This study was approved by the Clinical Research Ethics Committee, Shiraz University of Medical Sciences. All chemicals were purchased form Merck Chemical Company, with the best and purest grade available.
Subject recruitment
Human peripheral blood samples (20 mL) collected by venipuncture from 10 (mean age of 19 ± 8 years) G6PD-deficient and 10 healthy matched donors, with informed consents, were stored in adenine citrate dextrose at 4 °C. All analyses were carried out within 24 h.
G6PD screening
Qualitative screening of G6PD was carried out based on the Fairbanks and Klee method (
13). Blood samples obtained were centrifuged at 3000 rpm for 10 min at 22 °C, then they were washed three times with 0.9% w/v saline and centrifuged ( at 3000 rpm for 10 min) to obtain samples of constantly packed cells. Finally, erythrocyte suspensions (10% v/v) were prepared in pH 7.4 phosphate buffered saline (PBS).
Ten microliters of different blood samples were individually added to tubes containing 100 μl of a solution consisting of 50 mM glucose-6-phosphate, 7.5 mM NADP+, 0.5 g/dL saponin, 4 mM oxidized glutathione and 0.7 M of pH7.8 tris–HCl buffer. The blood samples were individually mixed and then 10 μL aliquots immediately transferred onto a 1×1 cm filter paper. After 5 min, this procedure was repeated. Spots were allowed to dry and then examined under a long-wave (320–400 nm) 150 W lamp. Florescence of specimens was compared with positive and negative controls.
The presence of Heinz bodies in freshly drawn blood samples were observed in order to approve G6PD deficient red blood cells after challenging with 0.1mg/mL α–naphthol.
Hb level and RBC count were also measured, using a DAX-48 autoanalyzer in all subjects.
Incubation of RBC suspension with H2O2and quercetin
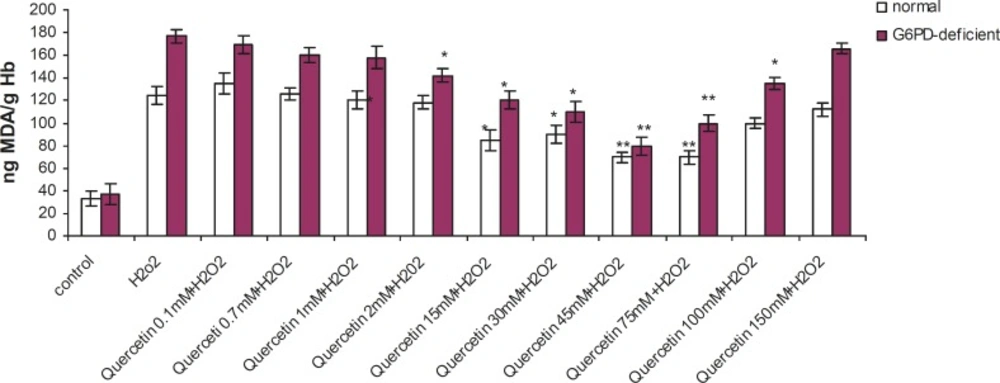
2.5 mL of the normal and G6PD-deficient erythrocyte suspension samples were treated with quercetin (0.1-150 mM) and vitamin C (250 mM) for 2h (1h before and 1h after incubation with 20 mM of H2O2) at 37 °C. After 1 h of H2O2 treatment, levels of TBA-reactive substances (TBARS) and GSH content were measured.
Determination of lipid peroxidation
The lipid peroxidation of red blood cell (RBC) membrane was assessed, as described by Stocks and Dormandy (
14). After a 2 h incubation period of erythrocytes with quercetin and vitamin C in the absence or presence of H
2O
2 (20 mM) at 37 °C, 0.5 mL of 25% TCA was added to 1 mL of suspension and the mixture was centrifuged at 1000 g for 5 min.
To 1 mL of the resulting supernatant, 1 mL of 1% thiobarbituric acid (TBA) in 0.05 M NaOH was added followed by boiling for 15 min. The formation of TBARS was used as a measure of lipid peroxidation. The TBARS concentration was determined using a spectrophotometer (BioTek Instruments, Winooski, VT, USA) at 532 nm and the results were expressed as ng MDA/g of haemoglobin.
Determination of GSH
Reduced glutation (GSH) was determined, based on the method of Ellman (
15). A 1 mL aliquot of the erythrocytes (0.5 mL of cells percipited by 2 mL of 5% TCA) was taken and 0.5 mL of Ellman’s reagent (0.0198% DTNB in 1% sodium citrate) and 3mL of phosphate buffer (pH 8.0) were added. The developed color was then read at 412 nm. The GSH concentrations in test samples were calculated, with reference to the standard curve of GSH (1–100 μg/mL). The results were expressed as μg/g of haemoglobin.
Statistical analysis
All the experiments were carried out at least in triplicate, using RBC from 10 subjects. Results were tested by one-way ANOVA, followed by usig the Dunnett post-hoc test. The difference between the G6PD-deficient and normal groups was analyzed by student’s t-test. All the statistical tests were carried out at a 5% level of significance (p < 0.05). Data obtained have been expressed as mean ± SD.