



1. Background
In recent years, stuttering has been recognized as a common type of speech disorder in childhood and has been observed in at least 5% of all children (1). Common speech symptoms that present in stuttering are repetition, prolongation of sounds and syllables, pauses, filler words, and speech blocks (2). All of these symptoms may appear in a person who stutters at the same time, but with different frequencies. Most of the time, one symptom may be more prominent than the others and thus, the frequency of its manifestation would be the highest. Undoubtedly, identification and classification of stuttering symptoms can make a major contribution to both prognosis determination and the treatment process of stuttering (3). Although the higher the frequency of manifestation of each symptom, the longer the recovery and treatment process will be (4), these conditions will still differ depending on the type of symptom. For example, if repetition is the dominant symptom, the higher the frequency of its manifestation, the better the individual's prognosis for recovery (3).
On the other hand, bilingualism or multilingualism is very common in today's societies, and its prominent role in verbal communication problems has attracted the attention of many researchers (5-7). Most studies that have focused on the relationship between stuttering and bilingualism state that the probability of stuttering in bilingual children is higher while their chance for recovery is lower (6, 8-11). It has been reported that the prevalence of stuttering in bilinguals is about three or even four times higher than in monolinguals (12). Stuttering in bilingual children occurs at a younger age (13). Moreover, speech disfluency is more manifest while using the second language (14).
Particularly, stuttering manifests more during spontaneous speech and phone conversations in a second language (6). The occurrence of stuttering in the less fluent language of bilinguals is higher than in the language in which they have more profound proficiency or better fluency (15). For instance, the appearance of stuttering symptoms while using Spanish was higher in an English-Spanish bilingual person whose first language was English (9).
These unbalanced proficiencies in languages, to some extent, can be related to different levels of linguistic complexity between languages (interlanguage complexity) (16). The specific phonetic structures in each of the languages are one example of interlanguage complexity that can lead to differences in the performance of bilinguals (17).
Again, from this point of view, the motor control of the speech process may be different for each language. For example, in a comparison of the two languages English and Kannada, the speech motor process may be more unstable in English speakers. Herein, problems in English are more evident in English-Canadian bilingual children with stuttering (16). Therefore, the appearance of disfluency symptoms in each of their two languages will be different.
On the other hand, inconsistency in the process of speech motor control in people who stutter may lead to the occurrence of some involuntary psychomotor behaviors in their face and limbs during speech production (18-21). Thus, concurrent with the manifestation of verbal symptoms of stuttering (such as repetition, blocks, etc.), some extra irrelevant gestures like physical tension may also be seen (22), which are usually known as secondary behaviors or nonverbal stuttering symptoms.
In continuation of these topics, some environmental factors such as the extent to which each of these languages is used in daily life are effective and should be considered too (7). Sometimes, the use of languages during daily life follows socio-cultural habits. In this regard, it should be noted that Iran has been a multilingual country throughout history and in addition to Persian as the official language, many native languages like Kurdish, Balochi, Azari, Arabic, Gilaki, etc., have been prevalent there too. Although Persian is the language used for education and correspondence, most people usually speak their native languages in informal situations. Herein, the native and/or first language (L1) of people in some western cities of Iran like Kermanshah is Kurdish, and Persian, as the official language of the country, is their second language (L2). So, they are known as Kurdish-Persian bilingual speakers and, since children learn the official language in kindergartens and schools, they are able to speak both languages from childhood. Indeed, due to the existence of such conditions, in some Iranian multilingual families, parents, even at home, insist on speaking to their child in Persian (23). Such a cultural habit is seen among families in Kermanshah too. Overall, insisting on such behaviors can bring consequences and difficulties for children who stutter.
Regardless of the factors mentioned above, the appearance of stuttering can be different based on sex and age groups (24, 25). The prevalence of stuttering is higher in boys than in girls (25, 26). The boy-to-girl ratio in terms of age groups is reported to be 2.3 to 1 at 2 to 5 years of age, 3.3 to 1 at 6 years of age, and 4 to 1 at 11 to 20 years of age (26). On the contrary, the occurrence of stuttering among students decreases with age (27).
