



1. Context
Chronic pain is defined as pain that lasts longer than the normal recovery time and usually persists for over three to six months (1). Back pain is considered the most common type of chronic pain and has been the dominant cause of disability worldwide for more than two decades (1). Back pain plays a significant role in increased healthcare needs, has a huge impact on healthcare systems, and predominantly affects adults. Hence, it can greatly influence healthcare costs and the national economy (2-4). The annual incidence of this disease in adults is estimated to be between 10 and 15% worldwide, and its 3-month prevalence in the United States is reported to be 31%, highlighting the commonness of this condition. Factors associated with back pain include age, chronic disease, comorbidities, obesity, a sedentary lifestyle, as well as environmental factors such as lifting heavy objects and improper work ergonomics (3). Back pain can result in a reduced quality of life, prolonged disability, and severe effects on work efficiency and work absenteeism (5). Indeed, health-related quality of life (HRQL) is affected by chronic back pain in different areas of life, such as physical and mental health, social relationships, and functional ability (1).
The use of sedatives, narcotic analgesics, non-steroidal anti-inflammatory drugs, and muscle relaxants is common in back pain management, but these are associated with many complications (6-8). For this reason, in recent years, non-pharmacological methods have been receiving more attention from researchers and medical staff for treating chronic back pain (9, 10). Among these methods is traditional medicine. Traditional medicine is used to prevent, diagnose, and treat physical and mental diseases and maintain overall health. In East Asian countries, approximately 80% of the population depends on traditional medicine for primary healthcare needs, and 70 - 80% of the population in developed countries use alternative or complementary treatments (11). The most common traditional medicine treatments for back pain include acupuncture and massage. Massage therapy enhances local blood flow and oxygen supply to muscles and affects nerve activity at the segmental level of the spinal cord, thus influencing pain. Researchers believe acupuncture stimulates the central nervous system, triggering the release of various chemicals in the body. These chemicals, such as endorphins, serotonin, and acetylcholine, can help reduce back pain and promote relaxation (12). Consequently, we can assume that, in general, these methods may reduce the use of medical and surgical interventions. However, more research is needed to understand the effectiveness of different treatment approaches in traditional medicine. Given the potential therapeutic effects of different traditional medicine treatments on common back pain conditions, it is optimal to investigate the efficacy of traditional interventions as affordable treatments with low side effects for patients suffering from back pain.
2. Objectives
The present study aimed to systematically review the existing evidence regarding the use of traditional medicine interventions for chronic back pain.
3. Methods
3.1. Protocol and Approval
A systematic review was conducted to identify studies that used traditional medicine interventions for back pain treatment. This systematic review was in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines (13). The PRISMA statement was developed to provide guidelines for reporting the outcomes of systematic reviews and meta-analyses. It is primarily focused on the reporting of reviews evaluating the effects of interventions and consists of a 27-item checklist that outlines the sections/topics to be included in a systematic review. In addition, it includes a flow diagram, which provides a visual overview of the different stages of the systematic review, including the identification, screening, and inclusion (and exclusion) of studies. Prior to conducting the preliminary searches, we received proposal approval from the Ethics Committee of Shahrekord University of Medical Sciences for this systematic review (IR.SKUMS.REC.1401.214).
3.2. Selection Criteria
We included studies of any therapeutic intervention if they involved traditional medicine aimed at the treatment and reduction of chronic back pain compared with a control group (treatment as usual or routine care/waiting list), or other interventions and treatments for back pain. We included studies in this systematic review if they were written in English or Persian and consisted of adult participants (aged 18 and over). Published studies were eligible if they were published in peer-reviewed journals. We included studies if participants were diagnosed with a back pain condition using validated measures at pre-treatment and received traditional medicine intervention for the back pain condition. We did not apply any restrictions on the severity of back pain symptoms. Two reviewers (MGA and SS) completed title/abstract screening and full-text screenings independently, and there was no discrepancy about whether a paper was eligible for the present study.
3.3. Search Strategy
3.3.1. Search Methods for Identification of Studies
We conducted an advanced search in Web of Science, Scopus, ProQuest, PubMed, and Iranian databases such as Rondo, Magiran, and SID up to February 2023. We applied filters to exclude animal studies and articles considered as secondary studies. We included specific controlled vocabulary terms [medical subject headings (MeSH)] with specific free-text words related to back pain and traditional medicine (Table 1). For Iranian databases (Rondo, Magiran, and SID), a manual search was conducted using both English and Persian terms, including "back pain", "traditional medicine", and "intervention", to ensure comprehensive coverage of relevant studies. The searches were independently peer-reviewed by a researcher using the peer review of electronic search strategies (PRESS) checklist (14).
