As stated before, the purpose of this study was to develop and evaluate a vagino-adhesive propranolol hydrochloride gel with potential use in short-term contraception. To achieve this, various mucoadhesive polymers were utilized to prepare the gel formulations. Different tests (mentioned in the previous section) were performed on these formulations in order to gain a formulation with desirable characteristics. The results obtained would be presented and discussed in the following sections.
Formulation and characterization of propranolol HCl gels
In the process of formulating the vagino-adhesive propranolol HCl gels, it was observed that formulations F
19 – F
28 containing different concentrations of Na CMC and carbomers (C934 and C940) were not able to form gel in the aqueous solution containing propranolol hydrochloride. This observation could be attributed to the fact that carbomers; based on their anionic nature and large number of acidic groups available in their polymeric structure; tend to interact with cationic substances. Propranolol hydrochloride, which is a cationic drug, and carbomers interact ionically, giving rise to the formation of insoluble complexes which significantly affect drug release properties and mucoadhesiveness (
23). The same phenomenon would stand for explanation of the interaction observed between Na CMC and the drug, as this polymer also possesses an anionic nature. Hence, formulations F
19 – F
28 were left out of further studies. Physical appearances and apparent viscosities of propranolol HCl gel formulations F
1− F
18 are given in
Table 3. Formulations F
1, F
5, F
6, F
10, F
11 and F
15 had low and or relatively low apparent viscosities. A low-viscosity vaginal gel formulation is not as efficacious as a high-viscosity vaginal gel for use as a contraceptive gel, since rheological properties of spermicidal vaginal gels have considerable influence on their contraceptive success. As the consistency of the applied product increases, its efficacy may also increase as result of becoming more tenacious and more resistant to sperm migration, and consequently decreasing the capability of sperm to reach the site of fertilization (
8).
Formulations F4, F9, F14 and F18 showed very high apparent viscosities and gels with lumps rather than smooth gels, were formed. Hence, all the aforementioned formulations were excluded from further studies. Among the rest of the formulated gels, formulations F2, F3, F7, F8, F12, F13, F16 and F17 which exhibited suitable apparent viscosities (relatively high or high) as well as good physical appearances, were used for further studies.
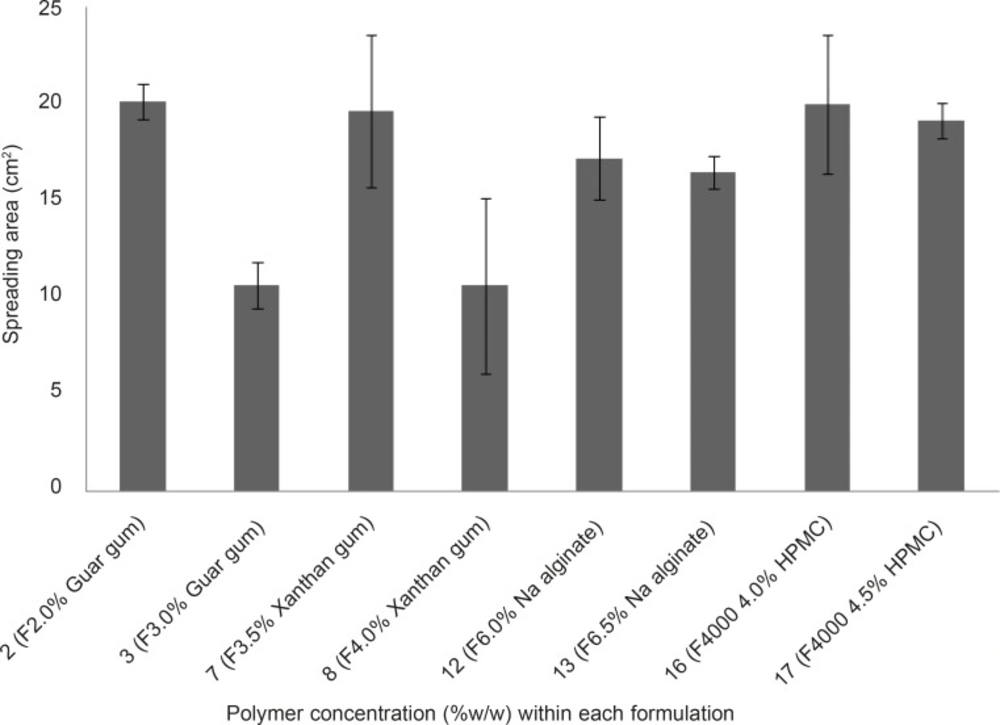
Comparison of spreading area of vagino-adhesive propranolol HCl gel formulations (F2, F3, F7, F8, F12, F13, F16 and F17). Data are expressed as mean ± SD (n = 3).
