



1. Background
International marriage and migration have recently abruptly increased in South Korea (in the latter part of this paper, it will be marked as “Korea”). The term multicultural family was set by the Multicultural Families Support Act in Korea, as one comprising an immigrant or person who has acquired Korean nationality pursuant to the Korean Nationality Act (including migrant workers, international marriage, North Korean refugees, and Korean - Chinese people) and their families (1, 2). With the recent increases in international marriages and migrant workers, there were 318917 multicultural families in 2017, of these, 115876 families were composed of marriage between Koreans and migrants, and 75957 were between Koreans and naturalized Koreans (3). The increased number of multicultural families has led to a significant increase in children with multicultural backgrounds in Korea. Multicultural birth cases (18440) accounted for 5.15% of all Korean birth cases (357771) in 2017 (4). Therefore, the proportion of adolescents with multicultural background will be abruptly increased in the near future. Thus, the health problems, including mental health, of multicultural adolescents will become an important social issue.
In this study, we explore the differences in adolescents’ mental health between multicultural and monocultural families based on their self-reported stress and depressive mood, suicidal thinking, suicidal plans, and suicide attempts. The suicide rate in Korea ranked in the highest level among Organization for Economic Cooperation and Development (OECD) countries and 2.4 times higher than the average rate of other OECD countries in 2013 (5, 6). And despite the national suicide prevention program implemented in the early 2000s, suicide rate of adolescents in Korea has continuously increased, although it has decreased in other OECD countries (6). The most common cause of death in Korean adolescents was suicide in 2016 (5). Adolescents with multicultural backgrounds, who have more stress factors than those with monocultural backgrounds, are likely to be more vulnerable to suicide. Because the interrelationships of stress, drinking, and smoking in adolescents are well known, we aimed to investigate whether health behaviors such as smoking and drinking also differed between the two groups, as well as to determine which factors influence mental health. Our hypotheses are as follows. First, multicultural adolescents have more risk behaviors, such as skipping breakfast, smoking, and drinking, than monocultural adolescents in Korea. Second, multicultural adolescents have a higher rate of mental health problems than those with a monocultural background. Third, the relationship between multicultural status and mental health is dependent on the degree of risk behaviors.
2. Methods
2.1. Study Design and Data Collection
The Korean Ministry of Education, Ministry of Health and Welfare, and Centers for Disease Control and Prevention conducted The Korean Youth Risk Behavior Web-Based Survey (KYRBS) in 2005 with the goal of understanding and monitoring the health-related status of adolescents in Korea. The KYRBS is a cross-sectional, self-reported web-based survey conducted annually in a nationally representative sample of Korean adolescents aged 13 - 18 years, and it consists of 123 questions. To ensure sample representativeness, the KYRBS utilizes proportional allocation methods, and the participants are drawn as stratified multistage clustered samples from 400 middle and 400 high schools in Korea, comprising 44 locations. Student participation in the KYRBS is voluntary and answering the questionnaire was guaranteed anonymity completing at a school computer laboratory. The purpose of the KYRBS is to assess health-risk behaviors, including dietary behaviors, such as skipping breakfast and consuming fruit juices, soft drinks, drinks with a high caffeine content, fast food, noodles, and snacks. The KYRBS also assesses hygiene status, obesity levels, weight control efforts, physical activity, time spent using smartphones, consumption of alcohol, use of tobacco products, and causes of injury. Finally, the KYRBS assesses mental health status by asking about symptoms of depressive mood, suicide ideation, and suicide attempts. In the present study, we used documents publicly available from the 13th KYRBS published in 2017. Among adolescents in the sample class, we excluded participants with absenteeism (absence without permission), those with special educational needs (such as development disabilities), and those with dyslexia. A multicultural family was defined as a response of “No” to the following question: “Were your father and mother both born in Korea?” (no indicating at least one parent born in a foreign country). A monocultural family was defined as a response of “Yes” to the same question (yes indicating both parents born in Korea). Additional questions about the parents’ birthplaces were included as follows in regular order: China (Korean - Chinese who were ethnic Koreans born in China), China (Han and other ethnicities), North Korea, Vietnam, the Philippines, Japan, and so on. We considered Korean - Chinese families as multicultural, but excluded adolescents from North Korean defectors from this study because they might have experienced emotional trauma during defection.
