1. Background
According to the US preventive health service, chronic kidney disease (CKD) is defined as decreased kidney function, with size-adjusted estimated glomerular filtration rate (eGFR/1.73 m2) < 60 mL/min, or as damage that persists for at least three months (1). The eventual outcome of CKD is end-stage renal disease (ESRD). ESRD is defined as irremediable reduction in kidney function, and renal replacement therapy is required to save the patient’s life. Increasing numbers of patients with ESRD indicate that it is a growing public health problem (2). “According to the report of the management center for transplantation and special diseases (MCTSD) of Iran, the total number of patients with ESRD undergoing renal replacement therapy (RRT) in 2007 was 32,686, which denotes a prevalence of 435.8 per million populations (pmp). This number is very high compared with 1997 and 2000, when the prevalence of ESRD was 137 pmp and 238 pmp, respectively. The incidence of ESRD patients also seems to be increased, from 13.82 pmp in 1997 to 49.9 pmp in 2000 and 63.8 pmp in 2006” (3).
Renal replacement therapies include three main categories: hemodialysis (HD), peritoneal dialysis (PD), and renal transplantation (RT) (2, 4). Availability, socioeconomic status and comorbid conditions may influence the selecting of one of these modalities over another (5, 6). Since renal transplantation raises the quality of life and is more cost effective than long-term dialysis, it is the preferred choice for ESRD patients (2, 7, 8).
Patient survival and graft survival are two main outcomes in renal transplantation analyses that clinicians should appraise. Graft failure is defined as either returning to dialysis or death with a functioning graft (9). The rate of mortality after renal transplantation for patients with ESRD is decreasing. However, their survival remains lower than that of the general population (7).
Significant improvements in patient survival over the last three decades have been made. Current global estimates are 95% and 90% survival at 1 and 5 years, respectively (10). In spite of the many efforts to improve survival of renal grafts, numerous patients still experience graft failure. In general, one- and five-year allograft survival rates are 0.82 and 0.63 in Iran (7).
The factors influencing patient and graft survival are still not completely understood (10). Male gender, older age of recipient, diabetes, hypertension, CMV infection, and cigarette smoking have been suggested in some studies as negative determinants of patient survival. In other studies, many variables are shown to contribute to survival or rejection of graft, such as donor source, anemia after transplantation, age, gender, serum creatinine level, blood group, Rh type, waiting time for transplant, duration of hospitalization, vascular complications and acute rejection (11-19).
In most medical studies, biomarkers are longitudinally measured to check patient status along with time-to-event data. For patients with renal transplantation, time to graft failure is a major clinical event of interest, and serum creatinine is the simplest biomarker routinely measured to manage kidney transplant recipients. Longitudinal biomarkers and time to graft failure are typically correlated, where both types of data are associated through unobserved random effects.
Because these processes are correlated, the use of independent models may lead to biased estimates (20-22). To consider this association, the proportional hazard Cox model is not useful and the time-dependent Cox model also fails to correctly handle an endogenous variable (23, 24). Joint models of survival and longitudinal nonsurvival data take into account the dependence between both processes and the resulting estimates have reduced standard errors. Thus, with more accurate parameter estimates, valid inferences concerning the effect of covariates on the longitudinal and survival processes can be obtained.
2. Objectives
The aim of this study is to investigate the etiological role of recipient and donor characteristics on serum creatinine changes within the follow-up period and/or graft failure risk.
3. Patients and Methods
This retrospective cohort study was intended to consider graft failure in all patients (461 cases) who received kidney transplantation in Baqiyatallah transplant center, Baqiyatallah hospital, Tehran, Iran, during April 2005 through December 2008. The studied variables compromised donor’s and recipient’s age, gender, blood group, history of dialysis therapy before transplantation, history of diabetes, donor source, serum creatinine level at baseline and at every visit (baseline, 15 days after transplant, one month after transplant, 3 months after transplant, 6 months after transplant, 9 months after transplant, and 12 months after transplant). All data were collected from patients’ files.