Spreadability measurement of propranolol HCl gel formulations
The spreading area of propranolol HCl gel formulations F
2, F
3, F
2, F
8, F
12, F
13, F
16 and F
17 was measured according to the technique explained earlier. The results are shown in Figure 3. The spreading areas of these formulations were in the following order: F
2 > F
16 > F
7 > F
17 > F
12 > F
13 > F
8 > F
3. Data obtained were statistically analyzed using one-way ANOVA, followed by Tukey post-hoc test. It was found that the difference in spreading area between the propranolol HCl gel formulation, showing the highest spreadability (F
2, containing 2% w/w guar gum) and formulations F
3 and F
8 was statistically significant (p < 0.05), whereas this difference between the gel formulation F
2 and all other tested formulations was statistically insignificant ( p > 0.05). Bachhave
et al. developed a vaginal gel of fluconazole. They considered a spreading area of 40.69 cm
2 as good spreadability (
17), while the highest spreading area obtained in our study was 20.15 cm
2 ± 0.92 which was found to be poor in comparison to that obtained for fluconazole vaginal gel. The reason for poor spreadability of all the developed propranolol HCl gel formulations was their high viscosities due to their high polymer concentration. However, in case of contraceptive vaginal gels, having high viscosity not only speaks in favor of better contraceptive efficacy, but also increases the mucoadhesivity and retention of the gel formulation in the vaginal canal (
6,
8).
| Formulation code | Physical appearance | Apparent viscosity | Formulationcode | Physical appearance | Apparent viscosity |
|---|
| F1 | Transparent, light green color, without lumps | Low | F10 | Translucent, light yellow color, without lumps | Low |
| F2 | Transparent, light green color, without lumps | Relatively high | F11 | Translucent, light yellow color, without lumps | Relatively low |
| F3 | Transparent, light green color, without lumps | high | F12 | Translucent, light yellow color, without lumps | Relatively high |
| F4 | Transparent, light green color, with lumps | Very high | F13 | Translucent, light yellow color, without lumps | high |
| F5 | Translucent, white color, without lumps | Low | F14 | Translucent, light yellow color, with lumps | Very high |
| F6 | Translucent, white color, without lumps | Relatively low | F15 | Transparent, colorless, without lumps | Relatively low |
| F7 | Translucent, white color, without lumps | Relatively high | F16 | Transparent, colorless, without lumps | Relatively high |