2.2. Evaluation Indices
2.2.1. Demographic Characteristics
Age, sex, school grade, height, weight, parent educational status, and behaviors related to food intake, including fruit intake, carbonated drinks, and fast food, time of physical exercise and effort for weight control were also surveyed. Responses to questions about scholastic achievement and family socioeconomic status were divided into 5 categories as follows: high, middle-high, middle, middle-low, and low. Division according to the smartphone average use time during weekdays and weekend were established into two groups; less and much than the average time.
2.2.2. Eating and Diet Behaviors
Based on convention in the current literature (7), subjects engaging in any of the following behaviors were classified as displaying extreme weight control behavior (EWCB): using diet pills, laxatives, or diuretics, and inducing emesis after meals. Likewise, subjects who fasted, skipped meals, ate very little amounts of food, or utilized diet food substitutes, such as powdered drinks, or smoked cigarettes for the purpose of losing weight or keeping from gaining weight were considered to be engaging in unhealthy weight control behaviors (UWCB). The KYRBS contains specific questions related to EWCB and UWCB. Frequency of breakfast consumption was assessed with the question, “During the past 7 days, how many days did you eat breakfast?” with allowed responses of “never, 1, 2, 3, 4, 5, 6, or 7 days.” Those who indicated they ate breakfast less than 2 days per week were considered to regularly skip breakfast and were called “breakfast skippers.”
2.2.3. Risk Behaviors
In KYRBS, risk behaviors consisted of drinking alcohol, smoking, and drug use. Participants who had consumed at least one alcoholic beverage during their lifetime were defined as having drinking experience, and those who had consumed at least one alcoholic beverage within the past 30 days were defined as current drinkers. Smoking experience or lifetime smoking was also defined as having experienced smoking at least more than a puff of cigarette ever in life, and the current smokers were defined as ones having smoked at least once within the last 30 days. The variables related to drug use were assessed by the following question: “Have you ever used any kind of drugs, such as butane gas, glue, stimulants, amphetamine, narcotics, a lot of cough medication, or a tranquilizer for the purpose of changing your mood, experiencing hallucinations, or excessive diet?”
2.2.4. Depressive Mood, Suicide Ideation, and Suicide Attempts
Experience with a depressive mood was defined as a participant’s reporting feeling sad or desperate to a degree that caused them to stop their usual activities for two weeks within the most recent 12 months. The questions about both suicide ideation and suicidal attempts included, “Have you ever thought about killing yourself?” and “Have you ever tried to kill yourself?” Response options included “No,” “Yes, within the recent 12 months,” and “Yes, I tried to commit suicide within the last 12 months.” Repetition of depressive mood, suicide ideation, and suicide attempts were not assessed. The frequency of perceived stress was assessed with the following question: “How often do you feel stress?” And this was scored on a 5-point scale (1 = very often, 2 = often, 3 = occasionally, 4 = rarely, 5 = never), and responses of 1 or 2 were defined as stressful. The state of perceived healthiness was assessed with the following question: “What do you usually think about your health condition?” It was scored on a 5-point scale in the same way (1 = very healthy, 2 = healthy, 3 = average, 4 = unhealthy, 5 = very unhealthy), and responses of 4 or 5 were defined as unhealthy.
2.3. Statistical Analysis
We conducted statistical analysis using the Statistical Package for the Social Sciences (SPSS) version 21.0 software (SPSS Inc., Chicago, IL, USA). The characteristics of monocultural and multicultural adolescents were compared using crosstabs analysis. Additionally, we used independent t-tests for the continuous variables. We carried out multiple logistic regression analysis in order to identify the associated risk factors for depressive mood and suicidal attempts in multicultural and monocultural adolescents. For all analyses, we considered a P value of < 0.05 to be statistically significant.
2.4. Ethics Statement
The approval of this online statistical research was achieved by the Institutional Review Board (IRB) of the Centers for Disease Control and Prevention, and we used the publicly available documents for academic purposes. The study protocol was reviewed and approved by the IRB of Samsung Changwon Hospital (IRB No. 2018-11-001). The informed consent requirement for our study was waived by the IRB of Samsung Changwon Hospital.
