1. Background
2. Objectives
3. Patients and Methods
3.1. Population
3.2. Histological and Immunochemistry Studies
3.3. Statistical Analysis
3.4. Ethics
4. Results
| Simple Mole | GTN | P Value | |
|---|---|---|---|
| Final diagnosis | 28 | 30 | |
| Primary diagnosis | 0.00 | ||
| Complete mole | 18 | 28 | |
| Partial mole | 10 | 2 | |
| Age, mean ± SD | 26.2 ± 7.4 | 31.9 ± 9.0 | 0.01 |
| Gestational age, mean ± SD | 11.3 ± 4.0 | 11 ± 3.2 | 0.79 |
| Gravity number, mean ± SD | 1.7 ± 1.5 | 3.1 ± 2.3 | |
| Parity number, mean ± SD | 0.5 ± 1.5 | 1.9 ± 2.2 |
Abbreviation: GTN, Gestational Trophoblastic Neoplasia.
aP value < 0.05 considered significant.
| GTN | Simple Mole | P Value | Complete Mole | Partial Mole | P Value | |
|---|---|---|---|---|---|---|
| P53 Cytotrophobalsts | 41.6 ± 25.4 | 5.3 ± 9.3 | 0.000 | 27.9 ± 26.7 | 9.0 ± 21.1 | 0.007 |
| P53 Syncytiotrophoblasts | 19.3 ± 18.8 | 1.2 ± 1.1 | 0.000 | 12.1 ± 17.1 | 4.0 ± 9.8 | 0.027 |
| C-erbB-2 Cytotrophobalsts | 18.4 ± 26.4 | 2.5 ± 8.6 | 0.000 | 11.7 ± 21.6 | 6.2 ± 20.1 | 0.053 |
| C-erbB-2 Syncytiotrophoblasts | 5.4 ± 14.5 | 1.6 ± 5.4 | 0.508 | 4.0 ± 12.1 | 1.6 ± 5.7 | 0.437 |
Abbreviation: GTN, Gestational Trophoblastic Neoplasia.
aP value < 0.05 considered significant.
bValues are expressed as mean (SD).
")
(A), Nuclear cytotrophoblasts and syncytiotrophoblasts immunoreactivity (× 100) (B), Negative immunoreactivity of syncytiotrophoblasts and positive nuclear immunoreactivity of more than 80% of trophoblasts (C), positive cytoplasmic immunoreactivity of trophoblasts for c-erbB-2 with fairly no staining of syncytiotrophoblasts (D), Hydropic villi with trophoblastic vacuolization and positive immunoreactivity in about 80% of trophoblasts (× 40)(E), (× 100) (F).
| P53 Cytotrophoblast | P53 Syncytiotrophoblast | C-erbB-2 Cytotrophoblasts | C-erbB-2 Syncytiotrophoblast | |||||
|---|---|---|---|---|---|---|---|---|
| SMP | GTN | SMP | GTN | SMP | GTN | SMP | GTN | |
| Negative | 1 (3.8) | 1 (3.3) | 6 (23.1) | 2 (6.9) | 23 (88.5) | 7 (23.3) | 23 (88.5) | 25 (83.3) |
| + | 22 (84.6) | 3 (10) | 20 (76.9) | 11 (37.9) | 1 (3.8) | 12 (40) | 1 (3.8) | 1 (3.3) |
| ++ | 3 (11.5) | 17 (56.7) | 0 (0) | 15 (51.7) | 2 (7.7) | 7 (23.3) | 2 (7.7) | 3 (10) |
| +++ | 0 (0) | 9 (30) | 0 (0) | 1 (3.4) | 0 (0) | 4 (13.3) | 0 (0) | 1 (3.3) |
| P Value | 0.000 | 0.000 | 0.000 | 1.000 | ||||
Abbreviations: GTN, Gestational Trophoblastic Neoplasia; SMP, Simple Molar Pregnancy.
aFor p53 marker, we applied 0 for no stained cells, + for staining of less than 10% of cells, ++ for 10 to 50% of cells, +++ for staining in more than 50% of cells. To score c-erbB-2 staining intensity we used negative as of no or less than 10% of cells’ membranes stained, + for faint membranous staining in more than 10% of cells, ++ for weak to moderate complete membranous staining in more than 10% of cells and evaluate +++ as strong, for complete membranous staining in more than 30% of cells, results of chi-square test.
bP value < 0.05 considered significant.
cValues are expressed as No. (%).

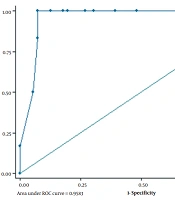
For p53 and c-erbB-2 markers among cytotrophoblasts and syncytiotrophoblasts in molar tissue to estimate their risk to GTN transformation.The test result variable(s): p53Cyto, p53Syncyto, Her2cyto, Her2Syncyto has at least one tie between the positive actual state group and the negative actual state group. Statistics may be biased. a, Under the nonparametric assumption. b, Null hypothesis, true area = 0.5.
| P53 Cytotrophoblasts, (%) | P53 Syncytiotrophoblast, (%) | C-erbB-2 Cytotrophoblasts, (%) | |
|---|---|---|---|
| Cut off for percentage of cells with positive immunostaining | 5.5 | 2.5 | 12.5 |
| Positive predictive value | 90 | 88.8 | 88.4 |
| Negative predictive value | 92 | 82.1 | 76.6 |