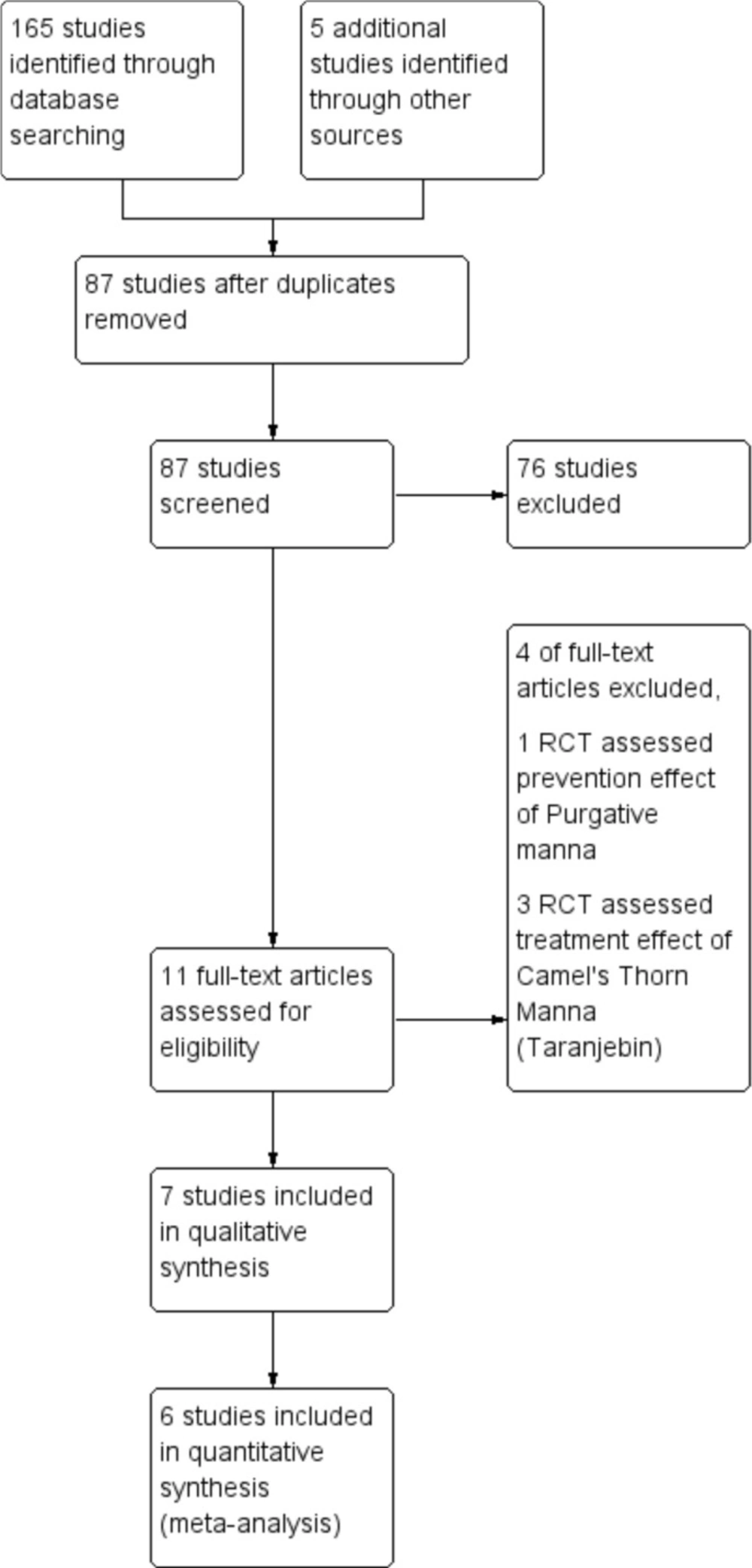
A total of 165 articles from different databases were identified. After reviewing the full text of articles, only seven clinical trials with 812 neonates met the inclusion criteria and were included in this review (
Figure 1). The languages of selected studies were in Persian (
16,
17 and
19) and English (
18,
20-
22).