3. Results
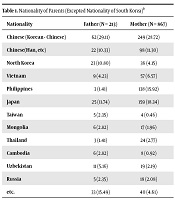
Among the targeted 64991 adolescents in 400 schools, 62276 (response rate 95.8%) in 799 schools ultimately participated in this survey. We excluded the 52 adolescents from the families of North Korean defectors and 4172 who lacked responses to the question related to their parents’ birthplace. Table 1 shows the parents’ birthplaces, and Table 2 shows the general characteristics of the 58052 who were finally included in this survey. The multicultural adolescents made up 1.56% of the participants, with female predominance and, compared with the monocultural adolescents, they were younger, shorter, and more slender, and had lower educational status of parents, lower self-recognized academic performance, lower economic status and used smartphone longer time. The average use time of smartphone was 205 minutes during weekdays and 328 minutes in weekend. In the health-related behaviors, multicultural adolescents ate less fruit and fast-food and ate more convenience store food, exercised less regularly, and more frequently displayed EWCB and UHCB for controlling their weight than monocultural adolescents (Table 3). Ever experiencing smoking and drinking rates were higher in the monocultural adolescents; however, daily smoking and drinking rates were higher in the multicultural adolescents. Multicultural adolescents reported feeling more stress and subjective unhealthiness than monocultural adolescents. Depressive mood was not statistically significantly higher, but suicidal ideation, plans, and attempts were higher in the multicultural adolescents. The experience rate of suicidal attempts within last 12 months among multicultural adolescents was 6.06%, which was approximately three times higher than those of monocultural adolescents (Table 3). When we considered daily smoking and drinking, lower economic status, poorer self-recognized academic performance, and much use than average time as independent variables, they affected depressive mood, but multicultural background itself did not affect depressive mood (Table 4). The highest odds ratio was daily drinking in this group at 3.18. These variables, including multicultural background, also affected suicidal attempts, and the highest odds ratio was multicultural background at 9.50 (Table 5).
| Nationality | Father (N = 213) | Mother (N = 867) |
|---|---|---|
| Chinese (Korean - Chinese) | 62 (29.11) | 249 (28.72) |
| Chinese(Han, etc) | 22 (10.33) | 98 (11.30) |
| North Korea | 23 (10.80) | 36 (4.15) |
| Vietnam | 9 (4.23) | 57 (6.57) |
| Philippines | 3 (1.41) | 138 (15.92) |
| Japan | 25 (11.74) | 159 (18.34) |
| Taiwan | 5 (2.35) | 4 (0.46) |
| Mongolia | 6 (2.82) | 17 (1.96) |
| Thailand | 3 (1.41) | 24 (2.77) |
| Cambodia | 6 (2.82) | 8 (0.92) |
| Uzbekistan | 11 (5.16) | 19 (2.19) |
| Russia | 5 (2.35) | 18 (2.08) |
| etc. | 33 (15.49) | 40 (4.61) |
Nationality of Parents (Excepted Nationality of South Korea)a
| Characteristic | Total (n = 58052) | Multicultural (n = 904) | Monocultural (n = 57148) | P Value |
|---|---|---|---|---|
| Sex (weighted %) | 0.030 | |||
| Male | 29409 (51.92) | 415 (47.55) | 28994 (51.98) | |
| Female | 28643 (48.08) | 489 (52.45) | 28154 (48.02) | |
| Age (weighted mean ± SE) | 15.12 ± 0.03 | 14.83 ± 0.07 | 15.12 ± 0.03 | < 0.001 |
| Grade | < 0.001 | |||
| Middle school 1st grade | 9641 (15.07) | 190 (18.88) | 9451 (15.02) | |
| Middle school 2nd grade | 9763 (15.56) | 184 (18.06) | 9579 (15.52) | |
| Middle school 3rd grade | 9599 (15.05) | 157 (16.22) | 9442 (15.04) | |
| High school 1st grade | 9501 (17.13) | 147 (18.19) | 9354 (17.12) | |
| High school 2nd grade | 10009 (18.88) | 120 (15.06) | 9889 (18.93) | |
| High school 3rd grade | 9539 (18.31) | 106 (13.58) | 9433 (18.38) | |
| Height (weighted mean ± SE) | 165.57 ± 0.18 | 163.25 ± 0.36 | 165.60 ± 0.18 | < 0.001 |
| Weight (weighted mean ± SE) | 58.52 ± 0.20 | 56.42 ± 0.49 | 58.54 ± 0.20 | < 0.001 |
| Body mass index (weighted mean ± SE) | 21.21 ± 0.03 | 21.04 ± 0.14 | 21.21 ± 0.03 | 0.219 |
