors including, higher solubility of ibuprofen in oil phase, less solubility in surfactant and optimized viscosity due to polycarbophil (
38). The flux data revealed rapid permeation through nasal mucosa which may be due to the relatively smaller globule size and cumulative penetration action of surfactant, co-surfactant and oil by altering the fluidization lipid of nasal mucosa. Moreover, the rapid permeation of ibuprofen through developed MMEI was supported by the enhanced mucoadhesion of the formulation on the nasal mucosa.
Nasal Ciliotoxicity study
No mucociliary alteration of mice nasal mucosa was observed following intranasal administration of MMEI (
Figure 5) whereas complete destruction of the nasal mucosa was observed with positive control animals. Results of nasal ciliotoxicity did not reveal any toxicity issues which supports the acceptability of MMEI for intranasal application.
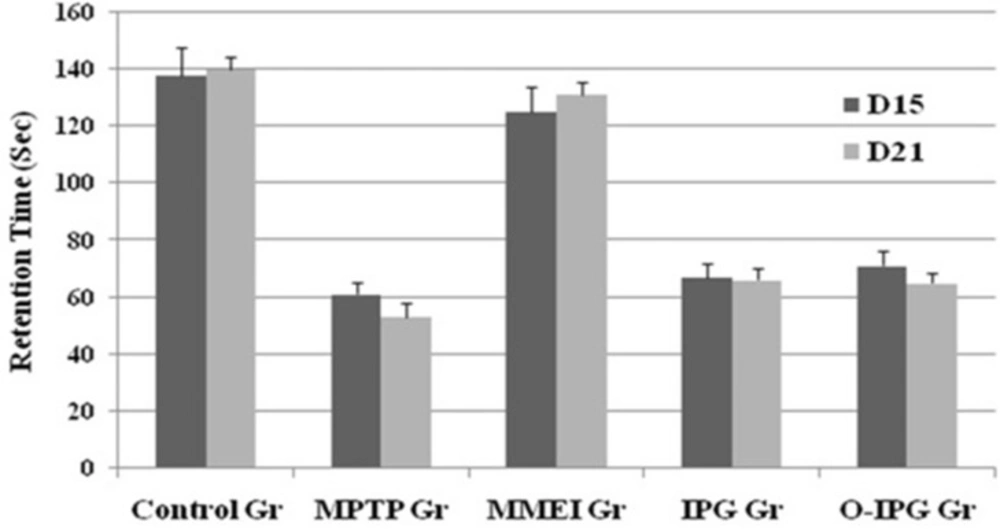
Assessment of spontaneous activity and muscular coordination
A noticeable DA turnover elevation was observed for intranasal MMEI treated group compared to MPTP control group (
p < 0.05). As shown in
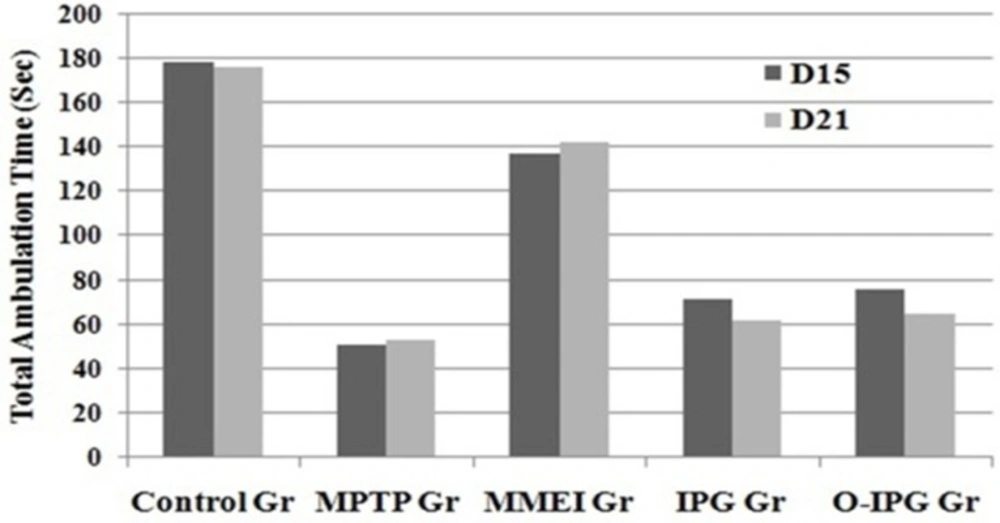
Figure 6, retention time was found to be 53 to 67 sec for the MPTP treated group compared to 125 to 131 sec for the ibuprofen treated group. Further, a significant reduction in total ambulation time was observed in MPTP-intoxicated group as compared to normal controls. Total ambulation time for the MPTP treated group was around 50 sec, in comparison to 137 to 142 sec for ibuprofen treated group. Moreover the total ambulation time for the MMEI treated group was significantly higher as compared to the MPTP-intoxicated group (122 sec v/s 47 sec).