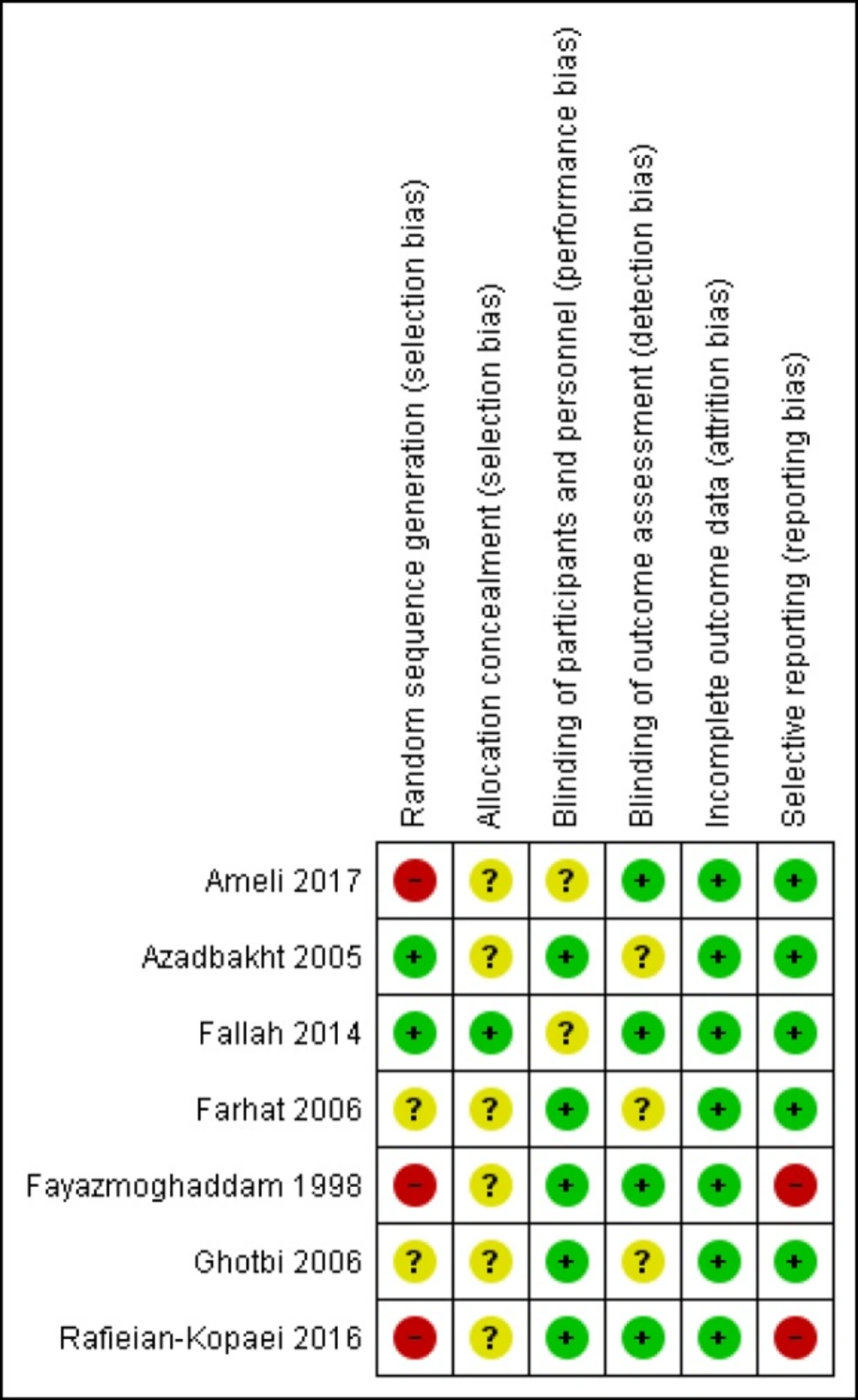
Risk of bias summary (Reviewers’ assessment of each risk of bias item; “+”, low risk of bias; “?”, unclear risk of bias; and “−”, high risk of bias)
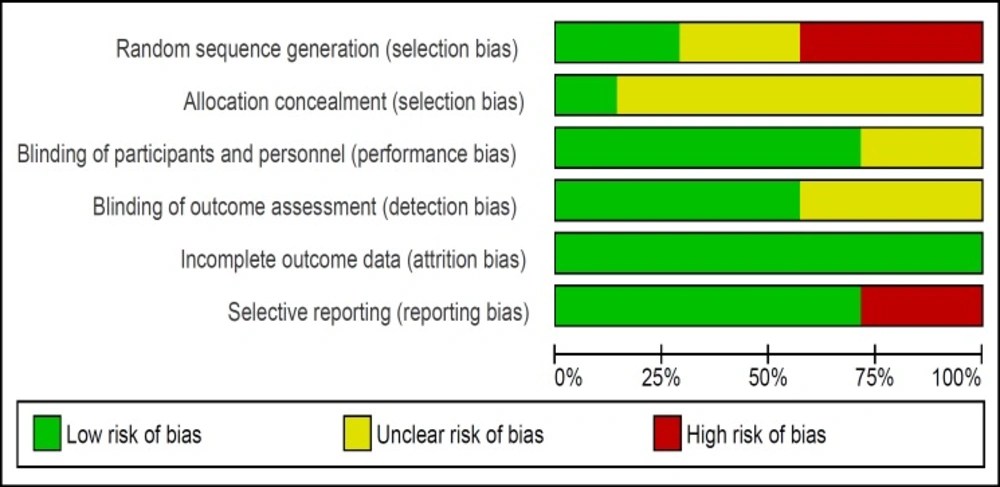
Risk of bias graph (Review authors' judgments about each risk of bias item presented as percentages across all included studies)
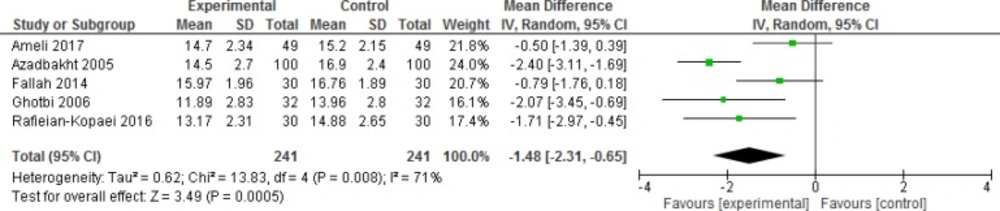
Comparison of bilirubin level at 12 h
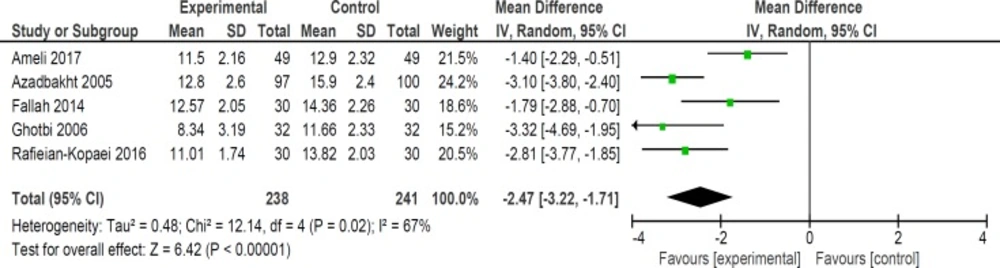
Comparison of bilirubin level at 24 h
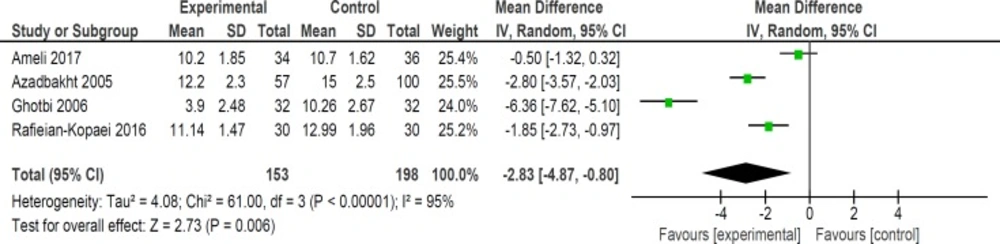
Comparison of bilirubin level at 36 h
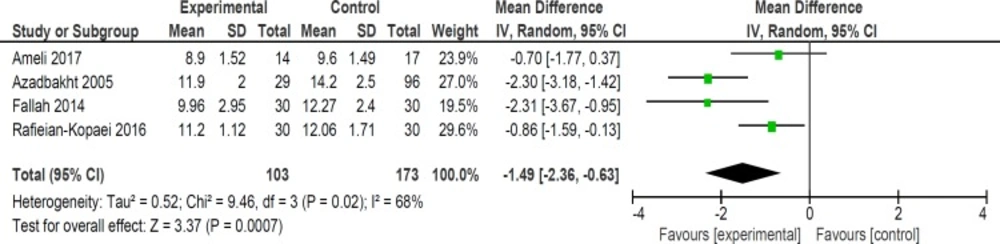
Comparison of bilirubin level at 48 h
Comparison of bilirubin level at 72 h
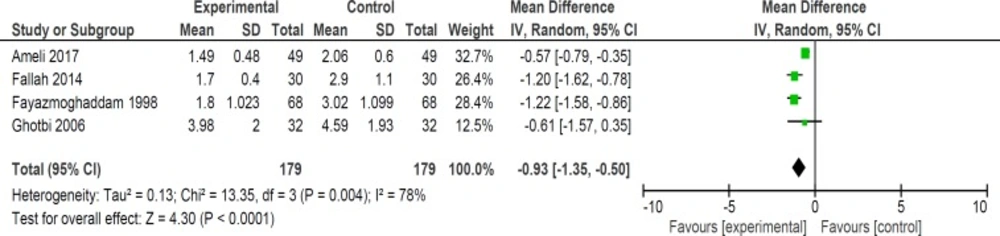
Comparison of length of hospital stay in days
| Author, year (reference) | Date and Location | Participants | TBS level on admission | Intervention | Purgative mannadose (mg) | Purgative manna source |
|---|
| Fayazmoghaddam, 1999 (16) | October 1998,Sanandaj, Iran | 136 neonates | Admission on 24 h to 72 h after birth:15-20 mg/dL Admission on more than 72 h after birth: ≥20 mg/dL | Intervention group (n = 68): Purgative manna three times a day+ phototherapy Control group (n = 68): water (placebo) three times a day + phototherapy | 666.67 mg purgative manna three times a day | Not reported |