| Educational status of father | < 0.001 | |||
| Middle school | 1076 (2.14) | 101 (16.39) | 975 (1.99) | |
| High school | 15296 (31.31) | 276 (47.70) | 15020 (31.13) | |
| College | 31065 (66.55) | 192 (35.91) | 30873 (66.88) | |
| Educational status of mother | < 0.001 | |||
| Middle school | 916 (1.79) | 54 (10.53) | 862 (1.70) | |
| High school | 18643 (38.45) | 216 (36.15) | 18427 (38.47) | |
| College | 28400 (59.76) | 313 (53.33) | 28087 (59.83) | |
| Self-recognized academic performance | < 0.001 | |||
| Poor | 5349 (9.39) | 123 (14.69) | 5226 (9.32) | |
| Below average | 12668 (21.86) | 250 (27.30) | 12418 (21.78) | |
| Average | 16766 (28.96) | 260 (28.23) | 16506 (28.97) | |
| Above average | 15248 (26.09) | 191 (19.91) | 15057 (26.17) | |
| Excellent | 8021 (13.70) | 80 (9.88) | 7941 (13.76) | |
| Economic status | < 0.001 | |||
| Low | 1128 (1.95) | 56 (6.91) | 1072 (1.89) | |
| Low-middle | 6229 (10.56) | 186 (20.17) | 6043 (10.43) | |
| Middle | 26823 (45.86) | 433 (46.57) | 26390 (45.85) | |
| Upper-middle | 17522 (30.51) | 162 (18.09) | 17360 (30.68) | |
| High | 6283 (11.12) | 67 (8.26) | 6283 (11.16) | |
| Smartphone usagea | < 0.001 | |||
| Less than average | 37885 (74.06) | 480 (65.41) | 37405 (74.88) | |
| More than average | 13267 (25.94) | 280 (34.59) | 12987 (25.12) |
General Characteristics of Participants
| Multicultural (n = 904) | Monocultural (n = 57148) | P Value | |
|---|---|---|---|
| Regular breakfast feeding | 758 (83.53) | 47338 (82.75) | 0.568 |
| Fruit intake | 797 (88.30) | 51665 (90.39) | 0.049 |
| Carbonated drinks | 709 (79.02) | 45075 (78.97) | 0.971 |
| High-caffeinated drinks | 239 (26.48) | 13370 (23.51) | 0.066 |
| Sweet drink | 786 (87.18) | 50025 (87.52) | 0.784 |
| Fast-food | 672 (74.66) | 45676 (80.49) | < 0.001 |
| Instant noodles | 677 (74.97) | 44396 (77.59) | 0.107 |
| Snacks | 763 (83.65) | 47854 (83.48) | 0.911 |
| Convenience store food | 606 (66.87) | 36765 (64.74) | 0.027 |
| Physical for more than 60 minutes | 597 (66.85) | 36640 (63.69) | 0.098 |
| Vigorous physical | 689 (76.67) | 43669 (75.85) | 0.595 |
| Muscular exercise | 462 (51.31) | 29626 (51.31) | 0.999 |
| Walking exercise | 855 (95.29) | 54385 (95.34) | 0.950 |
| Weight control status | 485 (52.54) | 30024 (51.96) | 0.737 |
| Weight control method | |||
| Regular exercise | 329 (66.99) | 21863 (72.39) | 0.018 |
| Weight-loss drug (obtain a drug on a doctor’s prescription) | 13 (2.43) | 506 (1.67) | 0.207 |
| Weight-loss drug (not obtain a drug on a doctor’s prescription) | 21 (4.33) | 737 (2.40) | 0.016 |
| Vomiting after meals | 19 (3.77) | 800 (2.61) | 0.179 |
| Laxative or diuretic | 12 (2.20) | 522 (1.71) | 0.440 |
| Fast for more than 24 hours | 49 (9.86) | 2712 (8.84) | 0.490 |
| Reduction in food intake | 305 (61.28) | 19999 (66.70) | 0.026 |
| One food diet | 48 (9.73) | 2122 (6.86) | 0.025 |
| Chinese medicine | 21 (4.74) | 1740 (5.75) | 0.427 |
| Diet foods | 51 (10.88) | 2403 (8.00) | 0.036 |
| Experience of smoking | 782 (84.22) | 50097 (87.00) | 0.044 |
| Current smoking | 68 (57.42) | 3131 (44.86) | 0.007 |
| Daily smoking status | 16 (2.33) | 120 (0.22) | < 0.001 |
| Experience of drinking | 279 (34.15) | 22071 (39.58) | 0.004 |
| Current drinking | 110 (41.11) | 8568 (39.52) | 0.625 |
| Daily drinking status | 35 (4.81) | 1388 (2.61) | < 0.001 |
| Stress | 0.005 | ||
| Very high | 115 (13.87) | 5744 (9.93) | |
| High | 233 (25.00) | 15338 (26.83) | |
| Middle | 353 (38.93) | 24290 (42.91) | |
| Low | 160 (17.54) | 9459 (16.34) | |
| Very low | 43 (4.66) | 2317 (3.99) | |
| Subjective happiness status | < 0.001 | ||
| Very unhappiness | 20 (2.87) | 17235 (29.45) | |
| Unhappiness | 62 (7.21) | 21835 (38.33) | |
| Average | 208 (23.04) | 13837 (24.71) | |
| Happiness | 328 (35.86) | 3606 (6.35) | |
| Very happiness | 286 (31.01) | 635 (1.16) | |
| Subjective health status | < 0.001 | ||
| unhealthy | 75 (12.44) | 3464 (7.91) | |
| healthy | 615 (87.56) | 41559 (92.09) | |