3.1. Statistical Analysis
Joint modeling of survival and a continuous longitudinal nonsurvival data with shared parameters (random effect) was used in this study. It is commonly found in the collection of medical longitudinal data that both repeated measures and time-to-event data are collected. In our research, serum creatinine levels were measured longitudinally over time for each patient; time of graft failure was also of interest.
Longitudinal trajectories of serum creatinine levels as a biomarker may influence time to graft failure. As mentioned above, separate analyses of survival and longitudinal nonsurvival data may lead to biased estimates.
To provide valid and efficient results, all information from the survival and longitudinal process are incorporated in a joint model framework simultaneously. Assessing how the biomarker trajectories over time influence the risk of the event is the basic goal of joint analysis. To model both survival and longitudinal nonsurvival data simultaneously, the joint model links two processes by unobserved random effects through the use of a shared parameter. The linear mixed effects model and the Cox proportional hazard model were applied for modeling the longitudinal serum creatinine levels and the event process, respectively (25).
Covariates included in the joint model are as follows: gender, age, history of dialysis therapy before transplantation, history of diabetes, donor source, serum creatinine level at baseline and in every visit (baseline, 15 days after transplant, one month after transplant, 3 months after transplant, 6 months after transplant, 9 months after transplant, and 12 months after transplant).
The JM package in R version 3.2.2 was used to implement the joint model. A P-value of less than 0.05 was considered to be statistically significant (26).
4. Results
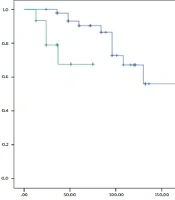
A total of 461 patients receiving transplants were studied. Demographic characteristics of the patients are presented in Table 1. Patients were 41.80 ± 13.40 years of age at transplantation time and the mean follow-up time was 6.80 months. Table 2 shows the results of the fitted joint model.
Table 1. Baseline Characteristics of 461 Transplanted Patients
| Variable | Patients (n = 461) | |
|---|---|---|
| Mean ± SD | No. (%) | |
| Recipient age (years) | 41.80 ± 13.04 | - |
| Recipient body mass index (kg/m2) | 23.17 ± 4.13 | - |
| Donor age (years) | 28.36 ± 5.00 | - |
| Recipient men | - | 310 (67.20) |
| History of diabetes | - | 92 (19.95) |
| Donor men | - | 386 (83.70) |
| Living donor | - | 405 (97.60) |
| History of dialysis | - | 387 (83.90) |
| Graft failure | - | 343 (74.40) |
Table 2. Results of the Joint Modeling Analysis
| Variable | Coefficient | 95% CI | P Value |
|---|---|---|---|
| Longitudinal sub-model | |||
| Intercepta | 4.99 | (4.33, 5.51) | < 0.001 |
| Timea | - 0.23 | (- 0.29, - 0.17) | < 0.001 |
| Recipient age (years)a | - 0.008 | (- 0.01, - 0.0001) | 0.04 |
| Recipient body mass index | 0.002 | (- 0.009, 0.004) | 0.54 |
| Recipient female | - 0.22 | (- 0.59, 0.10) | 0.30 |
| History of dialysisa | 0.37 | (0.01, 0.71) | 0.03 |
| Survival sub-model | Hazard Ratio | ||
| Serum creatininea | 4.33 | (3.02, 5.71) | < 0.001 |
| Recipient age (years) | 1.03 | (0.99, 1.07) | 0.10 |
| Recipient female | 2.91 | (0.58, 4.5) | 0.45 |
| Living donora | 2.52 | (1.68, 3.86) | < 0.001 |
| History of dialysisa | 0.18 | (0.04, 0.92) | 0.02 |
| History of diabetes | 1.13 | (0.84, 1.49) | 0.43 |
Abberivation: CI, confidence interval.
aStatistically significant at 0.05 level.
4.1. Risk Factors for Serum Creatinine Levels
A significant linear decreasing trend was seen for creatinine values over time (P < 0.001). Age and history of dialysis were associated with creatinine values. Female patients had a lower mean of serum creatinine levels (P = 0.3). Although it is not statistically significant, recipient’s body mass index (BMI) is related to higher serum creatinine levels over time.