| Azadbakht, 2005(17) | Iran | 200 neonates Full-term | Unclear | Intervention group (n = 100): 5 drop purgative manna three times a day + phototherapy Control group (n = 100):placebo drop three times a day+ phototherapy | 152.5 mg mannitol* threetimes a day | Manna of Cotoneaster discolor pojark from Qaien, Khorasan, Iran |
| Farhat, 2006 (18) | May 2001 toDecember 2003 Mashhad, Iran | 104 neonates Breastfed, more than 2500 g at birth | 18-29 mg/dl | Intervention group (n = 50): a single dose of 6 g of purgative manna dissolved into distilled water (8 mL) during the first hour of trial + phototherapy Control group(n = 54): a single dose of starch solution(0.1%, 8 mL)colored with one drop of caramel solution (placebo) + phototherapy | 6000 mg purgative manna for one dose | Manna of cotoneaster tricolor pojark from Qaien, Khorasan, Iran |
| Ghotbi, 2006 (19) | June 2003 toFebruary 2006, Iran | 64 neonates Full- term, Breastfed, 2500-4000 g atbirth,beginning of jaundice:3-11 days after birth | 15-20 mg/dL | Intervention group (n = 32): 10 cc purgative manna three times a day for the durationof one day + phototherapy control group (n = 32):distilled water (placebo) three times a day + phototherapy | 1666.67 mgpurgative mannathree times | Manna discolor from Khorasan |
| Author, year (reference) | Date and Location | Participants | TBS level on admission | Intervention | Purgative mannadose(mg) | Purgative manna source |
| Fallah, 2014 (20) | September 2012to February 2013 Yazd, Iran | 90 neonates Full-term, breastfed, 2500-4000g at birth, beginning of jaundice: 3-7 days after birth | 15-20 mg/dL | Intervention groups (n = 60):Thirty neonates were given 5 drop per kg Bilineaster