| Depressive mood | 248 (27.15) | 14015 (24.59) | 0.126 |
| Suicidal ideation | 143 (16.80) | 6714 (11.68) | < 0.001 |
| Suicide plan | 54 (6.73) | 2133 (3.65) | < 0.001 |
| Suicidal attempt | 45 (6.06) | 1363 (2.34) | < 0.001 |
| Clinical therapy after suicidal attempt | 18 (45.45) | 184 (13.86) | < 0.001 |
Comparison of Health Related Behaviors and Mental State of Multicultural and Monocultural Adolescents
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | P Value | OR (95% CI) | P Value | OR (95% CI) | P Value | |
| Daily drinking status (ref: not daily) | 2.79 (1.92 - 4.07) | < 0.001 | 2.79 (1.91 - 4.07) | < 0.001 | 3.18 (2.13 - 4.74) | < 0.001 |
| Daily smoking status (ref: not daily) | 1.79 (1.57 - 2.04) | < 0.001 | 1.79 (1.57 - 2.04) | < 0.001 | 1.80 (1.58 - 2.06) | < 0.001 |
| Economic status (ref: high) | 1.12 (1.09 - 1.15) | < 0.001 | 1.12 (1.09 - 1.15) | < 0.001 | 1.12 (1.09 - 1.15) | < 0.001 |
| Academic performance (ref: excellent) | 1.15 (1.13 - 1.18) | < 0.001 | 1.15 (1.13 - 1.18) | < 0.001 | 1.15 (1.13 - 1.18) | < 0.001 |
| Smartphone usage (ref:less than average) | 1.38 (1.31 - 1.45) | < 0.001 | 1.38 (1.31 - 1.45) | < 0.001 | 1.92 (1.34 - 2.75) | < 0.001 |
| Multicultural families status (ref: monocultural) | 1.01 (0.85 - 1.20) | 0.921 | 1.84 (0.96 - 3.52) | 0.066 | ||
| Interaction terms | ||||||
| Daily drinking status * Multicultural families status | 0.33 (0.09 - 1.21) | 0.094 | ||||
| Daily smoking status * Multicultural families status | 0.91 (0.38 - 2.20) | 0.837 | ||||
| Economic status * Multicultural families status | 0.83 (0.69 - 1.01) | 0.050 | ||||
| Academic performance * Multicultural families status | 1.00 (0.87 - 1.15) | 0.970 | ||||
| Smartphone usage * Multicultural families status | 0.71 (0.50 - 1.03) | 0.069 | ||||
Factors Influencing the Depressive Mood of Adolescents
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | P Value | OR (95% CI) | P Value | OR (95% CI) | P Value | |
| Daily drinking status (ref: Not daily) | 9.51 (5.90 - 15.34) | < 0.001 | 8.63 (5.32 - 14.01) | < 0.001 | 8.44 (5.10 - 13.96) | < 0.001 |
| Daily smoking status (ref: Not daily) | 1.82 (1.41 - 2.36) | < 0.001 | 1.81 (1.39 - 2.34) | < 0.001 | 1.80 (1.38 - 2.36) | < 0.001 |
| Economic status (ref: high) | 1.11 (1.03 - 1.20) | 0.008 | 1.10 (1.02 - 1.19) | 0.014 | 1.12 (1.04 - 1.21) | 0.005 |
| Academic performance (ref: Excellent) | 1.20 (1.13 - 1.26) | < 0.001 | 1.20 (1.13 - 1.26) | < 0.001 | 1.20 (1.14 - 1.27) | < 0.001 |
| Smartphone usage (ref: less than average) | 1.75 (1.54 - 2.00) | < 0.001 | 1.76 (1.53 - 2.01) | < 0.001 | 1.19 (0.54 - 2.61) | 0.659 |
| Multicultural families status (ref: Monocultural) | 2.16 (1.53 - 3.06) | < 0.001 | 9.50 (2.84 - 31.72) | < 0.001 | ||
| Interaction terms | ||||||
| Daily drinking status * Multicultural families status | 0.92 (0.16 - 5.32) | 0.928 | ||||
| Daily smoking status * Multicultural families status | 1.08 (0.20 - 5.67) | 0.931 | ||||
| Economic status * Multicultural families status | 0.69 (0.47 - 1.02) | 0.060 | ||||
| Academic performance * Multicultural families status | 0.89 (0.64 - 1.22) | 0.462 | ||||
| Smartphone usage * Multicultural families status | 1.49 (0.67 - 3.28) | 0.325 | ||||
Factors Influencing the Suicidal Attempt of Adolescents
4. Discussion
We conducted this study to investigate the association between risk behaviors, such as smoking and drinking, and mental health problems, such as depression and suicide attempts, among adolescents from multicultural versus monocultural families in Korea using an online survey data from the 2017 KYBRS. We found that depressive mood did not significantly differ between the two groups, but suicidal behaviors were higher in the multicultural adolescents. Smoking has been shown to be a risk factor for suicide behavior among multicultural adolescents (8); however, in the current study, we found multicultural background itself to have the greatest influence on suicide attempts.
