Vancomycin is associated with an increased risk of kidney impairment, with reported nephrotoxicity rates ranging from 5% to 35%. Prolonged use, especially beyond seven days, significantly elevates the likelihood of these adverse effects (
20).
Understanding the mechanisms underlying vancomycin-associated nephrotoxicity is crucial for developing effective preventive strategies. Current research suggests that nephrotoxicity may arise from factors such as oxidative stress, mitochondrial dysfunction, and inflammatory pathways, underscoring the importance of continued investigation in this field (
5). However, the precise mechanism remains unclear.
Theophylline has been studied for its potential to mitigate vancomycin-induced nephrotoxicity and reduce the incidence of AKI associated with vancomycin use (
21). However, clinical guidelines recommend exercising caution when using it for the prevention of AKI.
The maximum safe dose of theophylline is 12 to 14 mg/kg. However, due to its extremely narrow therapeutic window, a dose of 10 mg/kg/day, divided into two administrations, was prescribed in this study to minimize the risk of toxicity (
22). No adverse effects were observed through active clinical monitoring. Additionally, severe side effects like nausea, vomiting, cardiac arrhythmias, hypotension, and convulsions were not reported during the treatment (
23). Theophylline has been investigated in numerous studies for its potential to prevent nephrotoxicity, including CIN, with varying outcomes. In this study, a safe and conservative dose of theophylline was used to evaluate its effects.
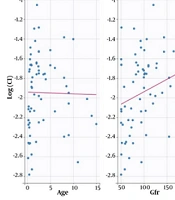
Results showed that the average microalbumin levels on the third day post-intervention were lower in the intervention group compared to the control group, though this difference was not statistically significant. However, by the 10th and 30th days, the differences between the groups became statistically significant. Importantly, all microalbumin values remained within the normal range, suggesting the observed effect may represent a modulation of subclinical renal stress rather than prevention of overt AKI. Blood urea nitrogen levels levels increased in the control group, while eGFR remained stable in the control group and showed an increase in the treatment group. The changes in the intervention group were more pronounced, with statistically significant reductions observed on the 10th and 30th days, in contrast to the 3rd day, where no significant changes were noted.
The results indicate that theophylline did not significantly affect eGFR, BUN, or microalbumin levels compared to the control group on the third day. However, significant differences between the two groups emerged after the 10th and 30th days of theophylline administration, suggesting a delayed response in kidney function markers to theophylline treatment. The positive eGFR results observed 30 days post-treatment prompted further investigation. On the other hand, the positive eGFR results observed 30 days post-treatment prompted further investigation.
Previous trials and meta-analyses investigating the use of the adenosine antagonist theophylline have produced inconsistent findings, with the majority of research conducted on animal models, particularly rats (
18,
19). Some studies have investigated the protective effects of a single dose of theophylline in cases of neonatal asphyxia. Building on this evidence, we conducted the present study to assess the potential prophylactic effect of theophylline on vancomycin-induced nephrotoxicity.
Similarly, Bhatt et al. investigated the role of theophylline and aminophylline in preventing AKI in children. They found that a single dose of theophylline as prophylaxis in neonatal asphyxia significantly reduced the risk of AKI and severe kidney dysfunction (
15).
Aziz et al. demonstrated that theophylline exerts a protective effect against kidney dysfunction and reduces the risk of AKI in neonates with asphyxia. In cases of asphyxia-induced tubular hypoxemia, vasoconstriction occurs, leading to elevated adenosine levels. Similarly, vancomycin can induce renal vasoconstriction and increase adenosine levels, thereby reducing renal blood flow and decreasing the GFR. The vasoconstrictive effects of adenosine can be mitigated by adenosine antagonists, such as theophylline, which block its action (
24,
25).
Vancomycin is known to induce oxidative stress in kidney tubules, resulting in impaired mitochondrial function and disrupted tubular reabsorption. Theophylline, acting as an adenosine antagonist, has been shown to exert protective effects against this oxidative stress and renal vasoconstriction (
26). While our study was not designed to elucidate the precise mechanism, the observed renoprotection is consistent with the proposed pathways of adenosine antagonism and antioxidant activity, as cited in previous literature (
3,
13,
15). Future studies should include biomarkers for oxidative stress and renal blood flow to directly test these hypotheses.
Wu et al. emphasized the antioxidant properties of theophylline and theobromine, underscoring their potential to mitigate oxidative stress. Numerous studies have corroborated the ability of these compounds to reduce the production of ROS, further supporting their therapeutic benefits (
16). Similarly, our results suggest that theophylline demonstrates antioxidant properties and may be effective in mitigating vancomycin-induced nephrotoxicity. In a systematic review, Bagshaw and Ghali investigated the role of theophylline in preventing CIN and identified evidence supporting its potential efficacy in reducing CIN, particularly in moderate- to high-risk patients undergoing coronary angiography or angioplasty (
3). The pathophysiology of CIN involves hypoxic injury to the renal medulla, driven by three interconnected mechanisms: The hemodynamic effects of contrast media (CM), the production of ROS and free radicals, and the direct cytotoxic effects of CM molecules on tubular cells (
27). Notably, the mechanisms underlying CIN and vancomycin-induced nephrotoxicity exhibit significant similarities, and the protective role of theophylline in both conditions is well-documented.
In our study, the control group demonstrated a progressive increase in BUN and microalbumin levels, along with a decline in eGFR over time. In contrast, the theophylline treatment group exhibited significant improvements in these parameters throughout the 30-day observation period (P < 0.05).
5.1. Limitations
This study has several limitations that warrant consideration. The primary limitation is the small sample size, which restricts the generalizability of the findings and underscores the need for further validation through larger, more robust clinical trials. These trials should prioritize clinically relevant outcomes such as KDIGO-defined AKI to better elucidate theophylline's potential in preventing vancomycin-induced AKI. Additionally, the clinical safety of theophylline across various dosing regimens requires comprehensive evaluation before any reconsideration of its use in clinical practice. Another significant limitation was the inability to measure vancomycin and theophylline levels at this center, which could have provided valuable insights into their pharmacokinetic interactions and potential dose-response relationships. We have now explicitly stated the lack of pharmacokinetic monitoring as a major limitation in the Discussion. Furthermore, the study did not assess the ratio of microalbumin to creatinine, a more sensitive and reliable index for detecting early kidney injury. Although microalbumin levels decreased in the intervention group, they remained within the normal range, limiting the ability to draw definitive conclusions about theophylline's renoprotective effects. The clinical significance of the observed biomarker changes therefore remains uncertain. Furthermore, the single-blind design where clinicians were not blinded could have introduced potential for performance bias, although outcome assessors were blinded. Although an ITT analysis supported our findings, the replacement of dropouts in the per-protocol analysis is a methodological limitation that may introduce bias. These limitations highlight the need for more rigorous and detailed investigations in future studies. These findings should be interpreted as hypothesis-generating and require confirmation in larger, independently conducted RCTs with pharmacokinetic monitoring and clinical renal endpoints.
5.2. Conclusions
In conclusion, the findings from this preliminary trial suggest that theophylline may hold promise in modulating surrogate biomarkers of renal function and injury during vancomycin therapy. However, the clinical relevance of these biomarker changes is not established, as values remained within normal limits and no formal AKI endpoint was used. Further research with more robust designs, including standardized AKI definitions, pharmacokinetic monitoring, and clinical endpoints, is essential to confirm these results and definitively assess its clinical applicability.