4.2. Risk Factors for Time to Graft Failure
There was no significant difference in history of diabetes (HR = 1.13, P = 0.43) and patient’s age (HR = 1.03, P = 0.1) in hazards of graft failure in the joint model. Patients with living kidney had more hazards of graft failure than patients with deceased kidney (HR = 2.52, P < 0.001). There is a nonsignificant difference between male and female patients in hazard of graft failure (HR = 2.91, P = 0.45). In addition, the significant model association parameter revealed a positive correlation between serum creatinine levels and graft failure (HR = 4.33, P < 0.001), which means that the graft failure is more likely to happen in patients with higher serum creatinine levels.
5. Discussion
Recently, a high rate of ESRD incidence has been reported in Iran (3, 27). The rising incidence of ESRD in Iran makes it an important medical concern, as well as a social and economic problem (1, 3, 28). Progression assessment of renal disease by monitoring kidney function for patients with renal transplantation is imperative. Blood urea nitrogen (BUN), serum creatinine (Cr) and estimated glomerular filtration rate (eGFR) are the three main factors measured repeatedly. Monitoring these biomarkers after transplantation helps to ensure that no signs of renal failure due to graft rejection are present. Demographic and physiologic features of patients undergoing transplantation may influence these biomarkers. Serum creatinine levels are needed to ensure an accurate evaluation of kidney function (29). This study was carried out in an effort to assess the prognostic factors of graft failure and its relation with trajectories of serum creatinine levels.
We proposed a joint model for survival and longitudinal nonsurvival data, allowing each process to be correctly modeled and their relationship quantified while avoiding the possible bias observed when the Cox model or mixed model are used separately (25, 30). This suitable model enhances the clinical message with respect to methodological concepts because (1) the whole serum creatinine trajectory is considered, (2) graft failure risk is adjusted on serum creatinine change, and (3) serum creatinine changes and graft failure risk relationship is quantified.
Joint analysis of biomarker trajectories and survival data allows the examination of whether changes in longitudinal serum creatinine levels over time are associated with graft failure or not. The study showed significant effect of history of diabetes and serum creatinine level related to hazard of graft failure. However, the results of our study showed that the serum creatinine levels and its increase can also inform the hazard of graft failure.
In general, there is agreement between some studies in the field of nephrology about the role of serum creatinine levels in experiencing graft failure after renal transplantation (31, 32). Serum creatinine is a well-known biomarker for renal function, and its values after transplantation are an important indicator of graft status. Thus, the longitudinal serum creatinine values could be used to predict graft failure.
To monitor the outcome of the transplantation, regular measurements of serum creatinine levels in RRT patients is a useful tool. The main advantages of this study were investigating the inflectional factors on both survival and longitudinal nonsurvival outcomes and evaluating the dependence between serum creatinine levels and graft failure through the joint model simultaneously. Thus, the pattern of serum creatinine levels can be understood better. According to the joint model results, history of dialysis and history of diabetes were positively associated with serum creatinine levels. There are few studies focused on the affective factors on the serum creatinine levels over time (29).
The current study findings from the longitudinal submodel regarding time, age and gender are in general agreement with published data (29). A statistically significant relationship between age and serum creatinine levels were seen in some reports (29, 33). Additionally, the findings in this study showed that history of dialysis was associated with serum creatinine trajectories, indicating a positive association between dialysis history and serum creatinine levels.
This study used a joint model to simultaneously consider the two processes in a shared random framework. The major finding of this study is that a one unit increase in serum creatinine level suggests an increased risk of graft failure up to four times. Furthermore, serum creatinine has a slow rate of decrease over time (β = - 0.23, p < 0.001). Thus, frequent measurement of serum creatinine levels to monitor the outcome of renal transplantation is very important.
Physicians should pay particular attention to elderly recipients, female patients, and patients with history of diabetes. For these patients, monitoring serum creatinine could be useful to evaluate the risk of graft failure.
5.1. Limitation
One limitation of this study was that there were some missing values in the longitudinal assessment of serum creatinine levels. Thus, we were forced to ignore such patients.