Suicide is a major public health problem for adolescents worldwide (9). It occurs throughout the lifespan and is globally the second leading cause of death among 15 - 29 year olds (5). In particular, the mental health of the offspring of immigrants and those in international marriages is a major public health concern (10-12). Several studies have shown that adolescents in multicultural families are likely to have poorer psychological well-being than those with monocultural backgrounds, such as lower self-esteem, marked life dissatisfaction, depression, and anxiety (2, 13, 14). Similar to these results, we found that youth with multicultural backgrounds displayed no difference in depressive mood; however, they had higher frequency of suicide ideation, planning, and attempts compared to those with monocultural backgrounds. Comparison of health behaviors between the two groups suggests that those in multicultural backgrounds are more likely to have a higher risk of displaying EWCB and UHCB for controlling their weight, daily alcohol consumption, and smoking compared to monocultural adolescents. These differences in health behaviors and psychological difficulties may be explained by several factors. The risk factors for suicide ideation for adolescents in monocultural families are known: residence without a family, poor perceived state of healthiness, depressive mood, high level of stress, poor perceived level of happiness, and experience of violence (8). Additionally, gender (girls), lower grades, lower economic status, depression, low sleep satisfaction, high stress, alcohol consumption, smoking, and sexual activity are the risk factors for suicide ideation in adolescents (15). However, we consider different risk factors for suicide behavior among multicultural adolescents. First, low Korean language competence, especially in reading and writing, due to lack of mutual feedback by non-fluent parents negatively influence learning and personal relationships, and this low language competence causes stress, depression, and anxiety (16). Second, differences in outward appearance from the major population, especially in a homogenous nation like Korea, may cause bullying among kids in school, and its self-recognition can lead to poor school adjustment (16). A study reported that 15.7% of teenagers with multicultural backgrounds had experienced teasing, bullying, or discrimination by their friends because of their foreign parents or for no specific reasons (17). Victimization of bullying is an important risk factor of suicide attempts among adolescents globally (18). Friends were the most common perpetrators of discrimination and the experience of ethnic discrimination was associated with depressive symptoms among multicutural adolescents in South Korea (19). Third, acculturative stress between the living-in culture and the foreign culture learned from migrant parents can make multicultural adolescents feel confused about cultural adjustment and create difficulties in communicating with their parents. Yu et al. found in a study of 164 first-generation Chinese immigrants in the United States that American orientation was strongly associated with positive psychological well-being, and moreover, American orientation was negatively associated with depressive symptoms only at mean or high levels of Chinese orientation (20). However, according to another study, the risk of suicide is higher in the second generation of migrant youth, especially in Hispanic and Asians, than in the first generation (21). Fourth, low socioeconomic status (SES) is also frequently experienced by children with multicultural backgrounds (22). Although subjective SES is a significant moderator of the association between school connectedness and psychological distress, but not between school connectedness and suicidal ideation or attempts, however, the effects of school connectedness on mental health states may be more strongly related to adolescents’ SES beliefs rather than parental education (23). Lower peer