drop every 8 h up to 48 h + phototherapyThirty neonates
received half of glycerin suppository every 12 h up to 48 h + phototherapyControl group (n = 30):phototherapy | 75 mg/kg Mannitol* three times a day | Bilineaster drop from Sobhan Darou Company |
| Rafieian-Kopaei, 2016 (21) | 2010Shahrekord, Iran | 120 neonates Full-term, breastfed, 2500-4000g at birth, beginning of jaundice: 2 days after birth | 14-20 mg/dL | Intervention groups (n = 90):Thirty neonates were given 3 drop per kg Bilineaster
drop three times a day + phototherapy and their mothers were given dose of neonates × 3 Bilineaster dropThirty mother were given dose of neonates × 3 Blineaster drop Thirty neonates were given 3 drop per kg Bilineaster
drop three times a day + phototherapyControl group (n= 30): distilled water (placebo) three times a day+ phototherapy | Unidentified | Bilineaster drop from Barij Essence Pharmaceutical Company |
| Ameli, 2017 (22) | June 2015 toMarch 2016 Mashhad, Iran | 98 neonates Term(35-42 weeks), breastfed, more than 2000 g at birth, beginning of jaundice: 2-14 days after birth | More than17-20 mg/dL | Intervention group (n = 49): 5 drop per kg Bilineaster drop three times a day+ phototherapy Control group (n = 49):phototherapy | 75 mg/kg Mannitol* three times a day | Bilineaster drop from Sobhan Darou Company |
The main constituent of manna is mannitol of which it may contain from 40 to 60 percent.