According to the above, various factors are involved both in the development of language proficiencies between the two languages of bilinguals and in the manifestation of stuttering symptoms. However, it is not yet clear how effective each of these factors is. Undoubtedly, more studies in different languages are still needed to answer this question more precisely.
2. Objectives
Consequently, this study aimed to investigate the symptoms of stuttering between the two languages used in Kurdish-Persian bilingual children and teenagers who stutter. The output of this research, in addition to confirming or rejecting the role of some mentioned factors, can also be effective in providing suggested strategies for the evaluation and treatment of bilingual people who stutter.
3. Methods
3.1. Participants
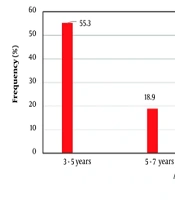
In this cross-sectional study, 360 Kurdish-Persian bilingual children and adolescents who stutter were selected by convenience sampling from all referrals to the speech therapy unit of Dr. Mohammad Kermanshahi Pediatric Specialty Hospital over two years. In this study, the symptoms of stuttering were compared between the two languages, both in terms of the frequency of occurrence of each symptom separately and in terms of the frequency of occurrence of all symptoms generally, in a group of bilingual people who stutter with Kurdish as their first language and Persian as their second language. In addition, the co-occurrence of secondary stuttering behaviors was also compared between the two languages. The age of onset of stuttering in all individuals was between 3 and 7 years, and while individuals could speak Kurdish at home, they also had to be able to communicate in Persian at the first clinic session. Conversely, based on our exclusion criteria, monolingual individuals or individuals with developmental language disorder (DLD), hearing impairments (HI), or learning disabilities (LD), as well as referrals whose age of stuttering onset was after 7 years, were excluded from the study. Therefore, although the total number of stuttering referrals during the two years of the present study was 451 children and adolescents, only 360 of them were included in the study based on the criteria mentioned above. Children were classified into age groups of 3 to 5 years, 5 to 7 years, 7 to 12 years, and 12 to 18 years (adolescents), of which children aged 3 to 5 years had the highest number of participants with 55.3% and adolescents had the lowest number with 11.9% among all subjects (Figure 1). In addition, 73.3% of the subjects were boys and 26.7% were girls (Figure 2).

Figure 1.
The frequency distribution of subjects based on age

Figure 2.
The frequency distribution of subjects based on gender
3.2. Tools
The performance of subjects in speech production was evaluated, both with Kurdish and with Persian languages separately, via three informal tasks as follows: (A) oral descriptive speech, (B) the picture description task with a single event, and (C) the picture description task with multiple relevant events.
3.3. Procedure
Each of the subjects was evaluated in three sessions. The duration of each session was 45 minutes. In the first session, we concentrated on gathering demographic information and taking history. In younger subjects, some of these data were collected through interviews with their parents. Also in the first session, while creating and establishing communication with the subjects, they were selected based on the inclusion and exclusion criteria, and that was how they were entered into the next two sessions. These evaluative sessions were held consecutively over two weeks for each language separately, and all data were gathered by the speech therapist.
In the implementation of the oral descriptive speech task, two simple topics were presented to the subjects and then we asked them to describe each topic with two to three sentences. Also, the single event tasks of picture description were implemented by six different picture cards in which the subjects were asked to describe each one orally. In the multi-event tasks of picture description, three separate picture cards were presented to the subjects for oral description.
In the picture description tasks, each of the picture cards was first placed in front of the subjects, and they were then asked, "What do you see in this picture?"
To summarize the implementation of this research, some points should be mentioned:
- Before starting each step, the examiner first answered a task as an example.
- In each of the tasks, up to two minutes were given to start answering, and in case of no answer, the next item was presented.
- The age groups of the subjects were considered in designing and selecting the topics for the tasks.