support, more family conflicts, violent experiences, and more parental noninterference are also risk factors creating vulnerabilities for adolescents with multicultural backgrounds, in addition to discrimination and prejudice against those of mixed racial heritage (2, 13). Also, consistent with our study, adolescents in multicultural families have reported that they perceived themselves as unhealthy, compared with monocultural adolescents (2). It is well known that physical health status is highly related to behavioral and psychological problems (24). In our study, multicultural adolescents ate more convenience store foods, exercised less regularly, displayed EWCB and UHCB more frequently, and had higher levels of daily drinking and smoking rates than monocultural adolescents. And they felt more stress and subjective unhealthiness. These findings indicate that the physical and mental health of multicultural adolescents should be monitored and managed.
There are several limitations to our study. First, although this study was based on a national survey, the results may have been influenced by selection or recall bias. For example, the sample was composed of students attending school with relatively lower risk of behavioral and psychological difficulties than out-of-school adolescents. And the survey did not include out-of-school adolescents, such as those who had dropped out or faced expulsion. In addition, students who attended alternative schools were not included in the survey. Had such students been included, data on suicide ideation may have differed. Second, because this study was conducted in the form of a self-response questionnaire rather than a standardized test when evaluating psychological problems, we should consider response bias of respondents. Specifically, in this format, adolescents may have believed that their answers would be linked to private and confidential information, and this may have led to erroneous reporting, decreasing response credibility. Third, our study did not measure several known risk factors associated with behavioral and psychological problems in multicultural adolescents such as fixed risk factors including family history of suicide or suicide attempts; history of adoption; parental mental health problems; lesbian, gay, bisexual, or questioning sexual orientation; transgender identification; a history of physical or sexual abuse; a previous suicide attempt; substance intoxication and substance use disorders; school violence; language fluency; and residence period in Korea (25, 26). Finally, although the number of refugees is relatively small, we should consider the effect of refugees. According to the literature, the refugees with depression were younger, more likely to be male, had lower levels of psychological social support, resilience, higher levels of alcohol problems, aggression and post-traumatic stress disorder than those without depression (27). Therefore, further research including these variables is necessary to clearly explain psychological and behavioral differences compared to monocultural adolescents. However, despite these limitations, this study has several strengths that build on the findings of previous reports of mental health status in adolescents from multicultural families. Specifically, this was a nation-wide government-directed survey with a high response rate (95.8%) that, to the best of our knowledge, included the largest number of participants (n = 58052) of any similar study, with an equal division of middle and high school students (400 schools, each) and a socioeconomically diverse sample that allows for good generalization of the results.
4.1. Conclusions
Our findings suggest that adolescents with multicultural backgrounds need much more attention regarding alcohol consumption, smoking, and suicidality problems. Therefore, more intensive education and practical prevention strategies are needed to manage risk behaviors and reduce suicide behaviors in multicultural adolescents.