| F8 | Translucent, white color, without lumps | high | F17 | Transparent, colorless, without lumps | high |
| F9 | Translucent, white color, with lumps | Very high | F18 | Transparent, colorless, with lumps | Very high |
Assessment of mucoadhesive strengths of propranolol HCl gels
The mucoadhesive strengths of propranolol HCl gel formulations (F
2, F
3, F
7, F
8, F
12, F
13, F
16 and F
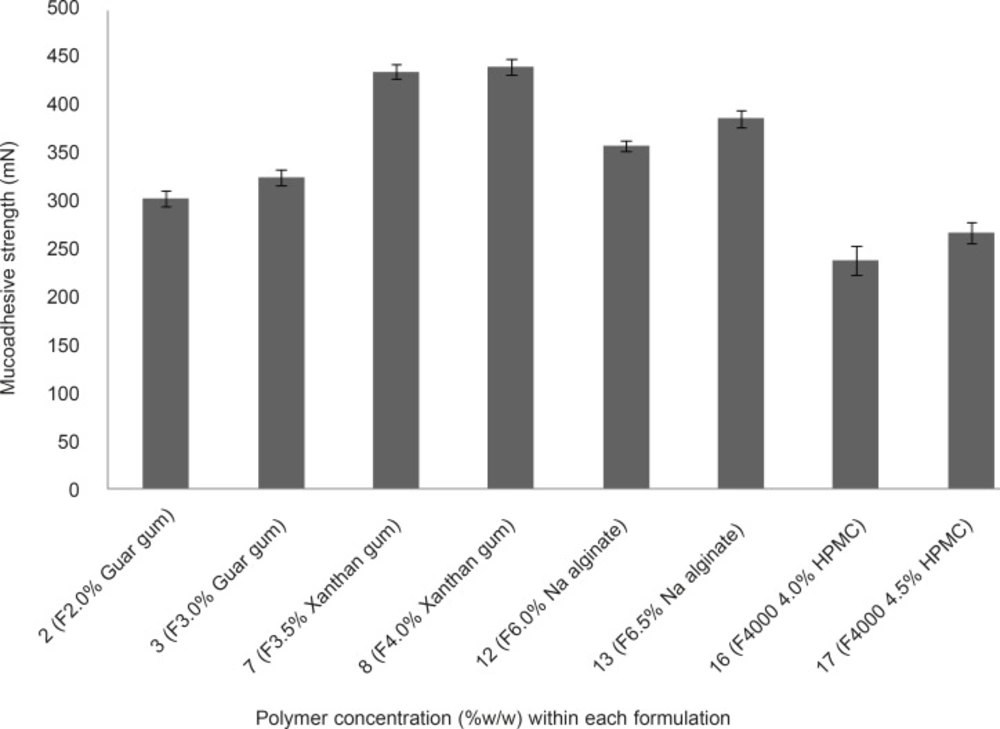
17) were examined and results are shown in Figure 4. It is evident from Figure 4 that, in case of formulations containing the same polymer but at different concentrations (
e.g. F
2 and F
3, as compared together), when the concentration of the polymer increased the mucoadhesive strength escalated, accordingly. This phenomenon can be attributed to the fact that, at lower concentration of the polymer chains, there is an inadequate and unstable interaction between the polymer and the mucosal layer resulting in lower mucoadhesive properties (
7). The mucoadhesive strengths observed, were in the following order: F
8 > F
7 > F
13 > F
12 > F
3 > F
2 > F
17 > F
16. Propranolol HCl gel formulations F
7, F
8 (containing 3.5 and 4.0% w/w xanthan gum, respectively), F
12 and F
13 (containing 6.0 and 6.5% w/w sodium alginate, respectively), showed statistically significant (p < 0.05, one-way ANOVA and Tukey post-hoc test) higher mucoadhesive strengths as compared to formulations F
12, F
13 (containing 2.0 and 3.0% w/w guar gum, respectively), F
16 and F
17 (containing 4.0 and 4.5% w/w HPMC 4000, respectively).This finding can be explained by the fact that the presence of charged functional groups in the polymer chains, which can be observed in xanthan gum and sodium alginate (presence of negatively charged carboxyl groups), may render them as polyelectrolytes and this has a marked effect on the strength of mucoadhesion due to the formation of strong hydrogen bonds between the polymer functional groups and the mucosal layer as compared to neutral polymers such as guar gum and HPMC. In general, anionic polyelectrolytes have been found to form stronger mucoadhesive bond when compared to the neutral polymers (
7). Propranolol HCl gel formulations F
8, F
7, F
13 and F
12 showed the highest mucoadhesive strengths among all the tested formulations. However, formulations F
3, F
8, F
13 and F
17 were considered as the chosen formulations for further assessments. The reason for selecting these formulations, was to investigate how an individual type of polymer can affect the propranolol HCl release from the gel matrix.