- All these steps were performed in Kurdish in one session and were repeated for evaluation with Persian in another session too.
Informed consent was obtained from all the participants who were enrolled in the research, either from the subjects or their parents.
3.4. Scoring and Analysis
The utterances were recorded throughout the sessions. In order to determine the frequency of each stuttering symptom (i.e., block, pause, repetition, prolongation, and filler), the recorded utterances were analyzed. After determining how much each of these symptoms was manifested among the subjects, the symptoms were arranged from the most frequent to the least frequent in each of the two languages separately, and then, the more frequent symptoms among the subjects were identified and compared between the two languages. In the following, the average frequency for all of these symptoms was compared between the two languages too. These averages in each subject are obtained by calculating the ratio of all stuttering symptoms to all words uttered. Then, the results were divided into low, moderate, and high levels for each language separately. So, if the ratio of all stuttered items to the total number of words uttered in each subject was less than 25%, the frequency of stuttering was at a low level; if the ratio was between 25% to 50%, it was at a moderate level; and ratios greater than 50% were categorized as a high level. Throughout the evaluation sessions, the secondary behaviors of stuttering, while using each of the two languages, if observed, were recorded.
All stages of the study, from gathering demographic information and taking history to implementation of the tasks and extracting data, were done by a speech therapist fluent in Kurdish and Farsi languages. In order to determine the inter-examiner reliability, another speech therapist who was an expert in two languages was also present at all stages. The inter-examiner reliability was calculated by the 95% confidence interval and intra-class correlation coefficient (ICC). The extracted ICC was 0.81 (0.79 - 0.89).
In this study, all statistical analyses were performed using SPSS software version 24. A significance level of (P < 0.05) was considered. Also, the chi-square test was used to compare the performance of subjects between the two languages.
4. Results
The results showed that the manifestation of two symptoms, block and repetition, had the highest frequency in more than 70% of the subjects, both in speaking with Persian and Kurdish languages. The average frequency percentage for manifestation of each stuttering symptom, among all of the subjects when evaluated with Kurdish tasks, was 47.8% for block, 26.1% for repetition, 15.9% for pause, 6.1% for prolongation, and 4.1% for filler. Instead, the average frequency percentage for manifestation of each stuttering symptom during Persian tasks was 39.2% for block, 34.4% for repetition, 5% for pause, 11.9% for prolongation, and 9.5% for filler. Furthermore, a comparison of the frequency of each symptom between the two languages indicated a significant difference (P < 0.05, Table 1).
Table 1.Comparison of the Frequency of Each Stuttering Symptom Among Subjects When Evaluated with Both Kurdish and Persian Tasks a
| Sign Types | Kurdish Language | Persian Language | Chi-square Test | P-Value |
|---|---|---|---|---|
| Blocks | 172 (47.8) | 141 (39.2) | 52.220 | < 0.05 |
| Repetition | 94 (26.1) | 124 (34.4) | ||
| Pause | 57 (15.9) | 18 (5) | ||
| Prolongation | 22 (6.1) | 43 (11.9) | ||
| Filler | 15 (4.1) | 34 (9.5) |
a Values are expressed as No. (%).
The findings also showed that the overall frequency level of the symptoms of stuttering while using the Kurdish language was low in 45.3% of the subjects, moderate in 36.4% of the subjects, and high in 18.3% of the subjects. On the other hand, the frequency level of total symptoms while using the Persian language was low in 20.3% of the subjects, moderate in 56.1% of the subjects, and high in 23.6% of the subjects. A comparison of these results using the chi-square test showed a significant difference between them (P < 0.05, Table 2).
Table 2.Comparison of the Average Frequency of All Stuttering Symptoms Between Two Languages a
| The Average Frequencies of All Stuttering Symptoms | Kurdish Language | Persian Language | Chi-square Test | P-Value |
|---|---|---|---|---|
| Low (below 25%) | 163 (45.3) | 73 (20.3) | 51.851 | < 0.05 |
| Moderate (25% - 50%) | 131 (36.4) | 202 (56.1) | ||
| High (more than 50%) | 66 (18.3) | 85 (23.6) |
a Values are expressed as No. (%).
