According to WHO, infertility is a disease that affects the reproductive system and is defined as the failure to achieve a clinical pregnancy after having 12 months (or more) of regular unprotected sexual intercourse (
1). One of the crucial causes of male infertility is urogenital infections and it is estimated that about 15% of male infertilities are caused by such infections (
25).
Chlamydia trachomatis and
L. monocytogenes are among the serious pathogens that cause sexually transmitted diseases all around the world (
26). In most cases, the infection is asymptomatic, so that about 70% to 80% of infected females and 50% of infected males present no symptom of infection (
27). Acute chlamydial infection in males causes urethritis, epididymitis, and prostatitis. Epididymitis is an inflammation that can cause infertility by preventing sperms from getting into the ejaculate, particularly when both testicles are involved (
28). Studies showed that
C. trachomatis can bind to sperm cell surfaces through its lipopolysaccharides and induce apoptosis (
29). Infection with
C. trachomatis directly affects semen parameters or indirectly changes the sperm quality via tissue inflammation, and ultimately causes male fertility (
30).
Listeria monocytogenes, an intracellular and opportunistic pathogen, enter the body through contaminated water and food and cause a systemic infection called listeriosis, which in turn causes meningoencephalitis in pregnant women, the elderly, and those with immunodeficiency (
13). The clinical spectrum of listeriosis contains two specific targets; the placental-maternal unit and the central nervous system (
15). Listeriosis in pregnant women is asymptomatic or has mild flu-like symptoms. Besides, after crossing the blood-brain barrier, the bacteria causes neonatal septicemia and meningitis, abortion, and preterm labor.
Listeria monocytogenes phospholipases play an essential role in its pathogenesis (
31).
According to the literature, results about the effects of Chlamydia infection on semen parameters are controversial. Moazenchi and colleagues showed that 11% of those infected with
C. trachomatis had sperm abnormalities (
32). In the current study, only azoospermic specimens infected with
C. trachomatis had a significant association with sperm abnormalities (P < 0.05), and no significant association with nonazoospermic samples was found (P > 0.05). The study conducted by Gdoura and colleagues on 104 asymptomatic male patients with infertility in Tunisia reported that the detection of
C. trachomatis in semen specimens had no significant association with abnormalities in semen parameters (P > 0.05) (
12). Zhu and colleagues reported a significant correlation between chronic chlamydial infection and infertility in males and females. In a five-year investigation (2010 to 2014), they found an increasing prevalence of
C. trachomatis infection (by about 3.15%) and reported no significant effect of the infection on semen parameters (P > 0.05) (
33).
In the present study, no significant association was observed between abnormalities in semen parameters and the detection of
L. monocytogenes in the specimens (P > 0.05). To the best of knowledge of authors, no study is conducted thus far on
L. monocytogenes and its bacteriospermia effects on males with infertility. Because PCR diagnostic method is the most sensitive test for the detection of
C. trachomatis and
L. monocytogenes, in the current study the presence of these two bacteria in semen specimens of infertile men was assessed using this method. In a study conducted by Samplaski and colleagues on infertile men using the PCR assay at Toronto’s Mount Sinai Hospital, the presence of
C. trachomatis was estimated to be about 0.3% (
34).
The prevalence of
C. trachomatis reported in the aforementioned studies is lower than the current study. In a research done by Sellami and colleagues on the semen of infertile men using the PCR molecular method, about 15.2% of 85 specimens were positive for the presence of
C. trachomatis (
17). In a study conducted by Sadrpour and colleagues on 120 semen samples from infertile men in the Avicenna Infertility Treatment Center in Tehran (Iran),
C. trachomatis was identified in 23.3% of the specimens (
35). These results are consistent with the results of the current study. Hence, it seems that the screening of men to find out
C. trachomatis infection, as one of the major causes of infertility, is of crucial importance.
Eslami and colleagues used the PCR method and reported that about 16% of 96 women with recurrent abortions were infected with
L. monocytogenes (
18). Goudarzi and colleagues detected seven cases of
L. monocytogenes positive (among 87 vaginal swab specimens from women with abortion) using the PCR assay (
36). In a molecular assessment performed by Le Monnier and colleagues to detect
L. monocytogenes, molecular techniques, including PCR, were introduced as rapid and reliable assays to detect the bacteria in clinical samples (
37). Lotfollahi and colleagues showed that 9 (out of 100) vaginal samples with a history of abortion, were detected to be infected with
L. monocytogenes (
38). These results were achieved on women with recurrent abortion with a similar method (PCR) that we used on infertile men for detecting
L. monocytogenes. By comparing the results of the current study with those of other studies, it can be concluded that differences in the ratio of these bacteria can be attributed to factors such as the selection and gender of the patients, the number of samples under study, the use of different diagnostic methods, the difference in the geographical distribution of populations, the rate and severity of bacterial colonization in the urogenital tract, and the sensitivity of the primers used in the test as well as sample volumes.
5.1. Conclusions
According to the findings, accurate sperm analysis to diagnose changes in semen parameters, as well as the application of PCR as a rapid and sensitive technique to detect the bacteria, are essential for all infertile men, particularly for asymptomatic patients. Also, the promotion of public education and raising the awareness of males about sexual health and the necessity of preconception screenings can be great preventive steps against infertility.





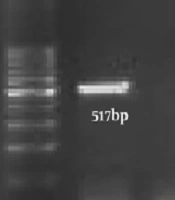
; C+: Positive Control; C-: Negative Control; Positive Samples: 3, 12, 22; Negative Samples: 1, 2, 4 - 11, 13 - 21, 23 – 25 (A). Amplification product of <i>Listeria monocytogenes</i> obtained from semen samples in infertile men. M: Size Marker 1 Kb DNA Ladder (Bioflux); C+: Positive Control; C-: Negative Control; Positive Samples: 1, 2, 3; Negative Samples: 4 – 15 (B).")