Ibuprofen treatment (2.86 mg/kg) through intranasal MMEI as in third group of animals significantly (
p < 0.05) improved the muscular coordination activity as compared to MPTP control as shown in
Figure 6. Further, MPTP-intoxicated group showed steep reduction in total ambulation time as compared to ibuprofen treated group as shown in
Figure 7.
Since MPTP is a toxin, the reduced level of DA, DOPAC and HVA in MPTP treated animals reflect the inflammation of the dopaminergic nerve endings. So the developed formulation through nasal route bypassed the barriers and reached the neural part with desired concentration to exert the anti-inflammatory action. Elevations of these parameters in MMEI pre-treated (intranasal) animals provide direct evidence of neuroprotection by the MMEI.
Dopamine and its metabolites assessment in brain
Striatal DA content after MPTP intoxication decreased to 29.92% (4.68 ± 0.77) which was elevated to 58.21% (9.12 ± 0.58) following administration of MMEIin comparison to normal control (15.67 ± 1.54). So MPTP intoxication significantly (
p < 0.05) decreased striatal DA contentto less than one third to that of control. In-addition, a concomitant elevation of DA turnover was also observed in MPTP induced mice after 15
th day of ibuprofen dose as shown in
Table 5.
Immune-histochemistry study
Further, in order to generate direct evidence of neuroprotective action, immune-histochemistry study was performed. Density of striatal dopaminergic nerve terminals (TH density in striatum) was found to be 4.5 ± 1.21 for MPTP treated group. TH density in striatum for MMEI treated group was found to be 14.9 ± 1.43 and 22.46 ± 1.27 on 15
th and 21
st day of the test respectively. MPTP resulted in significant decrease in neural density substantia nigra, when compared to control group (
p < 0.05). However, nasal administration of ibuprofen through MMEI increased TH expression in substantia nigra and density of striatal dopaminergic nerve terminals as shown in
Figure 8 compared to MPTP group (
p < 0.05).
Figure 8B showed complete nerve destruction while regeneration was observed with ibuprofen treated groups. Significant differences was noticed for MMEI treated group as shown in
Figures 8C and 8D at 15
th and 21
st day of study than that of
Figure 8E, which is ibuprofen dispersed gel group (IPG). MPTP resulted in a significant decrease in TH density in striatum and TH-positive neurons in Sn as compared with the control group (
p < 0.05).
This may be due to the fact that MMEI provides control release of ibuprofen while IPG. The mechanisms of the neuroprotective effects ibuprofen have earlier been linked to its anti-inflammatory PPARγ agonistic properties (
4,
5). Ibuprofen has also been reported to protect against neurodegeneration mediated by reactive oxygen species and glutamate excitotoxicity. So the neuroprotection observed in this study by MMEI can also be attributed to these factors (
39,
40). Thus, this study establishes MMEI as a suitable alternative to oral ibuprofen for potential application against PD.

![Result of nasociliotoxicity study showing the nontoxicity of developed MMEI. 5[A], 5[B] and 5[C] are representative of Saline, Propranolol and developed MMEI treated mucosal part respectively](https://brieflands.com/journals/ijpr/articles/124744/figures/ijpr-17-023-g005-preview.webp)
![Effects of ibuprofen on MPTP-induced DA terminal loss in striatum and dopaminergic neuronal death in Substantia nigra, [A] Saline [B] MPTP treated Mice, [C] and [D] ibuprofen treatment after 15<sup>th</sup> day and 21<sup>st</sup> day, [E] Treated with IPG. Normal control <i>vs</i> MPTP (#<i>p </i>< 0.05) and MPTP <i>vs</i> treated group (*<i>p </i>< 0.05](https://brieflands.com/journals/ijpr/articles/124744/figures/ijpr-17-023-g008-preview.webp)