In this study, the frequency for co-occurrence of secondary behaviors of stuttering in the subjects was 13.9% while using the first language (Kurdish language) and 35.8% while using the second language (Persian language). The difference in symptoms between the two languages was significant based on the chi-square test (P < 0.05, Table 3).
Table 3.Comparison of the Occurrence of Secondary Behaviors When the Subjects Spoke with Each of Kurdish and Persian Languages a
| Secondary Behaviors in Subjects | Kurdish Language | Persian Language | Chi-square Test | P-Value |
|---|---|---|---|---|
| Yes | 50 (13.9) | 129 (35.8) | 46.40 | < 0.05 |
| No | 309 (85.8) | 230 (63.9) |
a Values are expressed as No. (%).
5. Discussion
As stuttering is affected by several different factors, its manifestation may be variable among people who stutter, especially in comparison between two groups of bilinguals and monolinguals. For this reason, by limiting the comparison to evidence between two languages in one bilingual group with the same speakers, in the present study, an appropriate and minimal solution was tried to control some intergroup confounding factors.
Therefore, in this study, the types of stuttering symptoms including repetition, prolongation, blocks, filler, and pauses were compared in two languages, Kurdish and Persian, in terms of the frequency of manifestation of each symptom separately, and also the frequency level of all symptoms together. Moreover, the use of secondary behaviors of stuttering in the subjects when using each language was compared too. In the following, the differences and similarities of symptoms in two languages are discussed considering the influencing factors mentioned before.
As gender (sex) and age groups were the usual factors considered in most studies, our results in this regard showed that the proportion of stuttering in boys was nearly three times that of girls. This was consistent with the results of Choo and Smith (13) that, like monolingual ones, more boys than girls have been reported among bilingual children who stutter too. In the past few decades, this difference had been attributed to the type of separate expectations in traditional societies regarding girls and boys, or even in recent years has been ascribed to different socialization of gender roles. Although the process of socialization in children starts from about 3 years old, in fact, their gender roles gradually diverge from the middle of childhood. It is reminded here that more than 50% of the subjects in our study were children in the age range of 3 to 5 years and also, the subjects for some similar studies where the proportion of boys who stutter was more than that of girls, were in the pre-school age range. Therefore, the above justification is not completely accepted and on the contrary, we guess that maybe the lower proportion of stuttering in girls relates to their better language competence than boys.
The findings of this study for comparison of stuttering symptoms among bilinguals showed that block and repetition were respectively the most frequent symptoms in both languages. Moreover, for more than 70% of the subjects, both of these two symptoms together had the highest frequency in each of the languages. Consistent with this finding, some researchers have introduced block, repetition, and also physical tension as the common symptoms among people who stutter (28). In all, it can be argued that block and repetition are the most dominant symptoms in most bilingual and even monolingual people who stutter.
The comparison of symptoms between two languages in this study indicated that when using L1, block and pause were the most frequent symptoms among the subjects, whereas the frequency of symptoms of repetition, prolongation, and filler was higher during speech with L2. Also, Howell et al. have provided consistent evidence for such a difference, albeit only for L2 (the frequency of block and pause was higher while using L2) and suggested the existence of differences in phonetic structures as its reason (16).
Likewise, Fiestas et al. stated that the higher frequency of repetition as a dominant symptom in L2 can be the result of linguistic uncertainty in phonology and lexical levels, stressing the word, phonetic structures, and word length (28). Some other studies have only pointed to the effect of cross-linguistic phonological complexity as the cause of these differences (6, 29). Also, Another study argued that the greater appearance of some symptoms in one of the two languages is due to more complex phonological features in that language.