Table 1.Search Strategies in Databases
| Database | Search Strategy |
|---|---|
| PubMed | (["Back Pain, Backache"(MeSH) OR "Back Ache"(Tiab) OR Vertebrogenic Pain Syndrome (Tiab)] AND ["Traditional Medicine"(MeSH) OR "Primitive Medicine"(Tiab) OR Folk Medicine (Tiab) OR "Ethnomedicine"(MeSH) OR "Home Remedi "(Tiab)] AND (therapy* OR treatment * OR therapy OR therapies OR therapeutic* OR treat* OR interven*) AND ([English(lang)]) |
| Scopus | [TITLE-ABS-KEY ("Back Pain" OR "Backache" OR "Vertebrogenic Pain Syndrome") AND TITLE-ABS-KEY ("Traditional Medicine" OR "Folk Remedi" OR "Primitive Medicine" OR "Home Remedi" OR "Indigenous Medicine" OR "Ethnomedicine") AND TITLE-ABS-KEY ("treatment" OR "therapy" OR "intervene")] |
| Web of Science | (Back Pain * OR Backache * OR Back Ache * OR Vertebrogenic Pain Syndrome*) AND (Traditional Medicine* OR Folk Remedi OR Primitive Medicine OR Indigenous Medicine OR Home Remedi OR Ethnomedicine) (in Title or Topic) |
| ProQuest | Ab (Back Pain * OR Backache* OR Vertebrogenic Pain Syndrome*) AND ab (Traditional Medicine* OR Folk Remedi OR Primitive Medicine OR Indigenous Medicine OR Home Remedi OR Ethnomedicine) AND (treatment*) |
| Iranian databases (Rondo, Magiran, and SID) | Manual search in English and Persian using terms: (Back pain), (traditional medicine), (intervention) |
Abbreviation: MeSH, medical subject heading.
3.3.2. Data Extraction
Two reviewers (MGA and SS) performed data extraction independently using the same data extraction forms, and disagreements in data extraction were resolved through discussion with a third author (FA). We contacted study authors in case there was missing data and if any clarification was needed. We used a standardized data collection form to extract pre-arranged data, including the first author, publication year, country of origin, condition, target population, sample size, measurement of back pain, interventions, outcome, efficacy, duration, and adverse effects.
3.4. Risk of Bias
We aimed to carefully consider the potential limitations of the included studies and used the Cochrane Collaboration’s tool to assess the risk of bias (15). We explicitly evaluated the risk of selection, performance, detection, extent of loss to follow-up, reporting, and other biases (e.g., imbalance in baseline characteristics).
4. Results
4.1. Search Results
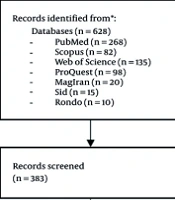
We identified a total of 628 studies from multiple databases, including Web of Science, Scopus, ProQuest, PubMed, and Iranian databases such as Rondo, Magiran, and SID, using the search strategy. After the removal of 523 studies and excluding those clearly not relevant, we assessed the potential studies for full-text eligibility. Out of 105 studies assessed for eligibility, 97 studies were excluded, mostly because they were review articles (n = 65), conference papers (n = 10), case studies (n = 17), and animal studies (n = 5). Based on the selection criteria, 8 studies relating to the use of traditional medicine for patients with back pain were included in this systematic review (16-23). Figure 1 presents the process of study selection in the PRISMA flow chart.
 flow diagram")
Figure 1.
Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram
4.2. Setting and Design
The eight included randomized controlled trials (RCTs) were conducted across diverse clinical and community healthcare settings in Asia, Europe, and Australia. Geographically, studies originated from Iran (16), Taiwan (17), Germany (23), Australia (19), Thailand (20), and mainland China (18, 21, 22). The time frame for publication spanned from 2010 to 2022. Most studies employed parallel-group RCT designs, with random allocation to treatment and control groups. Five trials utilized single- or double-blind methodologies — particularly those involving sham acupuncture or placebo ointments (17, 23) — to reduce performance and detection bias. The remaining three trials (19, 20, 22) operated as open-label or assessor-blinded studies, where blinding of participants was not feasible due to the nature of the interventions (e.g., physical therapy or exercise regimens). Sample sizes ranged from 44 to 160 participants, and the duration of the interventions varied from two weeks (23) to 12 weeks (17, 19), with follow-up assessments extending up to six months in certain trials (19, 21). Across studies, the control conditions included conventional treatments (physiotherapy, NSAIDs), placebo treatments (e.g., sham acupuncture, inert ointments), or waitlist controls, allowing for comparisons across a wide spectrum of standard care versus complementary techniques.