Mucoadhesive strength of vagino-adhesive propranolol HCl gel formulations. Data are expressed as mean ± SD
Determination of in-vitro drug release profiles from the chosen formulations
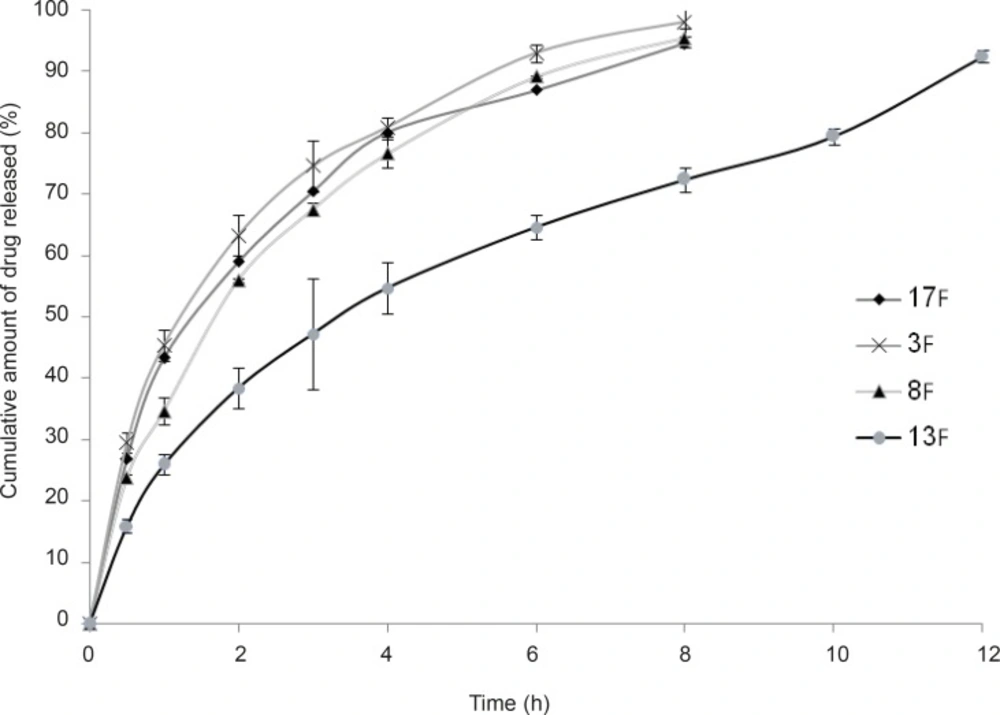
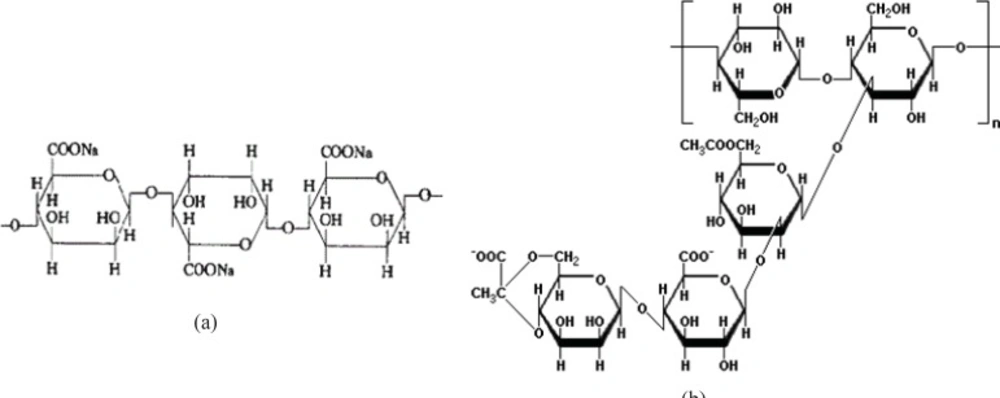
As stated in the previous section, propranolol HCl gel formulations F3, F8, F13 and F17 were chosen and their in-vitro drug release profiles were determined. The results obtained have been shown in Figure 5. As can be clearly observed in this figure, the drug release profile was slower from formulations containing anionic polymers such as formulations F13 and F8, which were contained of sodium alginate 6.5% w/w and xanthan gum 4% w/w, respectively. However, propranolol HCl gel formulation F13 released its drug content in a more retarded manner as compared to formulation F8. This observation may be attributable to the formation of ionic complexes (without affecting the gel structure) between propranolol HCl (a cationic drug) and sodium alginate (an anionic polymer). The chemical structures of sodium alginate and xanthan gum are shown in Figure 6. As it can be clearly seen in this figure, sodium alginate possesses more anionic carboxylate groups in its structure (there’s one carboxyl group on each of the monomers), while xanthan gum has only two carboxyl groups in the terminal side of its polymeric chain. Moreover, sodium alginate had been used in a higher concentration in formulation F13 (6.5% w/w) as compared to xanthan gum in formulation F8 (4.0% w/w). Hence, formation of greater drug-polymer complexes and subsequently a slower drug release pattern would be deducible from the F13 formulation. Formulations F3, F8 and F17 released nearly 100% of their drug contents over a period of 8 h, while propranolol HCl gel formulation F13 released more than 85% of its drug content throughout a 12 h period. As could be seen in release profile of this formulation (F13), a burst release occurred in the first 2 h after the drug release was initiated. In this case, burst release can be considered as a desirable phenomenon, since an initial burst is assumed to provide immediate contraceptive effects, through causing the propranolol HCl concentration exceeding its IC50 value (0.3 mM) followed by a prolonged release which maintains drug concentration above the IC50 value with the potential of promoting contraceptive efficacy for an extended period of time.