| Author, year (reference) | Outcomes | Results | Side effects in intervention group |
|---|
| Fayazmoghaddam, 1999 (16) | Length of hospital stay | Length of hospital stay were lower in intervention group (p ≤ 0.001) | Not reported |
| Azadbakht, 2005 (17) | Bilirubin level, Length of hospital stay | Bilirubin levels were lower in intervention group at 12,24,36 and 72 h after treatment (p ≤ 0.05) Discharge of the intervention group from hospital started after 1.5 days of hospitalization. For the control group, the beginning of release from hospital was after2.5 days of hospitalization. | Small number of neonates developed listlessness caused by loss of water(as a result of osmotic diarrhea due to purgative manna or phototherapy) |
| Farhat, 2006 (18) | Bilirubin level, Defecation frequency | Bilirubin levels and defecation frequency of intervention group were not significantly different from control group | No side effects (follow up at 24 h afterphototherapy discontinued) |
| Ghotbi, 2006 (19) | Bilirubin level, Length of hospital stay, Defecation frequency | Bilirubin levels were lower in intervention group at12, 24 and 36 h after treatment (p ≤ 0.001) Length of hospital stay was lower in intervention group(p ≤ 0.001) Defecation frequency was significantly higher in intervention group (p ≤ 0.001) | Small number of neonates developed listlessness caused by loss of water(as a result of osmotic diarrhea due to purgative manna or phototherapy) |
| Fallah, 2014 (20) | Bilirubin level, Length of hospital stay, Defecation frequency | Bilirubin levels were lower at 24 h (p = 0.02) and 48 h (p = 0.02) after treatment inpurgative manna group Length of hospital stay was lower in purgative manna groupversus control group (p = 0.02) Defecation frequency was not significantly different between purgative manna group and control group | No side effects (during hospitalization and on the second day after dischargein the clinic of hospital, no side effects were seen in purgative manna group) |
| Rafieian-Kopaei, 2016 (21) | Bilirubin level, Length of hospital stay | Bilirubin levels were lower in intervention group at 12, 24 and 36 h after treatment (p ≤ 0.05) Length of hospitalstay was lower in intervention groups versus control group (p ≤ 0.001) | No side effects |
| Ameli, 2017 (22) | Bilirubin level, Length of hospital stay | Bilirubin levels were lower at 24 h (p < 0.001) after treatment in purgative manna group Length of hospital stay was lower in purgative manna group versus control group(p < 0.001) | No side effects(follow up one and two months after discharge by phone calls) |
The risk of bias of studies was evaluated by two authors. All seven trials were RCTs however three of them had used alternation as the method of randomization (
16,
21-
22) and only one study described the method of allocation concealment (
20). The risk of bias summary and graph of included studies are summarized in
Figures 2 and
3.
The dates of trials were from 1999 to 2017. Five of trials included only term infants (
17,
19-
22) and two of them included both term and preterm neonates (
16,
18).
Neonates in six trials received
purgative manna orally every eight hours. One of these six trials administered
manna for only one day (
19) and one trial administered
manna for 48 h (
20). In one study neonates just received
manna for a single oral dose during the first hour of hospital admission (
18). In addition, all neonates in the control and intervention groups of seven included trials received phototherapy on hospital admission and during hospitalization. The characteristics of included studies are presented in
Table 1.
The preparation methods of purgative manna solution for neonates in included studies were as follows:
Fayazmoghaddam
et al. dissolved one gram of
purgative manna into 30 mL water for 10 neonates every day (33.33 mg purgative
manna/mL). Afterwards, 20 cc of solution were administered to every neonate three times a day (
16).