4.3. Participants
Across the eight RCTs, a total of 729 participants were enrolled, with individual study sample sizes ranging from 44 to 160. All participants were adults diagnosed with chronic or acute low back pain (LBP), with most studies focusing on chronic non-specific LBP lasting more than 3 months. Namiranian et al. recruited 90 patients aged 20 - 60 years with chronic LBP of at least 3 months’ duration. Participants were randomly assigned to Fateh massage, acupuncture, or physiotherapy groups (16). Yeh et al. included 80 participants (mean age ~ 45 years) with chronic LBP for more than 3 months. Participants were randomized to receive electronic acupuncture shoes or sham devices (17). Saha et al. enrolled 60 adults with chronic LBP, defined as pain persisting for more than 12 weeks. Participants were randomized to receive Gua Sha therapy or control treatment (18). Hall et al. studied 160 individuals aged 18 - 70 years with persistent non-specific LBP. Participants were randomized to Tai Chi or waitlist control groups (19). Buttagat et al. included 44 participants with chronic non-specific LBP aged 20 - 60 years. All participants had pain for more than 3 months and were randomized to Thai self-massage with stretching or control (20). Luo et al. recruited 72 patients with chronic LBP, aged 18 - 65 years, and randomly assigned them to hand-ear acupuncture or usual care (21). Tang et al. enrolled 82 participants with lumbar degenerative instability and chronic LBP. Participants were randomized to Tuina with or without core stability exercises (22). Giannetti et al. studied 141 patients with acute upper or lower back pain, aged 18 - 60 years, randomized to comfrey root extract ointment or placebo (23).
4.4. Assessment
Pain intensity was the most commonly assessed outcome, measured using the Visual Analog Scale (VAS) in all studies. Functional disability was evaluated using the Roland-Morris Disability Questionnaire (RMDQ) in all studies (16-23) or the Oswestry Disability Index (ODI) in two studies (20, 22). Additional assessments included range of motion, pressure pain threshold, and quality of life indices.
4.5. Interventions
The eight RCTs investigated a diverse array of non-pharmacological interventions for chronic low back pain (CLBP), indicating both traditional and modern therapeutic approaches. These interventions can be categorized into five broad modalities.
4.5.1. Traditional Manual Therapies
Fateh massage, a Persian manual therapy rooted in Iranian traditional medicine, involving rhythmic compressions, deep tissue manipulation, and stretching techniques. It was compared with acupuncture and physiotherapy in a three-arm RCT involving 90 patients (16). A scraping technique, known as Gua Sha, using a smooth-edged instrument to stimulate microcirculation and relieve musculoskeletal tension. The intervention was administered weekly for 4 weeks (18). Tuina, a form of Chinese therapeutic massage, was combined with core strengthening exercises to enhance spinal stability. The intervention lasted 4 weeks (22). Participants were trained in self-administered Thai massage techniques and stretching exercises, performed daily over a 4-week period (20).
4.5.2. Acupuncture-Based Therapies
Electronic acupuncture shoes was used as a novel wearable device delivering low-frequency electrical stimulation to acupuncture points on the soles. The intervention was applied twice daily for 12 weeks (17). Hand-ear acupuncture, a dual-modality acupuncture technique targeting auricular and hand meridians, administered twice weekly for 6 weeks (21).
4.5.3. Mind-Body Exercise
Tai Chi, a 10-week program of Yang-style Tai Chi, practiced twice weekly, emphasizing slow, controlled movements and postural awareness to improve pain and function (19).
4.5.4. Topical Herbal Therapy
Comfrey root extract ointment is a topical application of Symphytum officinale (comfrey) root extract, applied three times daily for 5 days to treat acute back pain (23).