In-vitro release profiles of vagino-adhesive propranolol HCl gel formulations F3 ( Guar gum 3.0% w/w), F8 ( Xanthan gum 4.0% w/w), F13 ( Na alginate 6.5% w/w) and F17 ( HPMC 4000 4.5% w/w) at 37°C, citrate-phosphate buffer pH 4.5. Data are expressed as mean ± SD.
In-vitro drug release kinetic studies of the chosen formulations
Data obtained from
in-vitro drug release of the chosen propranolol HCl gel formulations F
3, F
8, F
13 and F
17 were fitted to various mathematical models including: zero order, first order, Higuchi and Korsemeyer-Peppas models. The drug release kinetic data for the above formulations are given in
Table 4. The model that best fitted the release data of each propranolol HCl gel formulation was evaluated by the highest regression coefficient (R
2).
Chemical structures of sodiom alginate (a) and xanthan gum (b).
The zero order kinetic model (Equation 2) describes systems where the drug release rate is independent of its concentration. In contrast, first order kinetic model (Equation 3) is indicative of systems where drug release is a concentration dependent process. Higuchi’s model (Equation 5) describes the release of drugs from an insoluble matrix as the square root of a time dependent process, based on Fickian diffusion. Korsemeyer-Peppas model (Equation 5) is applicable when diffusion is the main drug release mechanism, while relating the drug release exponentially to the elapsed time. Data obtained from release profile of formulation F3, fitted best into Korsemeyer-Peppas model with an R2 value of 0.9946, while the drug release profiles of formulations F8 and F17 could be explained by the first order kinetic model as their drug release data fitted best into this mathematical model (with R2 values of 0.9972 and 0.9895, respectively). In case of formulation F13, the best fit with the highest regression coefficient (R2 = 0.9955) was found to be with the Higuchi’s model.
By incorporating the first 60% of drug release data, mechanism of drug release can be peredicted using the Korsemeyer-Peppas model, where
n is the release exponent, indicative of mechanism of drug release. The values of release exponent (
n) for propranolol HCl gel formulations F
3, F
8, F
13 and F
17 were found to be 0.597, 0.614, 0.562 and 0.566, respectively. Hence, the mechanism of propranolol HCl release from all these formulations, would be based on anomalous (non-Fickian) diffusion (as described in
Table 2) which appears to indicate a coupling of diffusion and erosion mechanisms, so-called anomalous diffusion and may indicate that the drug release is controlled by more than one process (
20). In a previous study describing the release mechanism of domperidone from alginate-based beads, similar results were observed with
n values ranging from 0.485 to 0.771. They also considered the corresponding
n values to be indicative of anomalous release mechanism (
24).
