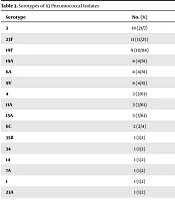
Streptococcus pneumoniae is one of the leading causes of pediatric and adult infections. The serotype distribution, antimicrobial resistance, and genotypes vary across different populations and change over time in each geographical region. Although the results of such studies seem to be of local use, they not only can improve global health by affecting pneumococcal vaccine immunization programs but also raise global awareness about antimicrobial resistance and molecular aspects of pneumococcal infections. This four-year surveillance study revealed that the most common serotypes of blood-isolated pneumococci in our region were 19A, 1, 23F, 19F, 14, and serogroups 15 (B/C) and 6 (A/B), which look like other countries before pneumococcal conjugate vaccination (
15,
23,
24). The PCV10 and PCV13 types covered 66.64% and 86.24% of serotypes, respectively, which, like other studies, illustrates that PCV13 could be suitable for controlling
S. pneumoniae isolates in this region (
25).
All of our isolates were highly resistant to tetracycline, erythromycin, clindamycin, trimethoprim-sulfamethoxazole, and chloramphenicol. Contrary, most isolates were susceptible to cefotaxime and penicillin. Of importance, all isolates were susceptible to vancomycin. The highest antimicrobial resistance rate was seen for the 1 and 19A serotypes, while the 6A/B serotype showed the lowest resistance.
Table 1 shows that, except for vancomycin, the antimicrobial resistance rate followed an increasing pattern from 2014 to 2018. Penicillin-resistant
S. pneumoniae emerged as a global problem in the past decade, and it seems that beta-lactam resistance was increasing during the last few years. In the present study, 35.3% of the isolates were PNSP, while the overall prevalence of PNSP was lower in other studies. Its prevalence in Morocco was 22.2% from 2007 to 2014 (
26). In other studies, the resistance rate to penicillin in
S. pneumoniae was 28% and 20% in Tehran, Iran, and in non-meningitis isolates of pneumococci was 10.7% in Shanghai, China (
1,
2,
25).
Some studies proved that PCV vaccination led to a decrease in the prevalence of antibiotic-resistant strains. Diawara et al. (
26) showed that the resistance rate to penicillin decreased from 34.5% to 22.9% after PCV vaccination in children. The reduction in the PNSP rate after PCV vaccination was reported in several countries (
23,
27-
29). Regarding relatively high resistance against penicillin in our isolates and also high serotype coverage of the 13-valent vaccine, it seems that the PCV vaccination could be useful to prevent the spread of resistant strains. The most prevalent serotypes among our PNSP were 19F, 19A, 23F, 14, 15B/C, 6A/B, and 1. No meaningful correlation was observed between serotypes and penicillin resistance (P > 0.05). These serotypes were mainly covered by PCV-13.
Serotypes 14, 6A/B, and 19F were observed among highly resistant isolates with penicillin MICs ≥ 32. Dissemination of 19F isolates has increased in many parts of the world, and they have become resistant to penicillin (
30-
32). In this study, all 19F isolates were resistant to penicillin. It should be noted that regardless of antimicrobial resistance, the most prevalent serotypes among our isolates were 19A, 6A/B, 1, 23F, 19F, 14, 15B/C, and 15A, respectively. In a similar study in Trinidad and Tobago, the most prevalent serotypes among invasive isolates were 19F, 6B, 23F, 3, 19A, 6A, 14, and 9V, respectively (
33). In another study in China, the most common serotypes were 19F, 19A, 15, 6B, 6A, and 17 (
34). Comparing our results with other studies shows partial differences in various geographical areas (
3,
24,
35-
39); for example, serotype 1 was not reported in China and Trinidad and Tobago studies, but we found it in our isolates. Conversely, serotypes 3 and 17 were found in that two countries though we did not observe it in our study.
The MLST analysis of
S. pneumoniae isolates in different countries showed that some international clones such as Spain
23F-1, Spain
6B-2, or England
14-9 are circulating worldwide (
1,
40,
41). The MLST analysis of PNSP isolates in this study revealed that three highly penicillin-resistant isolates with MIC ≥ 16 belonged to international clones, Sweden15A-25-19A (ST63), Taiwan19F-14-1, and Taiwan19F-14 (ST236). Importantly, for our Taiwan19F-14-1 and Taiwan19F-14 isolates, the MICs were higher than previously reported (
41). In primary introduced Taiwan19F-14-1 and Taiwan19F-14, the penicillin MIC was 2, but in our isolates and variants, the MIC was minimally ≥ 8. Other prevalent STs in our isolates were ST2687, ST320, and ST3130. It should be noted that ST320 is a DLV, and ST271 is an SLV of the ST236 Taiwan19F-14 clone (
Figure 1). The spread of ST320 can be problematic because it is an international virulent MDR strain (
42). This strain has been reported in many countries and is commonly found in North America, Europe, China, and other Asian countries (
2,
15,
42,
43). All of our ST320 isolates belonged to serotype 19A (
Figure 1).
In the present study, 82.35% of the isolates were classified as MDR. The relatively high presence of Taiwan19F-14 clones and their related STs put them as significant clones in circulation. Talebi et al. (
2) reported that common STs in erythromycin-resistant isolates of pneumococci were ST3130, ST180, and ST81. According to the results of another study by Raddoui et al. (
44), ST81 was the most prevalent sequence type in macrolide-resistant
S. pneumoniae isolates. Between 2007 and 2013, the most common ST in MDR pneumococci isolates was ST320 in Canada (
15). Lucas et al. (
33) reported that ST138, ST36, and ST180 were the most common sequence types in Trinidad and Tobago, while in this study, the most common STs in MDR isolates were 2687, 320, 236, 3130, 271, 329, 63, 7577, 10081, 13823, and 9777, respectively.
Serotype switching was observed in serotype 19A PNSP belonging to ST320 and ST276, serotype 19F distributed in ST3130, ST271, and ST236, and serotype 14 found in ST329 and ST143. A high rate of capsular switching was reported in other studies, especially in regions with national vaccination programs. Interestingly, we observed a high level of serotype switching in our isolates, although, in Iran, the state-run vaccination program has not been carried out yet. Therefore, further studies are required to confirm the relationship between serotype switching and vaccination. Finally, it seems that our PNSP isolates belonged to diverse clones that may be due to the various races living in this geographical area (
Figure 2).
5.1. Conclusions
In conclusion, the current study showed that serotypes 19A, 6A/B, 1, 23F, 19F, 14, and 15B/C were commonly isolated from blood cultures of children under five-years-old. It seems that PCV-13 with the 86.24% coverage of blood isolates of pneumococci is the most suitable choice for vaccination in this region. Other important points are a relatively high prevalence of PNSP and MDR strains between 2014 and 2018. The MLST surveillance showed that the Taiwan19F-14 clone and its related STs played an essential role in disseminating resistant S. pneumoniae isolates in Bojnurd, Iran. Hence, to select the optimal antimicrobial treatment, to understand the distribution pattern of clones, and to have the most effective immunization program for S. pneumoniae-related diseases, long-term regional surveillance could be beneficial.







 are displayed as a single eBURST diagram by setting the group definition to 0 of 7 shared alleles. STs found in this study are labeled and other ST labels have been removed. Our STs belonged to CC0, CC3, CC84, CC100, CC832, and CC2029.")