4.5.5. Conventional Comparators
4.6. Treatment Effectiveness
All eight RCTs reported statistically significant improvements in pain intensity and/or functional outcomes following their respective interventions (16-23). However, several studies (16-18, 20, 23) did not report effect sizes or confidence intervals, limiting the ability to quantify the magnitude of treatment effects. In the Namiranian et al. study, all three groups (Fateh massage, acupuncture, physiotherapy) showed significant within-group reductions in VAS and RMDQ scores (P < 0.05), but no significant between-group differences were observed (P > 0.05), indicating comparable efficacy (16). In the study conducted by Yeh et al., participants using electronic acupuncture shoes demonstrated a treatment success rate of 84% compared to 62% in the control group (P = 0.04). The VAS scores were significantly lower at visits 5 and 9 (P = 0.048), though effect sizes and confidence intervals were not reported (17).
In Saha et al.’s study, Gua Sha therapy led to a mean VAS reduction of -16.2 mm on a 100 mm scale (P < 0.001) and improved health status (P = 0.002). While the effect size was clinically meaningful, confidence intervals were not provided (18).
Based on the results from Hall et al.’s study, Tai Chi significantly reduced pain intensity by 1.3 points on a 10-point scale (95% CI: 0.6 to 2.0, P < 0.001) and improved RMDQ scores by 2.6 points (95% CI: 1.4 to 3.8, P < 0.001), indicating a moderate-to-large effect size.
In Buttagat et al.’s study, Thai self-massage with stretching significantly improved VAS, ODI, and flexibility scores (P < 0.05 for all outcomes). While statistical significance was achieved in this study, effect sizes and confidence intervals were not detailed (20). In Luo et al.’s study, hand-ear acupuncture improved RMDQ scores by 7.74 points at 6 months (P < 0.001), with an efficacy rate of 88.9% compared to 45.8% in the control group (P < 0.001), suggesting a large treatment effect (21). Tang et al.’s study results indicate that the combination of Tuina and core stability exercises significantly reduced VAS scores and improved JOA scores (P < 0.05 for both), with a lower recurrence rate (17.1% vs. 43.9%, P < 0.05; 22). Additionally, Giannetti et al. observed that Comfrey root extract ointment resulted in a 95.2% reduction in pain on movement versus 37.8% in the placebo group (P < 0.001), with significant improvements in all secondary outcomes. Exact effect sizes and confidence intervals were not reported for this study (23). See study details in Table 2.
Table 2.Study Characteristics
| Authors and Ref | Year | Country | Age (y) | Number of Participants | Indication | Intervention | Assessment Tools | Treatment Sessions | Provider | Efficacy | Adverse Effects |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Namiranian et al. (16) | 2022 | Iran | 20 - 60 | 90 | Chronic LBP (≥ 3 mo) | Fateh massage, acupuncture, and physiotherapy | VAS, RMDQ | Ten sessions over 5 weeks | Trained therapists, acupuncturists, and physiotherapists | Significant within-group reductions in VAS and RMDQ (P < 0.05); no between-group differences (P > 0.05); effect sizes and CIs not reported | None reported |
| Yeh et al. (17) | 2020 | Taiwan | ~ 45 | 80 | Chronic LBP (≥ 3 mo) | Electronic acupuncture shoes vs. sham | VAS, RMDQ | Twice daily for 12 weeks | Self-administered (device) | Eighty-four percent success rate vs. 62% in control (P = 0.04); lower VAS at visits 5 and 9 (P = 0.048); effect sizes and CIs not reported | None reported |
| Saha et al. (18) | 2019 | Germany | Not specified | 60 | Chronic LBP (≥ 12 wk) | Gua Sha vs. control | VAS, RMDQ | Weekly for 4 weeks | Trained therapists | Mean VAS reduction of 16.2 mm (P < 0.001); improved health status (P = 0.002); CIs not reported | Minor skin irritation in some participants |
| Hall et al. (19) | 2011 | Australia | 18 - 70 | 160 | Chronic non-specific LBP | Tai Chi vs. waitlist control | VAS, RMDQ | Twice weekly for 10 weeks | Tai Chi instructors | Pain reduction by 1.3 points (95% CI: 0.6 - 2.0, P < 0.001); RMDQ improved by 2.6 points (95% CI: 1.4 - 3.8, P < 0.001) | None reported |
| Buttagat et al. (20) | 2020 | Thailand | 20 - 60 | 44 | Chronic non-specific LBP (≥ 3 mo) | Thai self-massage with stretching vs. control | VAS, ODI, flexibility | Daily for 4 weeks | Self-administered (trained) | Significant improvements in VAS, ODI, and flexibility (P < 0.05); effect sizes and CIs not reported | None reported |
| Luo et al. (21) | 2019 | China | 18 - 65 | 72 | Chronic LBP | Hand-ear acupuncture vs. usual care | RMDQ | Twice weekly for 6 weeks | Acupuncturists | RMDQ improved by 7.74 points at 6 months (P < 0.001); 88.9% efficacy vs. 45.8% in control (P < 0.001) | None reported |