Among the chosen formulations tested for determination of drug release profile, only propranolol HCl gel formulation F13 could release its drug content throughout a 12 h period and the release pattern of this formulation was the most desirable as compared to other formulations. It also revealed a good mucoadhesive strength (386.97 ± 9.31 mN). Hence, propranolol HCl gel formulation F13 was considered as the final formulation and underwent complementary studies including determination of drug content and assessment of the duration of mucoadhesion.
| Formulation code | Zero order
| First order
| Higuchi
| Korsemeyer-Peppas
|
|---|
| K0 (h-1) | R2 | K1 (h-1) | R2 | KH (h-1/2) | R2 | Release exponent (n) | R2 |
|---|
| F3 | 10.724 | 0.7995 | 0.470 | 0.9871 | 35.536 | 0.9704 | 0.597 | 0.9967 |
| F8 | 11.029 | 0.8564 | 0.380 | 0.9972 | 35.586 | 0.9856 | 0.614 | 0.9950 |
| F13 | 6.700 | 0.9107 | 0.180 | 0.9478 | 26.180 | 0.9955 | 0.562 | 0.9927 |
| F17 | 10.360 | 0.8044 | 0.340 | 0.9895 | 34.241 | 0.9712 | 0.566 | 0.9849 |
Determination of drug content within the final gel formulation
As there is no pharmacopeial monograph for vagino-adhesive proranolol HCl gel, the range of 90-110% of the claimed label which is applicable for most pharmaceutical dosage forms, was considered for drug content evaluation of the final gel formulation. The propranolol HCl content of this formulation (F13) was found to be 101.05% ± 0.106 (n = 3, mean ± SD) of the theoretical value (1.6% w/w), which complies with pharmacopeial specifications for drug content. Hence, it can be concluded that a proper method had been used for drug content analysis and the drug had been evenly distributed within the gel matrix.
Determination of the duration of mucoadhesion of the final formulation
As it had been stated in a previous study (