Azadbakht
et al. obtained
manna from Khorasan, a province of north eastern Iran. They dissolved 400 g of
manna into 400 mL of distilled water and dried it under reduced pressure. Propyl paraben and methyl paraben were used as preservative. Finally, the dry extract had 88.3%
manna from which 50-60% was mannitol. One mL of the drop contained 610 mg active constituents based on mannitol (610 mg mannitol/mL). The neonates in intervention group received five drops of
purgative manna solution three times a day (
17).
Farhat
et al. collected
purgative manna from Khorasan. They dissolved six grams of
manna into distilled water (8 mL) for every neonate (750 mg
purgativemanna/mL) (
18).
Ghotbi
et al. gathered
purgative manna from Khorasan. They divided
manna to five gram packages. Every package was for administration to one neonate for one day. Five grams of
manna was dissolved into 30 mL boiling water every day (166.67 mg
purgativemanna/mL). Every neonate in intervention group received 10 mL of prepared solution three times a day for the duration of one day (
19).
Fallah
et al. (
20) and Ameli
et al. (
22) used Bilineaster drop from Sobhan Darou Company (300 mg mannitol/mL) and Rafieian-Kopaei
et al. (
21) used Bilineaster drop from Barij Essence Pharmaceutical Company.
In three trials, the number of neonates who needed exchange transfusion or Phenobarbital were reported. Azadbakht
et al. reported that three neonates in control group had exchange transfusion. In addition, Phenobarbital or
purgative manna was administered to four neonates in control group to manage jaundice. None of the neonates in intervention group needed exchange transfusion or Phenobarbital (
17). Furthermore, in Fallah
et al. study one neonate in each group of trial required exchange transfusion (
20). Ameli
et al. also reported that one neonate in
purgative manna group and five neonates in control group received Phenobarbital and eleven neonates in control group underwent phototherapy again after discharge for the management of their hyperbilirubinemia (
22). The obtained results of trials are summarized in
Table 2.
Meta-analysis findings
In meta- analysis, one study was not included because they administered
purgative manna only for one dose (
18) and the rest of studies administered
manna three times a day. Thus, the intervention was very different from the rest of studies. Three trials had more than one intervention group. As a result, among 708 neonates in included studies of meta-analysis, only 618 neonates were considered for analysis and 90 neonates in intervention groups other than
purgative manna were excluded.
Mean bilirubin level collected from neonates at 12 h after the start of intervention was lower for those allocated to
purgative manna and phototherapy than placebo and phototherapy (5 trials, 482 neonates) (WMD: -1.48, 95% CI: -2.31 into -0.65). Since WMD show reduction of bilirubin with 1.48 and CI does not contain zero, the intervention is statistically significant (
Figure 4). Similarly, five trials evaluating 479 neonates found significantly lower levels of neonatal bilirubin in
purgative manna group at 24 h after the start of intervention (WMD: -2.47, 95% CI: -3.22 to -1.71) (
Figure 5). At 36 h following intervention, four trials showed
purgative manna group had lower level of bilirubin versus control one (351 neonates) (WMD: -2.83, 95% CI: -4.87 to -0.80) (
Figure 6). In addition, four trials assessing neonatal bilirubin level at 48 h (276 neonates) (WMD: -1.49, 95% CI: -2.36 to -0.63) (
Figure 7) and at 72 h after the onset of intervention, (2 trials, 129 neonates) (WMD: -0.68, 95% CI: -1.28 to -0.08) showed lower levels of bilirubin in
purgativemanna group (
Figure 8).
Although six trials assessed the length of hospital stay in neonates but two of studies’ data were not available for quantitative analysis. In four studies, length of hospital stay was lower in
purgative manna group versus control group (358 neonates) (WMD: -0.93, 95% CI: -1.35 to -0.50) (
Figure 9) (
16,
19,
20 and
22).
Defecation frequency was another outcome that was considered in two trials. Ghotbi
et al. reported increasing number of defecation per day in intervention group (one trial) (64 neonates) (WMD: 0.71, 95% CI: 0.29 to 1.13) (
19). However, Fallah
et al. showed that number of defecation per day at 24 h (one trial) (60 neonates) (WMD: 0.65, 95% CI: -0.19 to 1.49) and 48 h (one trial) (60 neonates) (WMD: 1, 95% CI: 0.1 to 1.90) following intervention were not significantly different in both groups (
20).