| Tang et al. (22) | 2016 | China | Not specified | 82 | Chronic LBP with lumbar degenerative instability | Tuina ± core stability exercises | VAS, JOA | Weekly for 4 weeks | Trained Tuina therapists | Significant reductions in VAS and improved JOA (P < 0.05); lower recurrence rate (17.1% vs. 43.9%, P < 0.05); effect sizes not reported | None reported |
| Giannetti et al. (23) | 2010 | Germany | 18 - 60 | 141 | Acute upper or lower back pain | Comfrey root extract ointment vs. placebo | VAS, RMDQ | Three times daily for 5 days | Self-administered (ointment) | 95.2% reduction in pain on movement vs. 37.8% in placebo (P < 0.001); effect sizes and CIs not reported | None reported |
Abbreviations: LBP, low back pain; VAS, Visual Analog Scale; RMDQ, Roland-Morris Disability Questionnaire; ODI, Oswestry Disability Index; JOA, Japanese Orthopaedic Association score.
4.7. Risk of Bias in Included Studies
The methodological quality of the eight included RCTs was assessed using the Cochrane Risk of Bias 2.0 tool, which evaluates seven domains of potential bias (15). Overall, the studies demonstrated moderate to low risk of bias, though several domains showed variability across trials. All studies reported using randomization procedures, with five explicitly describing adequate methods such as computer-generated sequences or block randomization (17-19, 22, 23), indicating low risk. Others (16, 20, 21) did not detail the randomization method, resulting in unclear risk. Adequate allocation concealment was reported in four studies (17-19, 23), using sealed envelopes or centralized randomization, suggesting low risk. The remaining studies lacked sufficient detail, leading to unclear risk (16, 20-22). Blinding was feasible and implemented in studies using sham or placebo controls (17, 18, 23), rated as low risk. However, trials involving physical interventions such as massage or Tai Chi (16, 19, 20) were open-label, resulting in high risk of performance bias. Six studies reported assessor blinding (17-19, 21-23), indicating low risk. In two studies (16, 20), blinding of outcome assessors was not clearly described, leading to unclear risk.
All studies reported attrition rates and used intention-to-treat or per-protocol analyses. Dropout rates were generally low (< 10%), and reasons for withdrawal were documented, resulting in low risk across all trials. No evidence of selective outcome reporting was identified. All studies reported prespecified primary and secondary outcomes, and trial protocols (where available) aligned with published results, indicating low risk. No major concerns were identified regarding baseline imbalances, funding conflicts, or deviations from protocol. However, small sample sizes in some studies (18, 20) may limit generalizability. The risk of bias is summarized for each study in Table 3.
Table 3.Bias of the Included Studies
| Study and Ref | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|
| Namiranian et al. (16) | Unclear | Unclear | High | Unclear | Low | Low | Moderate |
| Yeh et al. (17) | Low | Low | Low | Low | Low | Low | Low |
| Saha et al. (18) | Low | Low | Low | Low | Low | Low | Low |
| Hall et al. (19) | Low | Low | High | Low | Low | Low | Moderate |
| Buttagat et al. (20) | Unclear | Unclear | High | Unclear | Low | Low | Moderate |
| Luo et al. (21) | Unclear | Unclear | High | Low | Low | Low | Moderate |
| Tang et al. (22) | Low | Unclear | High | Low | Low | Low | Moderate |
| Giannetti et al. (23) | Low | Low | Low | Low | Low | Low | Low |
5. Discussion
Our systematic review synthesized evidence from eight RCTs evaluating diverse complementary and alternative therapies (CATs) for back pain. Overall, the results underscore the clinical potential of therapies such as Tai Chi, Gua Sha, traditional massage methods, acupuncture modalities, and topical herbal preparations in alleviating pain, reducing disability, and enhancing functional capacity. Multiple studies demonstrated statistically significant reductions in pain intensity using validated outcomes like the VAS and ODI. For instance, Tai Chi, a low-impact mind-body practice, was associated with moderate to large improvements in pain and disability metrics (19), supporting previous evidence that mind-body interventions can modulate neuromuscular control and central sensitization (24, 25). Similarly, Luo et al. demonstrated a substantial effect of hand-ear acupuncture on RMDQ scores (21), echoing findings in systematic reviews where acupuncture has been shown to outperform placebo and conventional care in reducing CLBP symptoms (26, 27). Manual therapies such as Gua Sha (18), Fateh massage (16), and Thai self-massage (20) also yielded positive outcomes, reinforcing the role of tactile stimulation and fascial manipulation in pain inhibition, potentially via the gate control theory and myofascial