




1. Background
In recent years, in addition to a decrease in birth rate, the number of mothers ≥ 35 has been increasing (1). Based on this fact, and also the high incidence of Down syndrome with maternal age, as well as some other chromosomal anomalies, the efforts for prenatal diagnosis of these disorders have risen (2). In spite of introducing non-invasive prenatal tests, including prenatal aneuploidy screening program combined with NT (nuchal translucency), invasive antenatal test is yet widely being used around the world (3)). Amniocentesis is the gold standard and most commonly an invasive antenatal test for diagnosis of fetal chromosome abnormalities (4). Most of these abnormalities are numerical, and minority are structural and mosaicism (about 86%, 6%, and 8%, respectively) (5, 6). Various clinical indications affect the distribution of prenatal chromosome abnormality identification 4. Introduction of non-invasive prenatal testing changed the frequency of chromosomal abnormalities. However, cell-free fetal DNA testing, as the best screening test for common chromosomal abnormalities, failed to be a universal prenatal aneuploidy screening due to its high cost and false positive rate (7). Trisomy 21, known as Down syndrome, is the most prevalent chromosomal abnormality, which is associated with intellectual disability. The rates of fetal chromosomal aneuploidies in central Iran, Tehran, and north of Iran is 5.2%, 3.1%, and 1.5% - 1.7%, respectively (6).
2. Objectives
In this study, we determined the incidence and the type of chromosome abnormalities in the first and second trimester of pregnant women using amniocentesis in Khuzestan, south of Iran.
3. Methods
3.1. Subjects
This retrospective study was conducted on 1197 pregnant women undergoing amniocentesis for chromosomal abnormality detection at second trimester (18 - 24 weeks of gestation). The study population was recruited from the Prenatal Care Clinic at Imam Khomeini Hospital from 2012 to 2013. The amniotic fluids specimens were analyzed at Narges Medical Genetic Lab, Ahvaz, Iran.
3.2. Data Analysis
The data were analyzed using SPSS version 20.
4. Results
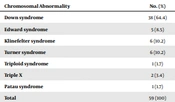
The incidence of abnormal aneuploidies was 4.9% (59 of 1197) for all specimens (Table 1). The highest chromosomal abnormality was Down syndrome (64.4%).
Table 1.The Incidence of Abnormal Aneuploidies
| Chromosomal Abnormality | No. (%) |
|---|---|
| Down syndrome | 38 (64.4) |
| Edward syndrome | 5 (8.5) |
| Klinefelter syndrome | 6 (10.2) |
| Turner syndrome | 6 (10.2) |
| Triploid syndrome | 1 (1.7) |
| Triple X | 2 (3.4) |
| Patau syndrome | 1 (1.7) |
| Total | 59 (100) |
5. Discussion
We reported an analyses of chromosomal aneuploidies identified among 1197 pregnant women undergoing amniocentesis within second trimeste. We found the rate of chromosomal abnormalities in 4.9% of amniocentesis specimens. The rate of chromosomal abnormalities in central Iran, Tehran and north of Iran were 5.2%, 3.1% and 1.5% - 1.7%, respectively (8-10). Studies in other countries reported lower rate, between 2.7% - 3.1% than our study (11-13). However, a study in Japan reported the rate of 6% (1).
According to our studies and previous reports the trisomy 21 remains the most common chromosomal abnormalities. We detected that 64.4% of chromosomal abnormalities were Down syndrome. In a study in Tehran, Iran the detection rate of Down syndrome at second trimester was 81%, which was higher than our study (6). Some other studies from other countries reported much lower rates of trisomy 21 detection including 46%, 35.6% and 36.9% of all chromosomal abnormalities (2, 13, 14). These varieties may be attributed to differences in maternal age of populations evaluated in different studies.
5.1. Conclusions
The rate of chromosomal abnormalities was higher than other reports from Iran and all over the world. The detection rate of Down syndrome similar to other reports remains high.