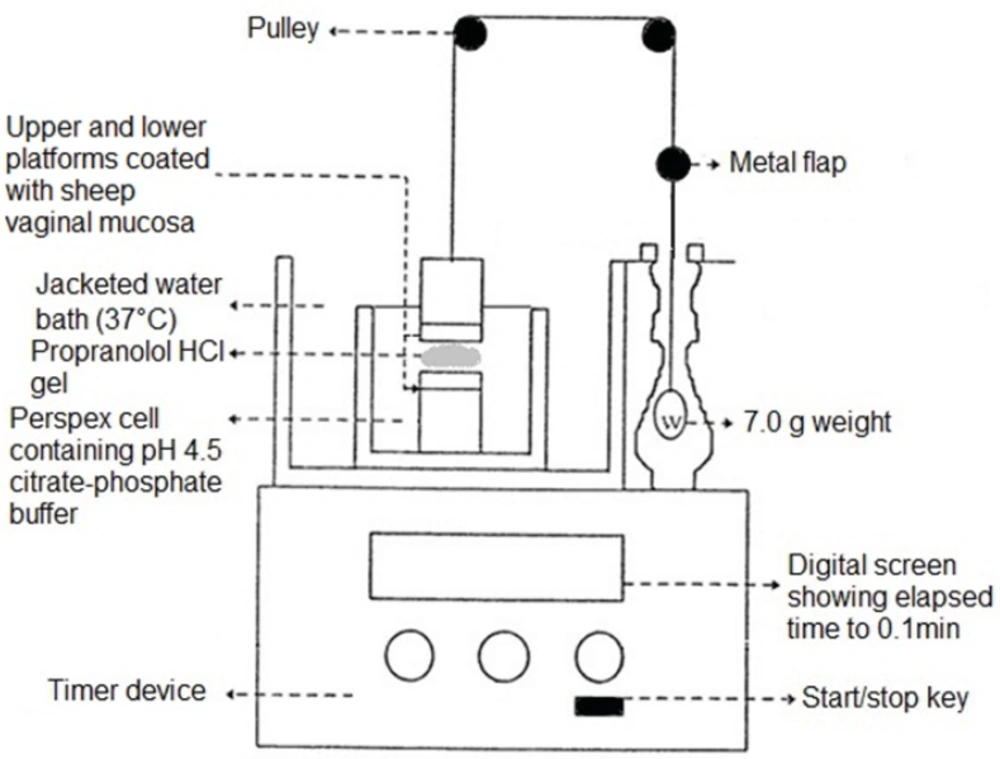
19), in most cases only the mucoadhesive strength of a newly formulated mucoadhesive system is evaluated, despite the fact that it is possible that a mucoadhesive system could initially adhere strongly to the mucosal surface but in long term it could quickly overhydrate and get displaced from the site of adhesion. Hence, investigating both these parameters is critical in the development of an effective mucoadhesive dosage form. In order to measure the duration of mucoadhesion of the final formulation (F
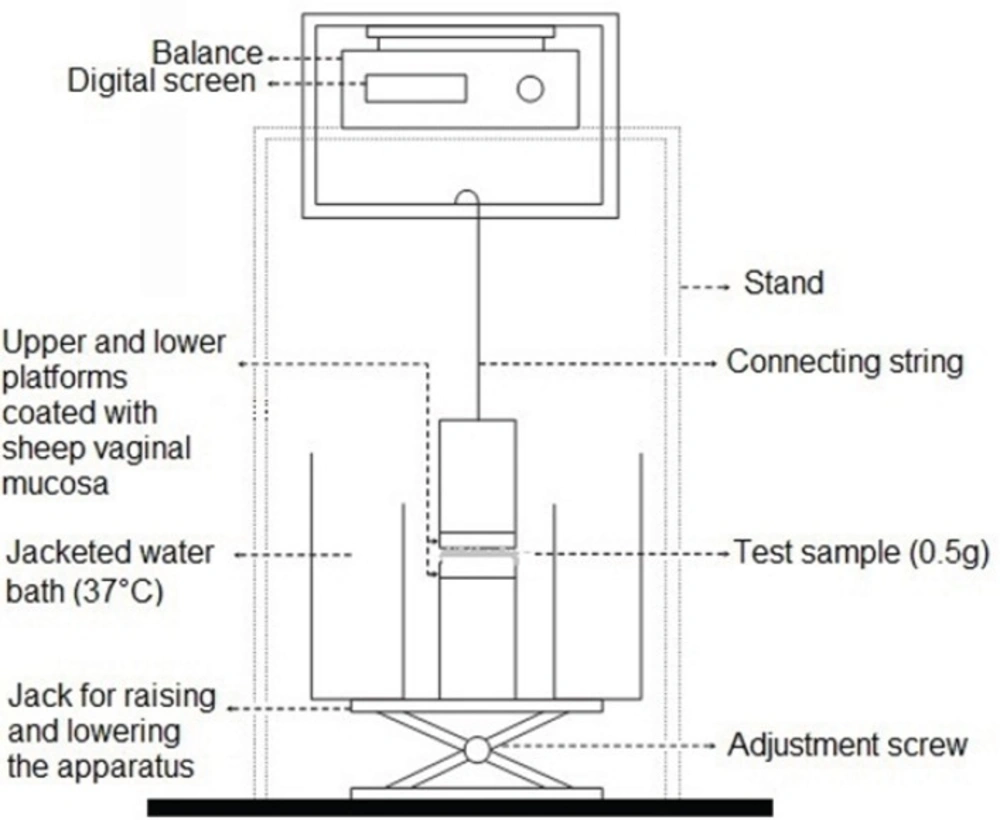
13), a 7.0 g weight was applied to the upper platforms of the apparatus shown in Figure 2. The results indicated that, by applying a maximum weight of 7.0 g, the gel could remain attached to the vaginal mucosa for more than 10 h. In this study the gel was fully immersed in an aqueous environment in order to prevent it from dryness and resembles the presence of vaginal secretions. However, this condition could result in a quicker hydration and faster disruption of the gel, in contrast to vaginal canal which contains less fluid. At the end, it should be noted that in both the evaluation of mucoadhesive strength and duration of mucoadhesion tests, separation of the gel from the mucosal surface appeared to be a result of a cohesive failure within the gel structure. Therefore, the mucosal surface was found to be coated with a rather thin layer of gel at the end of each test (
i.e. when gel mucosa separation took place). This finding would mean that in the
in-vivo condition, a thin layer of gel could still remain in contact with the vaginal mucosa, even after the main bulk of the gel applied has been washed away by vaginal secretions, prolonging the residence time of the gel and allowing further drug release from it.