trigger point deactivation (28, 29). Notably, Giannetti et al. reported high efficacy of comfrey root extract ointment in managing acute lower back pain (23), which aligns with prior findings on its anti-inflammatory and analgesic properties (30, 31). However, the lack of reported effect sizes and confidence intervals in several studies (16-18, 20, 23) limits the ability to quantify the magnitude of these effects and perform a meta-analysis, highlighting the need for standardized reporting in future research. Despite these promising results, methodological limitations must be acknowledged. Blinding was not feasible in most physical or exercise-based interventions, introducing performance bias, and allocation concealment procedures were often inadequately reported. Additionally, sample sizes were modest in several trials, and follow-up durations were limited, reducing the ability to draw conclusions about long-term efficacy and recurrence. Furthermore, publication bias may have influenced the findings, as the limited number of included studies (n = 8) and the predominance of positive results suggest that studies with null or negative outcomes may be underreported. The inclusion of only peer-reviewed studies in English and Persian may have excluded relevant unpublished or gray literature, potentially skewing the results toward positive outcomes. Future reviews should incorporate broader searches, including gray literature and non-English publications, to mitigate this risk.
Nonetheless, this review aligns with clinical practice guidelines that advocate non-pharmacologic interventions as first-line strategies for CLBP management (32, 33). The results suggest that CATs, when implemented judiciously, could contribute to a multimodal, patient-centered approach to chronic pain. Importantly, cultural context and patient preference, often overlooked in conventional paradigms, may enhance adherence and satisfaction with CAT-based regimens (34, 35).
It is worth mentioning that a meta-analysis was not conducted in this review due to substantial heterogeneity among the included studies. The interventions varied widely in modality (e.g., massage, Tai Chi, acupuncture, herbal ointments), treatment duration, comparator groups, and outcome measures (e.g., VAS, RMDQ, ODI). Additionally, several studies did not report sufficient quantitative data — such as standardized effect sizes, standard deviations, or confidence intervals — necessary for calculating pooled estimates. Given these methodological and reporting inconsistencies, a quantitative synthesis was deemed inappropriate, and a narrative synthesis was conducted instead to preserve the integrity and interpretability of the findings. Future studies should aim to standardize protocols across CAT modalities, report precise effect sizes and confidence intervals, and adopt longer-term follow-up. Comparative trials assessing CATs as adjuncts to conventional therapies could further refine their integration into modern rehabilitation frameworks. Most of the variables used in the present study are related to the evaluation of pain intensity and performance level, whose findings mainly confirm the positive effects of these treatment methods.
5.1. Conclusions
This systematic review demonstrates that CATs offer promising, non-pharmacological options for managing CLBP. Across eight RCTs, modalities such as Tai Chi, traditional massage techniques, acupuncture variations, Gua Sha, and comfrey root extract were associated with significant reductions in pain intensity and improvements in functional outcomes. While the degree of effect varied, several interventions, particularly Tai Chi and acupuncture, showed moderate to large treatment effects with acceptable safety profiles. These findings support recent clinical guidelines advocating for integrative approaches to CLBP that prioritize patient-centered care and minimize reliance on pharmaceuticals.
Nonetheless, limitations in study design and reporting temper the strength of these conclusions. Several trials exhibited risks of performance or detection bias, and few provided long-term follow-up or standardized effect estimates. The geographic concentration of included studies, primarily from Iran, China, and Taiwan, may limit the generalizability of findings to other populations with different cultural and healthcare contexts. The heterogeneity in intervention protocols also limits direct comparisons. To solidify the role of CATs in mainstream care, future research should emphasize methodological rigor, include larger and more diverse patient populations, and evaluate both clinical and economic outcomes over time. Despite these gaps, the collective evidence suggests that CATs are valuable additions to the therapeutic arsenal for individuals suffering from CLBP.

