The findings of this study reveal a concerning prevalence of carbapenemase genes among
A. baumannii isolates from Al-Azizya Hospital. The
blaOXA-51 gene, an intrinsic marker for
A. baumannii, was detected in all isolates, confirming their identity. This aligns with global studies reporting the ubiquity of
blaOXA-51 in
A. baumannii isolates, often accompanied by other carbapenemase genes such as
blaOXA-23 and
blaOXA-58 (
24). The presence of these genes is particularly alarming due to their association with MDR, a significant challenge in healthcare settings (
25). The detection of
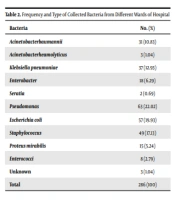
blaOXA-23 (26%),
blaVIM (24%),
blaOXA-48 (22%), and
blaNDM (21%) highlights the genetic diversity of carbapenem resistance mechanisms in this region. These findings are consistent with studies in the Middle East, such as in Iraq and Egypt, where
blaOXA-23 was the predominant gene among CRAB and
Klebsiella pneumoniae isolates, with
blaNDM also contributing significantly to resistance profiles (
15,
16,
26). Similarly, a Jordanian study reported high resistance to meropenem (98.1%) and imipenem (87.7%), mirroring our observed rates (96% and 95%, respectively) (
14).
However, contrasting results have been reported in other regions. For instance, a study in South Korea found a lower prevalence of
blaNDM (5%) among
A. baumannii isolates, with
blaOXA-23 dominating at 80%, suggesting regional variations in resistance gene distribution (
13). In Europe, particularly in Greece,
blaVIM was more prevalent than
blaOXA-23 in some hospital settings, highlighting differing resistance mechanisms (
12,
18,
22). These comparisons underscore the need for region-specific surveillance to tailor infection control strategies.
The presence of
blaOXA-23 is particularly concerning due to its association with high-level carbapenem resistance and its role in hospital outbreaks. This gene is often linked to insertion sequences that enhance its expression and mobilization, contributing to the virulence and resistance of
A. baumannii (
27). Similarly, detecting
blaVIM and
blaNDM, which encode metallo-β-lactamases, further complicates treatment options. These genes confer resistance to a broad range of β-lactam antibiotics, including carbapenems, which are often considered last-resort treatments for severe infections (
28). The emergence of these resistance genes poses a significant public health threat, necessitating alternative treatment strategies such as combination therapies or newer antibiotics like cefiderocol (
29).
The antibiotic resistance patterns observed in this study reflect a global trend of increasing resistance among
A. baumannii isolates. The highest resistance rates were observed against ceftazidime (100%), meropenem (96%), and imipenem (95%), which are critical antibiotics for treating MDR infections. These findings are consistent with reports from other regions, highlighting the urgent need for enhanced surveillance and infection control measures to mitigate the spread of resistant strains (
14). The COVID-19 pandemic has further exacerbated these trends, with shifts in bacterial prevalence and resistance profiles observed during this period (
30). The resistance to cephalosporins and carbapenems underscores the need for alternative treatment options and stricter antibiotic stewardship programs. Newer agents such as ceftazidime-avibactam, meropenem-vaborbactam, and cefiderocol have shown promise against resistant strains and should be considered in treatment regimens (
31). Effective stewardship programs are essential to optimize antibiotic use, reduce unnecessary prescriptions, and monitor resistance patterns, thereby preserving the efficacy of existing antibiotics (
32).
While aztreonam retains some utility against CRAB, with a resistance rate of approximately 59%, its effectiveness varies depending on the specific resistance mechanisms present. Susceptibility testing is therefore crucial before treatment (
33). Similarly, the high resistance rates to aminoglycosides (50.2%) and fluoroquinolones (65.7%) among CRAB isolates further limit therapeutic options, necessitating the exploration of alternative therapies and combination treatments (
34,
35).
The high prevalence of carbapenemase genes and antibiotic resistance in
A. baumannii isolates from Al-Azizya Hospital underscores the urgent need for stringent infection control measures. The ability of
A. baumannii to form biofilms enhances its persistence in clinical settings, complicating eradication efforts (
36). To mitigate the spread of resistant strains, healthcare facilities must implement rigorous infection control protocols, including enhanced surveillance, strict hand hygiene, contact precautions, and environmental disinfection (
37). Continuous education and training for healthcare workers are also vital to ensure compliance with these measures (
38).
While this study provides valuable insights into the molecular characteristics of A. baumannii isolates, it is limited by a small sample size from a single hospital and a focus on carbapenemase genes without exploring other resistance mechanisms. Clinical variables such as patient age, underlying diseases, and immunodeficiency status were not examined. Future studies should incorporate these factors to identify risk factors for CRAB infections and inform targeted prevention strategies.
5.1. Conclusions
This study demonstrates the high prevalence of carbapenemase genes and antibiotic resistance in A. baumannii isolates from Al-Azizya Hospital in Wasit, Iraq. The presence of blaOXA-23, blaVIM, blaOXA-48, and blaNDM genes highlights the genetic diversity of carbapenem resistance mechanisms in this region. These findings underscore the urgent need for effective infection control measures, including strict antibiotic stewardship and enhanced surveillance of CRAB in Iraqi hospitals. Additionally, the development of new therapeutic strategies, such as combination therapies and novel antibiotics, is essential to combat the growing threat of multidrug-resistant A. baumannii.
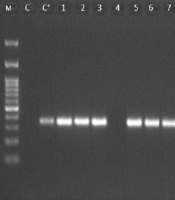




 DNA size marker (100 - 1500 bp), (C-) negative control, (C+) positive control, 1 - 17, PCR products from <i>A. baumanii</i> isolates, displaying expected bands (353 bp).")
 DNA size marker (100 - 1500 bp), (C-) negative control, (C+) positive control, 1 - 17, PCR products from isolates, displaying predictable bands (621 bp), indicative of the amplified <i>bla</i><sub>NDM</sub> gene; B, lanes: (M) DNA size marker (100 - 1500 bp), (C-) negative control, (C+) positive control, 1 – 17, PCR products from isolates, exhibiting expected bands (390 bp), representing the amplified <i>bla</i><sub>VIM</sub> gene; C, lanes: (M) DNA size marker (100 - 1500 bp), (C+) positive control, (C-) negative control, 1 - 17, PCR products from isolates, displaying expected bands (390 bp), corresponding to the amplified <i>bla</i><sub>OXA-23</sub> gene; D, lanes: (M) DNA size marker (100 - 1500 bp), (C-) negative control, (C+) positive control, 1 - 17, PCR products from isolates, showing a band at 390 bp, representing the amplified <i>bla</i><sub>OXA-48 </sub>gene.")