For the majority of the subjects in this study, the frequency of manifestation of all stuttering symptoms together was significantly higher in L2 than in L1. Although this finding was consistent with the results of Mohammadi et al. (27), it was inconsistent with the results of studies by Howell et al. that conversely declared the frequency of the stuttering symptoms was higher in the second language (16).
This difference is attributed by some studies to the unbalanced proficiency of languages. Poor proficiency in a language can lead to speech non-fluency, which is manifested by a higher frequency of stuttering symptoms (30). The results of a study by Ardila et al. (9) showed that the occurrence of stuttering symptoms in an English-Spanish bilingual person was higher in the second language. According to Schafer and Robb (4), the occurrence of stuttering is higher in the less fluent language of bilinguals. Byrd et al. argued that a higher frequency of stuttering symptoms in one of the two languages can be due to less practice with that language (15).
But, this difference can only to some extent be related to unbalanced proficiency of languages, because, in addition to this, parents in many bilingual societies in Iran, as mentioned before, insist on speaking with their children in the formal language especially when their child gets older to about school age. Such socio-cultural behaviors can bring more stress and negative experiences for bilingual children, particularly for those who stutter, and therefore may lead to a greater manifestation of stuttering symptoms, especially in the second language.
Lastly, our results indicated the occurrence of a small percentage of secondary behaviors of stuttering among the subjects while using each of the two languages. Even in this condition, the frequency of these secondary behaviors among the subjects was significantly higher in L2 than in L1 during the assessment sessions.
With a more detailed analysis of the data, we found that the manifestation of these non-speech symptoms was less among children aged 3 to 5 years, which included most of the subjects. Therefore, this may be the reason why a small percentage of secondary behaviors were reported among the subjects in this study.
So, these symptoms were mostly observed among the subjects with older age. Such a phenomenon can be the result of anxiety at the same time as stuttering, which appears as abnormal body movements (31). Accordingly, it could be suggested that the older the children are, not only are they more aware of their stuttering, but at the same time, their anxiety also increases. Moreover, since the bilingual subjects in this study were less fluent in L2, the anxiety of attending school in older children causes more non-speech symptoms in them along with L2, too.
To sum up, these justifications are somewhat in line with the results of a study by Kashyap and Maruthi who compared the symptoms between English and Kannada. They stated that English seems to have a relatively more unstable motor speech system (6). Poor motor-speech planning in people who stutter leads to more manifestations of both symptoms of stuttering and secondary behaviors accompanying it. Moreover, another study has pointed to the diversity of interlanguage complexity and different motor systems of these languages during speech production (16).
5.1. Conclusions
According to the results of this study, it seems that the greater occurrence of stuttering in boys than in girls may be related to an intrinsic factor such as girls' better language skills rather than to environmental and socio-cultural factors. As far as the symptoms of stuttering were more manifested in L2, it can be relevant to unbalanced development of language proficiency between two languages due to incongruity in some socio-cultural habits, and the predominant presence of a few other symptoms in L1 may relate to the complexity of its specific linguistic features. It is concluded that while the stuttering symptoms may be manifested with different frequencies in one language, also due to the existence of some interlanguage and/or environmental factors, the frequency of manifestation of each symptom can be different even between two languages of the same bilingual speakers. As a clinical conclusion, for bilingual people who stutter who refer to speech therapy, it is suggested that separate assessment and intervention programs be considered in each language. Moreover, as the secondary behaviors of stuttering occurred more while using the second language, it is recommended that future studies consider the relationship between secondary behaviors and an intrinsic factor like the level of anxiety in bilingual people who stutter.
5.2. Limitations
This study had limitations that should be considered when interpreting the results. These limitations include convenience sampling, which may limit the generalizability of the results to other populations. Therefore, it is suggested that random sampling be used to reduce selection bias. The cross-sectional design of the study does not allow for the investigation of causal relationships between internet addiction and social health. Longitudinal studies can investigate long-term changes in this relationship. This study was limited to one hospital, which limits the generalizability of the results.
